Overview of Pathological Findings in the Esophagus
|
 Diseases of the gastroesophageal junction
Diseases of the gastroesophageal junction Infections and other forms of esophagitis
Infections and other forms of esophagitis Diverticula
Diverticula Motility disorders
Motility disorders Varices
Varices Tumors
Tumors Foreign bodies and rare findings
Foreign bodies and rare findings Postoperative conditions
Postoperative conditions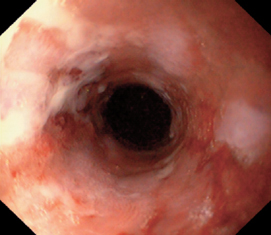
Fig. 3.1 Diseases of the gastroesophageal junction
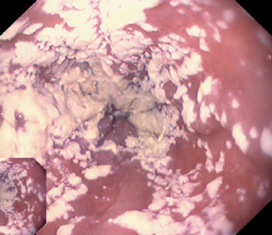
Fig. 3.2 Infections and other forms of esophagitis
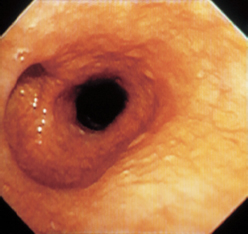
Fig. 3.3 Diverticula
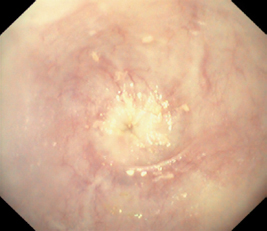
Fig. 3.4 Motility disorders

Fig. 3.5 Varices
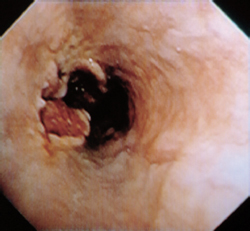
Fig. 3.6 Tumors
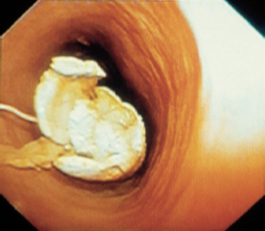
Fig. 3.7 Foreign bodies and rare findings

Fig. 3.8 Postoperative conditions
Cardial Incompetence
 Definition and Clinical Aspects
Definition and Clinical Aspects
Cardial incompetence, hiatal hernia, and gastroesophageal reflux are relatively common endoscopic findings. Often these findings are causally related to one another, but they may also occur independently. They are not consistently associated with typical clinical complaints.
Cardial incompetence is defined as absent or deficient closure of the gastric inlet in relation to the esophagus. The cause may be incompetence of the lower esophageal sphincter. A hiatal hernia can also cause impairment of gastroesophageal closure. Incompetence of the cardia is usually noted as an incidental finding in a patient who has no clinical complaints and no signs of reflux esophagitis.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Forward view
Forward view
- – Gaping gastric inlet (Fig. 3.9)
- – Gastric interior is already visible several centimeters above the cardia
- – Gaping gastric inlet (Fig. 3.9)
 Retroflexed view
Retroflexed view
- – Absence of cardial closure around the endoscope in retroflexion (Fig. 3.10)
- – Retroflexed view into the esophagus
- – Absence of cardial closure around the endoscope in retroflexion (Fig. 3.10)
 Caution: Do not pull the retroflexed tip into the esophagus.
Caution: Do not pull the retroflexed tip into the esophagus.
Differential diagnosis
 Normal finding
Normal finding
 Endoscopic artifact
Endoscopic artifact
 Examiner subjectivity
Examiner subjectivity
Checklist for endoscopic evaluation
 Closure of the cardia in forward and retroflexed views
Closure of the cardia in forward and retroflexed views
 Axial sliding hernia?
Axial sliding hernia?
 Signs of reflux esophagitis?
Signs of reflux esophagitis?
 Gastroesophageal prolapse?
Gastroesophageal prolapse?
Additional Study
 Esophageal manometry
Esophageal manometry
Comments
Since the endoscopic interpretation is highly subjective, you should be careful when making a diagnosis of cardial incompetence.
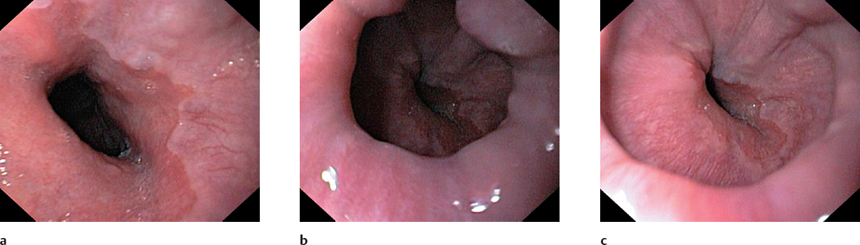
Fig. 3.9 Gastroesophageal junction a–c Observation of the gastroesophageal junction for approximately 30 seconds. Notice the absence of sphincter closure
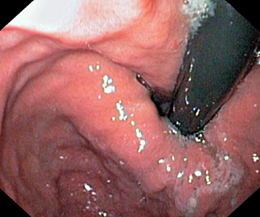
Fig. 3.10 Cardial incompetence. Retroflexed view. Note the failure of the cardia to close snugly around the endoscope (cf. p. 47)
Hiatal Hernia: Axial Sliding Hernia
 Definitions and Clinical Aspects
Definitions and Clinical Aspects
Hiatal hernia is defined as the persistent or recurrent herniation of portions of the stomach through the esophageal hiatus into the chest cavity.
