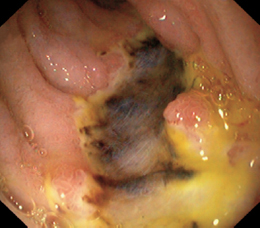
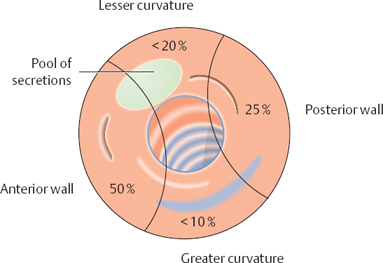
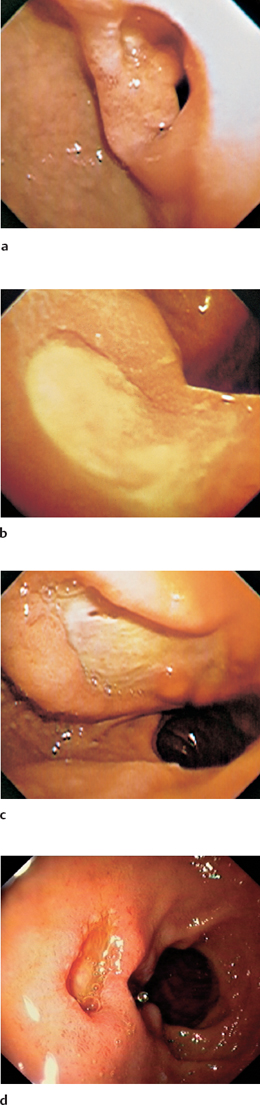
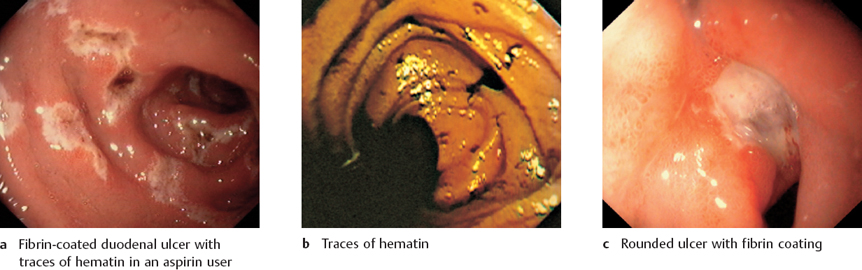
3.3 Pathological Findings: Esophagus Overview of Pathological Findings in the Duodenum Duodenal Ulcer: Clinical Features Duodenum Ulcer: Diagnosis and Treatment Polypoid Lesions in the Duodenum Polypoid Lesions in the Duodenum: Diagnosis Sprue, Crohn Disease, and Whipple Disease Duodenal Changes Associated with Diseases in Adjacent Organs Fig. 3.134 Duodenal ulcer Fig. 3.135 Bulbitis Fig. 3.136 Polypoid lesions in the duodenal bulb Fig. 3.137 Sprue Fig. 3.138 Bulbar diverticulum Fig. 3.139 Inflammation and necrosis in the duodenum of a patient with pancreatitis Duodenal ulcer is an epithelial defect in the bulbar or descending duodenum that penetrates the muscularis mucosae and extends into the submucosa (Fig. 3.141). The precipitating causes include Helicobacter pylori infection (detectable in more than 90% of cases) and the ingestion of nonsteroidal anti-inflammatory drugs (NSAIDs). Additional risk factors include nicotine abuse, alcohol abuse, and stress. A duodenal ulcer cannot be diagnosed from the clinical presentation alone. The symptoms range from typical nocturnal pain and vague or crampy abdominal discomfort to an almost complete absence of complaints, particularly with NSAID-induced ulcers. Ninety percent of duodenal ulcers occur in the duodenal bulb. Ulcers are usually located on the anterior wall of the bulb, less commonly on the posterior wall and lesser curvature. Ulcers on the greater curvature are rare (Fig. 3.140). Multiple “kissing” ulcers are found on the anterior and posterior walls in 10-20% of cases. Ulcers located distal to the bulb should raise suspicion of Zollinger-Ellison syndrome. Fig. 3.140 Frequency distribution of duodenal ulcers Fig. 3.141a–d Duodenal ulcer The patient is treated with proton pump inhibitors (PPI). If H. pylori is detected, eradication therapy is indicated (see p. 103). An uncomplicated duodenal ulcer that shows good clinical response does not require endoscopic follow-up. If complaints persist, the patient should undergo repeat endoscopy with biopsy (Crohn disease?), and further tests should be performed to exclude Zollinger-Ellison syndrome. Fig. 3.142 Duodenal ulcer