An axial sliding hernia is among the most common endoscopic findings, noted in up to 25% of upper gastrointestinal examinations (Fig. 3.11). In 80% of cases it is an incidental finding that is classified as a normal variant. The significance of a sliding hernia in the pathogenesis of reflux disease is uncertain. While more than 80% of cases are asymptomatic and endoscopy shows no signs of reflux esophagitis, a sliding hernia is commonly found in cases where esophagitis is already present.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Forward view (Fig. 3.11 a, c)
Forward view (Fig. 3.11 a, c)
- – Double-ring configuration with an intervening, bell-shaped dilatation. The proximal ring is formed by the lower esophageal sphincter (LES), the distal ring by the esophageal hiatus.
- – The gastroesophageal boundary (Z-line) is within the dilated segment, several centimeters above the esophageal hiatus.
- – Shortened distance between the Z-line and incisor teeth
- – Radial folds passing into the hiatus in the lower part of the hernia
- – Double-ring configuration with an intervening, bell-shaped dilatation. The proximal ring is formed by the lower esophageal sphincter (LES), the distal ring by the esophageal hiatus.
 Retroflexed view (Fig. 3.11 b, c)
Retroflexed view (Fig. 3.11 b, c)
- – Cardia does not close snugly around the endoscope
- – Bell-shaped dilatation over the cardia
- – Folds radiating into the hernia
- – Ascent of the hernia during inspiration
- – Cardia does not close snugly around the endoscope
 Caution: Do not pull the retroflexed tip into the esophagus. If this occurs, push back and then straighten the endoscope.
Caution: Do not pull the retroflexed tip into the esophagus. If this occurs, push back and then straighten the endoscope.
Differential diagnosis
 The typical appearance is unmistakable.
The typical appearance is unmistakable.
 Small hernias are often classified as a normal variant.
Small hernias are often classified as a normal variant.
Checklist for endoscopic evaluation
 Distance of the Z-line from the incisor teeth in centimeters
Distance of the Z-line from the incisor teeth in centimeters
 If determinable: distance of the LES from the incisor teeth in centimeters
If determinable: distance of the LES from the incisor teeth in centimeters
 Distance of the esophageal hiatus from the incisor teeth
Distance of the esophageal hiatus from the incisor teeth
 Retroflexed view showing lack of cardial closure around the endoscope
Retroflexed view showing lack of cardial closure around the endoscope
 Evidence of reflux disease
Evidence of reflux disease
Additional Study
 Oral contrast examination with a head-down tilt (only half of radiographically detectable sliding hernias are visible endoscopically)
Oral contrast examination with a head-down tilt (only half of radiographically detectable sliding hernias are visible endoscopically)
Comments
Axial sliding hernia is a common finding and is frequently asymptomatic. With symptomatic reflux, initial treatment consists of supportive measures and proton pump inhibitors (PPI). If medical therapy is unsuccessful or if gastric contents are regurgitated, fundoplication should be performed.
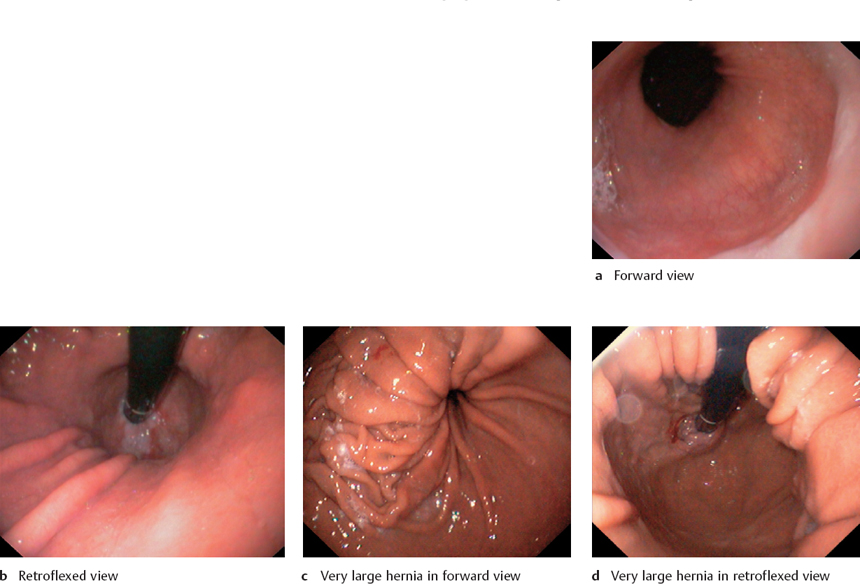
Fig. 3.11 Axial sliding hernia
Hiatal Hernia: Paraesophageal Hernia
 Definition
Definition
Paraesophageal hernia is rare, accounting for less than 5 % of all hernias (Fig. 3.13). In this condition, portions of the gastric fundus are herniated into the mediastinum. This usually occurs on the greater curvature side, owing to the relatively firm attachment of the lesser curvature to the cardia. Because the lower esophageal sphincter and cardia are normally positioned, this type of hernia can be seen only with a retroflexed endoscope.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Visible only in retroflexion (Fig. 3.12)
Visible only in retroflexion (Fig. 3.12)
 Normal configuration of the cardia
Normal configuration of the cardia
 Next to the normal cardia is a second lumen, with mucosal folds radiating into it
Next to the normal cardia is a second lumen, with mucosal folds radiating into it
 Caution: Avoid entering the hernia with the retroflexed scope.
Caution: Avoid entering the hernia with the retroflexed scope.
Differential diagnosis
 The typical appearance is unmistakable.
The typical appearance is unmistakable.
Checklist for endoscopic evaluation
 Inspect the hernia in retroflexion.
Inspect the hernia in retroflexion.
 Check for associated axial sliding hernia (common).
Check for associated axial sliding hernia (common).
 Complications?
Complications?
 Ulceration, necrosis, and incarceration are rarely detectable by endoscopy.
Ulceration, necrosis, and incarceration are rarely detectable by endoscopy.
Additional Study
 Radiographic contrast examination
Radiographic contrast examination
Comments
As there is a potential for incarceration, surgical correction is recommended even for asymptomatic cases (gastropexy, fundoplication for combined hernias).

Fig. 3.12 Paraesophageal hernias
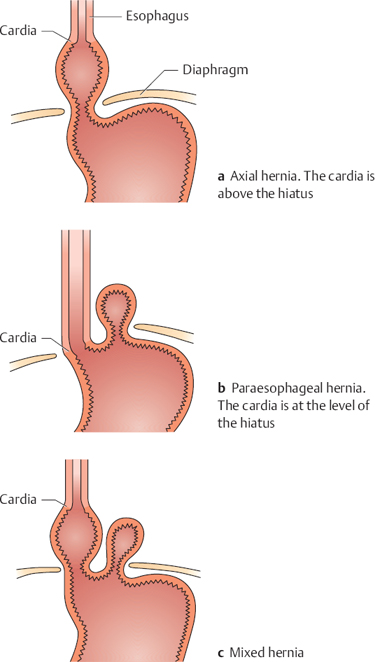
Fig. 3.13 Types of hernia
Hiatal Hernia: Upside-Down Stomach
 Definition
Definition
Upside-down stomach is an extreme form of paraesophageal hernia in which the entire stomach has herniated and rotated upward through the diaphragm into the mediastinum (Fig. 3.14).
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Bizarre presentation (Fig. 3.15)
Bizarre presentation (Fig. 3.15)
 Difficult orientation
Difficult orientation
 It is difficult or impossible to reach the pylorus.
It is difficult or impossible to reach the pylorus.
Differential diagnosis
 None
None
Checklist for endoscopic evaluation
 Inflammatory signs in the esophagus
Inflammatory signs in the esophagus
 Inflammatory signs in the stomach
Inflammatory signs in the stomach
Additional Studies
 Plain chest radiograph (Fig. 3.16)
Plain chest radiograph (Fig. 3.16)
 Radiographic contrast examination
Radiographic contrast examination
Comments
The diagnosis is established by contrast radiographs. Surgical correction is advised for patients who are well enough to tolerate surgery.
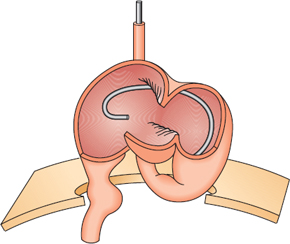
Fig. 3.14 Schematic diagram of upside-down stomach. Complete herniation of the stomach into the chest
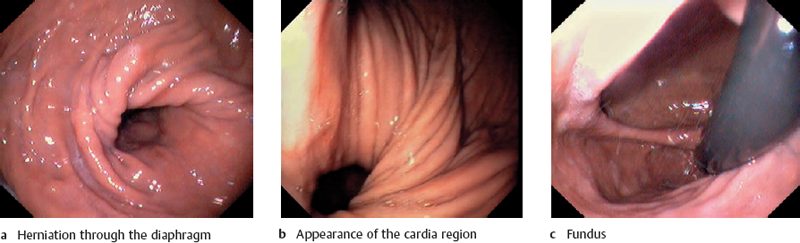
Fig. 3.15 Upside-down stomachs
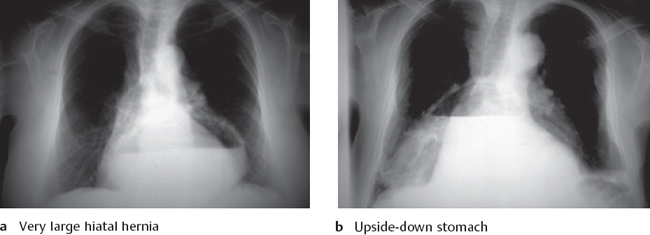
Fig. 3.16 Radiographic findings
Gastroesophageal Prolapse
 Definition and Clinical Aspects
Definition and Clinical Aspects
Gastroesophageal prolapse is defined as the partial intussusception of the anterior stomach wall or greater curvature into the esophagus. Based on published reports, it is discovered in up to 8% of patients who undergo upper GI endoscopy.