Overview of Pathological Findings in the Duodenum
 Duodenal ulcer
Duodenal ulcer
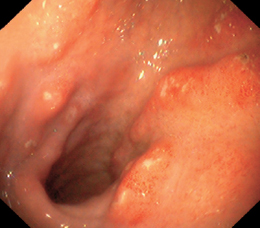
 Bulbitis
Bulbitis
 Polypoid lesions
Polypoid lesions
 Sprue
Sprue
 Crohn disease
Crohn disease
 Whipple disease
Whipple disease
 Diverticula
Diverticula
 Changes associated with diseases in adjacent organs
Changes associated with diseases in adjacent organs

Duodenal Ulcer: Clinical Features
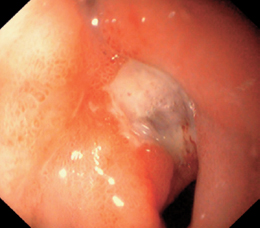
 Definition and Causes
Definition and Causes
 Clinical Aspects
Clinical Aspects
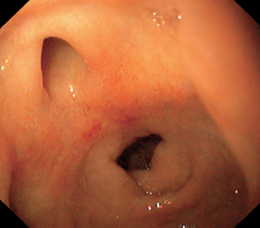
 Location
Location
Duodenal Ulcer: Diagnosis and Treatment
 Diagnosis
Diagnosis
![]() Endoscopic diagnostic criteria (Figs. 3.141, 3.142)
Endoscopic diagnostic criteria (Figs. 3.141, 3.142)
 The endoscopic appearance depends on the ulcer stage. Three stages are distinguished: the active stage, healing stage, and scar stage.
The endoscopic appearance depends on the ulcer stage. Three stages are distinguished: the active stage, healing stage, and scar stage.
 Active stage
Active stage
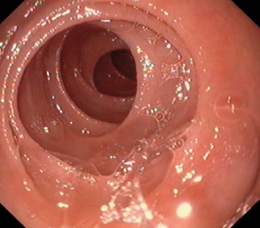
 Healing stage
Healing stage
 Scar stage
Scar stage
Differential diagnosis
 typical appearance
typical appearance
 Very rare: penetrating pancreatic carcinoma
Very rare: penetrating pancreatic carcinoma
 Carcinoid
Carcinoid
 Crohn disease
Crohn disease
 Malignant lymphoma
Malignant lymphoma
 Duodenal carcinoma
Duodenal carcinoma
Checklist for endoscopic evaluation
 Location
Location
 Size
Size
 Number
Number
 Shape: round, oval, oblong, linear, bizarre
Shape: round, oval, oblong, linear, bizarre
 Ulcer margin
Ulcer margin
 Ulcer base: fresh blood, hematin, fibrin, visible vessel
Ulcer base: fresh blood, hematin, fibrin, visible vessel
 Assess need for endoscopic treatment.
Assess need for endoscopic treatment.
Additional Studies
 Always biopsy the gastric antrum and body (H. pylori?) for histology, rapid urease testing, or both.
Always biopsy the gastric antrum and body (H. pylori?) for histology, rapid urease testing, or both.
 Biopsy the ulcer only if it does not heal or in order to exclude a particular diagnosis (Crohn disease).
Biopsy the ulcer only if it does not heal or in order to exclude a particular diagnosis (Crohn disease).
 Treatment and Follow-Up
Treatment and Follow-Up
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