Usually there is coexisting cardial incompetence, and an axial sliding hernia is often present (Fig. 3.17). Clinical complaints may include retrosternal pain, usually after a rise in intraabdominal pressure (coughing), as well as bleeding and transient incarceration.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Folds of stomach wall protrude into the distal esophagus during retching, appearing as a fungiform mass (Fig. 3.18)
Folds of stomach wall protrude into the distal esophagus during retching, appearing as a fungiform mass (Fig. 3.18)
 Prolapsed stomach occupies all or part of the esophageal lumen
Prolapsed stomach occupies all or part of the esophageal lumen
 Detectable in the midesophagus and lower esophagus during endoscope insertion
Detectable in the midesophagus and lower esophagus during endoscope insertion
Differential diagnosis
 The typical appearance is unmistakable.
The typical appearance is unmistakable.
Checklist for endoscopic evaluation
 Typical appearance of the prolapse
Typical appearance of the prolapse
 Signs of reflux disease
Signs of reflux disease
 Cardial incompetence
Cardial incompetence
 Hernia
Hernia
 Bleeding at the gastroesophageal junction
Bleeding at the gastroesophageal junction
 Retroflexed view: bleeding in the cardial region
Retroflexed view: bleeding in the cardial region
Additional Studies
 None
None
Comments
The clinical significance of gastroesophageal prolapse is uncertain. Complaints may occur during coughing and other acts that raise the intraabdominal pressure.
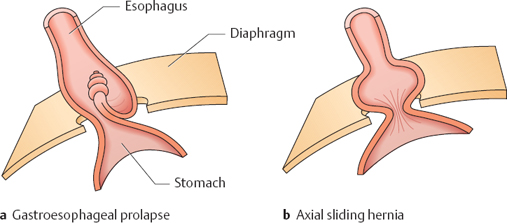
Fig. 3.17 Difference between gastroesophageal prolapse and sliding hernia
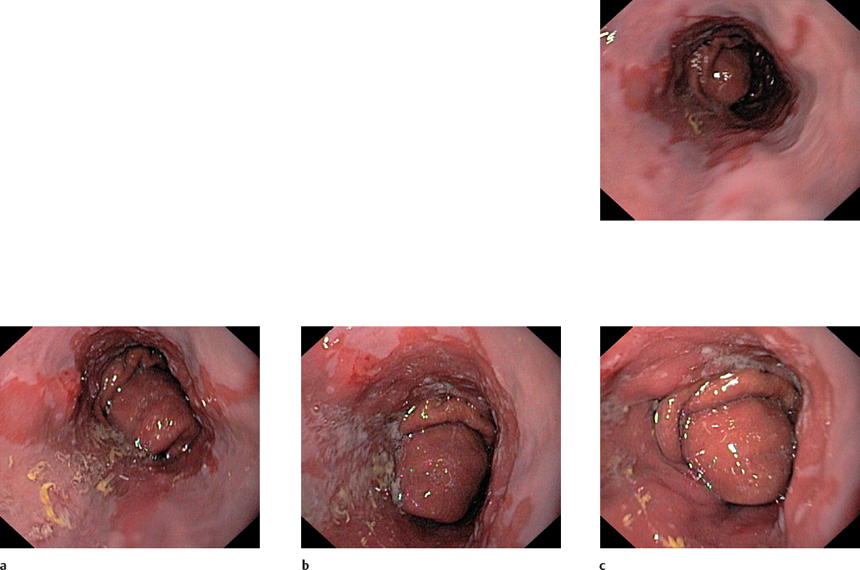
Fig. 3.18 a–d Gastroesophageal prolapse
Mallory-Weiss Lesion and Boerhaave Syndrome
 Definitions and Clinical Aspects
Definitions and Clinical Aspects
The Mallory-Weiss syndrome is characterized by bleeding from a mucosal laceration in the distal esophagus. The cause is a sudden rise in intraabdominal pressure, which may occur with forceful vomiting (especially in alcoholics), vigorous coughing, asthma attacks, or during pregnancy.
A complete rupture of the esophagus is known as Boerhaave syndrome. This complication leads to mediastinitis and has a high mortality rate. Mallory-Weiss lesions reportedly account for 10 % of all cases of upper gastrointestinal bleeding.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Longitudinal blood-stained or bleeding tears (Figs. 3.19, 3.20)
Longitudinal blood-stained or bleeding tears (Figs. 3.19, 3.20)
 Located at the gastroesophageal junction
Located at the gastroesophageal junction
 Frequently posterior
Frequently posterior
Differential diagnosis
 Reflux esophagitis
Reflux esophagitis
 Typical history of Mallory-Weiss lesion: retching followed by bloodless vomiting, then vomiting of blood
Typical history of Mallory-Weiss lesion: retching followed by bloodless vomiting, then vomiting of blood
Checklist for endoscopic evaluation
 Identify the bleeding source.
Identify the bleeding source.
 Endoscopic hemostasis (see p. 155)
Endoscopic hemostasis (see p. 155)
 Evaluate response.
Evaluate response.
 Complete esophagogastroduodenoscopy (EGD) to detect or exclude a concomitant bleeding source.
Complete esophagogastroduodenoscopy (EGD) to detect or exclude a concomitant bleeding source.
Additional Studies
 Oral contrast examination with a water-soluble medium (endoscopy is contraindicated in patients with a suspected perforation or if contrast extravasation occurs)
Oral contrast examination with a water-soluble medium (endoscopy is contraindicated in patients with a suspected perforation or if contrast extravasation occurs)
 Chest radiograph (pneumomediastinum is common in Boerhaave syndrome) (Fig. 3.21)
Chest radiograph (pneumomediastinum is common in Boerhaave syndrome) (Fig. 3.21)
Comments
Treatment for a Mallory-Weiss lesion is described on page 155. Gastroscopy should be repeated after 24 hours. Boerhaave syndrome warrants early, aggressive surgical treatment.
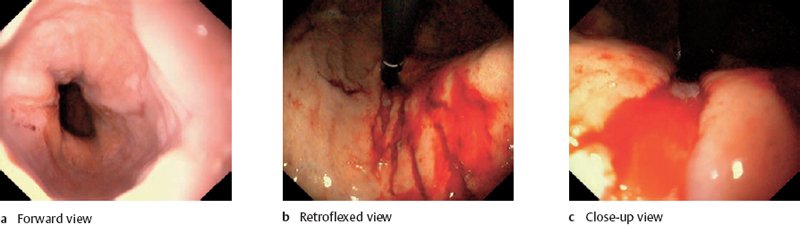
Fig. 3.19 Mallory–Weiss lesion
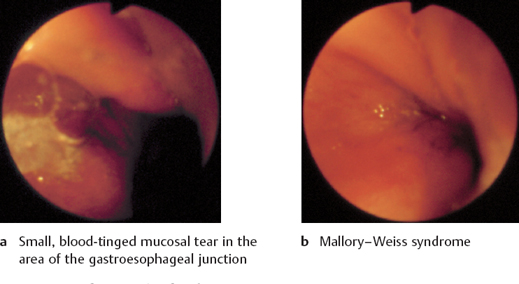
Fig. 3.20 Mallory–Weiss lesions

Fig. 3.21 Pneumomediastinum. Chest radiograph shows definite separation of the mediastinal pleura from the left cardiac border (from: Lange S, Radiologische Diagnostik der Thoraxerkrankung. Stuttgart: Thieme 1996).
Gastroesophageal Reflux and Reflux Esophagitis: Clinical Aspects
 Gastroesophageal Reflux
Gastroesophageal Reflux
Gastroesophageal reflux is a common endoscopic finding (Fig. 3.22). It is seen even in healthy individuals and usually causes no complaints. As a result, endoscopic detection does not necessarily indicate a pathological condition.
Pathophysiology. Because gastric juice contains substances that are corrosive to the esophageal mucosa, there are physiological mechanisms designed to protect the esophagus. Gastroesophageal reflux causes clinical complaints when these antireflux mechanisms fail. They include the sphincter mechanisms, the regenerative capacity of the esophageal epithelium, and the clearance function of esophageal motility, which curtails exposure to the corrosive gastric juice. Factors that predispose to gastroesophageal reflux are listed in Table 3.2.
Complaints. A wide variety of complaints is possible, ranging from mild postprandial discomfort, which the patient may not even consider abnormal, to severe complaints like those seen in reflux esophagitis (Table 3.3).
| Incompetent antireflux mechanisms |
|
| Impaired esophageal clearance |
|
| Impaired gastric emptying |
| Volume and corrosiveness of the refluxate |
 Persistent increased transient relaxation of the LES
Persistent increased transient relaxation of the LES Hypotensive LES
Hypotensive LES Shortened LES
Shortened LES Hiatal hernia
Hiatal hernia Motility disorders (scleroderma)
Motility disorders (scleroderma) | Typical | Atypical |
|---|---|
|
|
 Epigastric pain
Epigastric pain Heartburn
Heartburn Regurgitation
Regurgitation Odynophagia
Odynophagia Dysphagia
Dysphagia Vomiting
Vomiting Chest pain
Chest pain Cough, “chronic bronchitis”
Cough, “chronic bronchitis” Hoarseness
Hoarseness
 Reflux Esophagitis
Reflux Esophagitis
Reflux esophagitis refers to the gross or histological inflammatory changes that occur in the esophageal mucosa in response to reflux. The clinical picture is characterized by retrosternal or epigastric pain, heartburn, and dysphagia that periodically recur. Periods of remission with very mild clinical symptoms are followed by acute exacerbations. In many cases the complaints progress over time, eventually leading to complications such as chronic ulcers, scarring, strictures, columnar metaplasia, and adenocarcinoma.
3.22 Gastroesophageal reflux
Reflux Esophagitis: Diagnosis and Treatment
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria
Endoscopic diagnostic criteria
 Involves the region from the distal esophagus to the Zline
Involves the region from the distal esophagus to the Zline
 Streaky pattern of spread, typically affecting the crests of mucosal folds
Streaky pattern of spread, typically affecting the crests of mucosal folds
 Erythema, erosions, fibrin deposits (Fig. 3.23 a-c)
Erythema, erosions, fibrin deposits (Fig. 3.23 a-c)
 Ulcerations (Fig. 3.23 d)
Ulcerations (Fig. 3.23 d)
 Polypoid mucosal lesions (Fig. 3.24)
Polypoid mucosal lesions (Fig. 3.24)
Differential diagnosis
 Carcinoma, especially in cases with marked inflammatory changes
Carcinoma, especially in cases with marked inflammatory changes
 Mallory-Weiss lesion
Mallory-Weiss lesion
Checklist for endoscopic evaluation
 Define and identify the lesion (erythema, erosion, ulcer).
Define and identify the lesion (erythema, erosion, ulcer).
 Location and extent
Location and extent
 Relation to incisor teeth and to gastroesophageal junction
Relation to incisor teeth and to gastroesophageal junction
 Pattern of spread of erosive changes (see Grading)
Pattern of spread of erosive changes (see Grading)
 Cardial incompetence or hernia?
Cardial incompetence or hernia?
 Signs of chronic changes such as scarring, ulceration, narrowing, ring formation (see Barrett Esophagus p. 70, Peptic Stricture p. 72)
Signs of chronic changes such as scarring, ulceration, narrowing, ring formation (see Barrett Esophagus p. 70, Peptic Stricture p. 72)
Additional Studies
 24-hour pH monitoring
24-hour pH monitoring
 Esophageal manometry
Esophageal manometry
 Radiographic contrast examination to detect or exclude a possible hernia not detectable by endoscopy
Radiographic contrast examination to detect or exclude a possible hernia not detectable by endoscopy
Comments
The diagnosis of reflux disease is based on the clinical presentation, endoscopic findings, histological examination, and 24-hour pH monitoring. It should be emphasized that the correlation between clinical complaints and endoscopic findings is poor. Also, there is not always a close correlation between endoscopy and histology, especially in forms with an essentially normal-appearing mucosa.
 Treatment
Treatment
 PPI therapy
PPI therapy
 If unsuccessful: fundoplication
If unsuccessful: fundoplication
 Treatment of complications (see p. 157, 172)
Treatment of complications (see p. 157, 172)
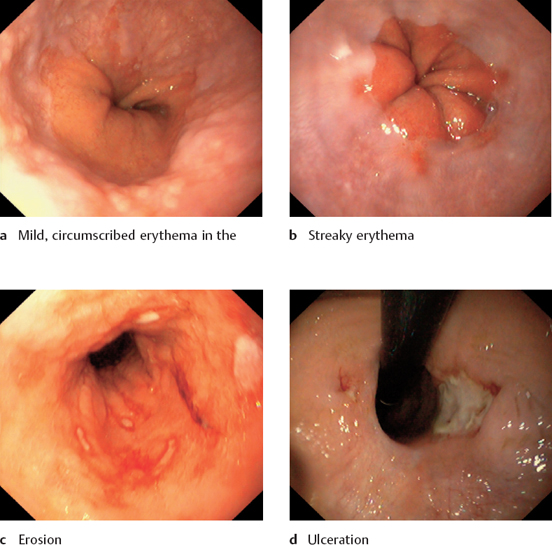
Fig. 3.23 Types of lesion that can occur in reflux esophagitis

Fig. 3.24 Polyps in reflux esophagitis
Reflux Esophagitis: Grading
 Grade I-IV Reflux Esophagitis
Grade I-IV Reflux Esophagitis
The inflammatory lesions of reflux esophagitis are currently graded according to the Savary-Miller classification, which is summarized in Table 3.4.
Grades I-III. Grades I-III (Fig. 3.25) reflect a more or less pronounced acute attack. These grades may be complicated by superficial bleeding, but some cases initially resolve without sequelae.
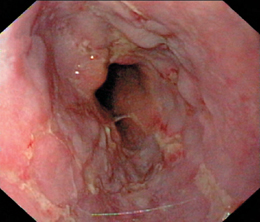
Grade IV. Grade IV (Fig. 3.26) represents the chronic, complicated stage of reflux esophagitis, which is subject to its own dynamic. The most serious complications are obstructive strictures and adenocarcinoma secondary to columnar metaplasia of the esophageal epithelium.
| Grade | Endoscopic findings |
|---|---|
| I | One or more nonconfluent, longitudinal mucosal lesions with erythema and exudate |
| II | Confluent erosive and exudative lesions not covering the entire circumference of the esophagus |
| III | Erosive and exudative lesions covering the entire circumference of the esophagus |
| IV | Chronic mucosal lesions such as ulcer, stricture, and Barrett esophagus |
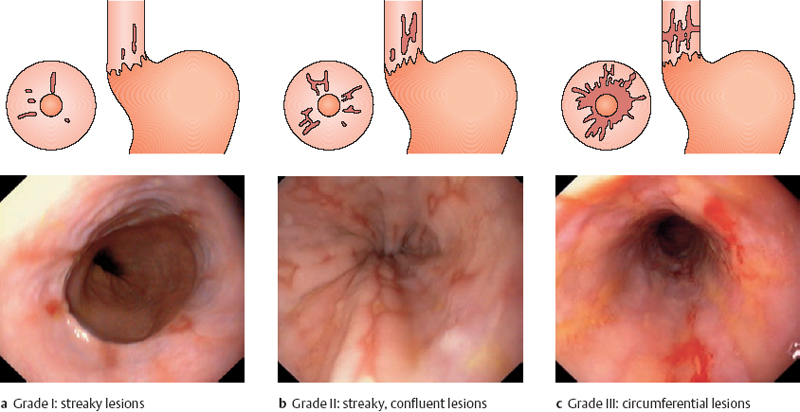
Fig. 3.25 Grading of reflux esophagitis

Fig. 3.26 Grade IV reflux esophagitis
Complications of Reflux Esophagitis: Barrett Esophagus
 Definition and Clinical Aspects
Definition and Clinical Aspects
In simple terms, Barrett esophagus is present when the squamocolumnar junction has migrated proximally into the esophagus by at least 3 cm (Fig. 3.27). This migration occurs when esophageal squamous epithelium that has been damaged by chronic reflux is replaced by metaplastic columnar epithelium.
This condition is found in up to 10% of patients with reflux esophagitis.The importance of the finding—and thus the necessity of identifying it, confirming it by biopsy, and monitoring its progression—lies in the approximately 10% risk of adenocarcinoma formation in the columnar-lined esophagus.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria (Fig. 3.28)
Endoscopic diagnostic criteria (Fig. 3.28)
 Reddened columnar epithelium lining the full circumference of the esophagus
Reddened columnar epithelium lining the full circumference of the esophagus
 Squamocolumnar junction located at least 3 cm above the esophageal hiatus
Squamocolumnar junction located at least 3 cm above the esophageal hiatus
 Frequent tonguelike extensions, occasional islands of epithelium
Frequent tonguelike extensions, occasional islands of epithelium
 “Short Barrett“ = epithelial boundary shifted 2 cm proximally
“Short Barrett“ = epithelial boundary shifted 2 cm proximally
Differential diagnosis
 Barrett carcinoma
Barrett carcinoma
Checklist for endoscopic evaluation
 Distance of the squamocolumnar junction from the incisors
Distance of the squamocolumnar junction from the incisors
 Location of the esophageal hiatus
Location of the esophageal hiatus
 Epithelial islands in the proximal esophagus?
Epithelial islands in the proximal esophagus?
 Hernia?
Hernia?
 Incompetent cardia?
Incompetent cardia?
 Fresh inflammatory changes?
Fresh inflammatory changes?
 Ulcer?
Ulcer?
 Stricture?
Stricture?
 Neoplasia?
Neoplasia?
Additional Studies
 See Management
See Management
Comment
Barrett epithelium is frequently missed at endoscopy. Adenocarcinoma, which develops in up to 10% of patients with Barrett esophagus, is also frequently missed on gross inspection. Dysplasia can be diagnosed only by histological examination.

Fig. 3.28 Barrett epithelium
Complications of Reflux Esophagitis: Management of Barrett Esophagus
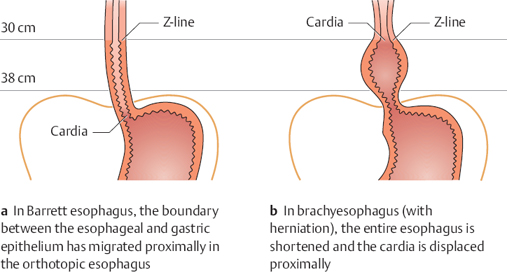
Fig. 3.27 Barrett esophagus and brachyesophagus
 Diagnosis
Diagnosis
 Gross endoscopic criteria
Gross endoscopic criteria
 See page 70
See page 70
 Caution: Barrett epithelium is often missed, as is adenocarcinoma, and it is very common to miss dysplasia at endoscopy.
Caution: Barrett epithelium is often missed, as is adenocarcinoma, and it is very common to miss dysplasia at endoscopy.
Specimen collection
 Circumferential at various levels (every 2 cm)
Circumferential at various levels (every 2 cm) Methylene blue staining (see
Methylene blue staining (see  Brush cytology
Brush cytologyExtended Testing
 Endosonography
Endosonography
 Treatment and Follow-Up
Treatment and Follow-Up
 Barrett epithelium without dysplasia:
Barrett epithelium without dysplasia:
– Yearly endoscopic follow-up with specimen collection
 Barrett epithelium with low-grade dysplasia:
Barrett epithelium with low-grade dysplasia:
– 18-month follow-up
 Barrett epithelium with high-grade dysplasia:
Barrett epithelium with high-grade dysplasia:
– Histological surveillance, then esophageal resection
 Alternatives:
Alternatives:
– Endoscopic treatment: thermal, photodynamic, mechanical
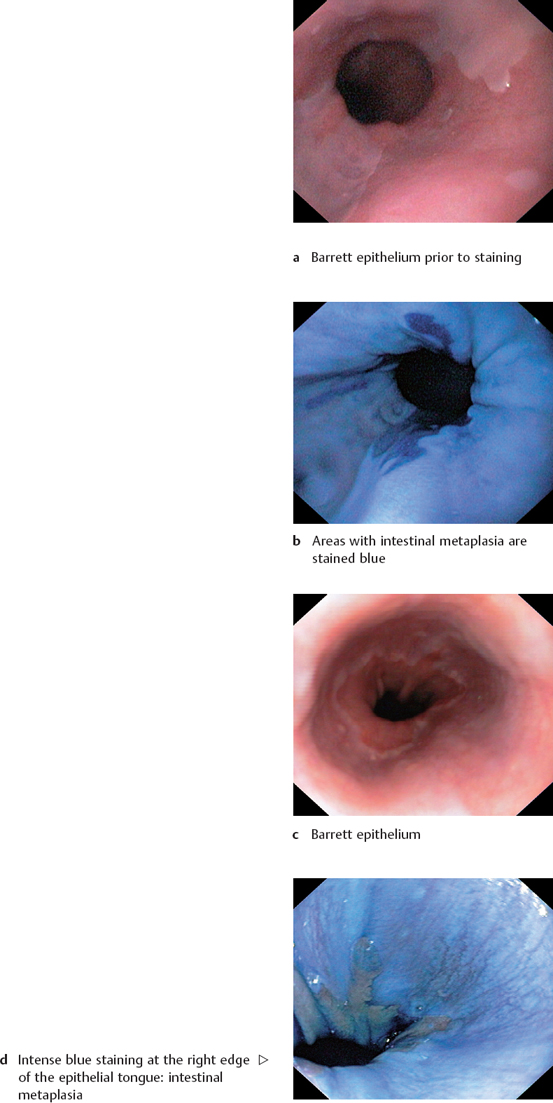
Fig. 3.29 Methylene blue staining
Complications of Reflux Esophagitis: Peptic Stricture
 Pathophysiology
Pathophysiology
Peptic strictures have a reported incidence of up to 15 % in patients with reflux disease. Strictures develop as a result of longstanding gastroesophageal reflux and chronic, deep inflammation (extending into the submucosa) with fibrosis and scarring. They are found in the region of the gastroesophageal junction. Most strictures are short, but some may extend for several centimeters in the distal esophagus. The earliest change is usually a thickening of the Z-line, followed by concentric luminal narrowing that may later become eccentric and may be associated with a diverticulum-like outpouching of the esophagus proximal to the stricture.
 Diagnosis
Diagnosis
 Endoscopic diagnostic criteria (Figs. 3.30–3.35)
Endoscopic diagnostic criteria (Figs. 3.30–3.35)
 Concentric or eccentric narrowing (Figs. 3.30, 3.35)
Concentric or eccentric narrowing (Figs. 3.30, 3.35)
 Surface alterations
Surface alterations
 Firm to the touch
Firm to the touch
 Pseudodiverticulum proximal to the stricture (Fig. 3.32)
Pseudodiverticulum proximal to the stricture (Fig. 3.32)
Differential diagnosis
 Malignant stricture
Malignant stricture
Checklist for endoscopic evaluation
 Distance of the stricture from the incisors
Distance of the stricture from the incisors
 Extent
Extent
 Diameter (using biopsy forceps as a measure)
Diameter (using biopsy forceps as a measure)
 Resistance to instrument passage
Resistance to instrument passage
 Retroflexed view (Fig. 3.33)
Retroflexed view (Fig. 3.33)
 Gross evidence of malignant change?
Gross evidence of malignant change?
Additional Studies
 Biopsy
Biopsy
 Cytology
Cytology
Comments
A peptic stricture often requires endoscope treatment (see Dilation, p. 172).

Fig. 3.30 Peptic stricture of the esophagus
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


