Purpose
To report the efficacy and safety of outpatient fluid-gas exchange for open macular hole after primary vitrectomy.
Design
Retrospective interventional case series.
Methods
setting : Institutional. patients : Thirty-six patients with primary failed closure or reopened holes after primary vitrectomy. intervention : Fluid-gas excahnge with 15% perfluoropropane (C 3 F 8 ) or 20% sulfur hexafluoride (SF 6 ) was performed to reclose the hole under topical anesthesia. main outcome measures : The hole closure rate and type, pre- and postexchange best-corrected visual acuity (BCVA), and complication rates were assessed.
Results
Thirty-two eyes (89%) achieved anatomic success from 1-3 weeks after the fluid-gas exchange. Twenty-two eyes (61%) achieved type 1 closure, 10 eyes (28%) achieved type 2 closure, and 4 eyes (11%) did not achieve closure. The BCVA for type 1 closure improved significantly from logarithm of the minimal angle of resolution (logMAR) 1.66 ± 0.41 to 0.84 ± 0.41, with a P value <.001. The BCVA for type 2 closure improved from logMAR 1.77 ± 0.41 to 1.52 ± 0.41, with a P value of .05. All patients with an unclosed hole after fluid-gas exchange had a stage IV macular hole before the primary vitrectomy and a hole size larger than 1000 μm. The complication related to fluid-gas exchange procedure was transient high intraocular pressure, which responded well to topical antiglaucoma medications. There were 2 retinal detachment cases following the exchange; surgery to reattach the retina was performed, with visual acuity recovery.
Conclusion
Outpatient fluid-gas exchange is an effective treatment option for eyes with open holes following vitrectomy.
A macular hole can distort vision, and pars plana vitrectomy (PPV) is a widely accepted surgery for repairing the hole. The use of gas tamponade, face-down posturing, and internal limiting membrane (ILM) peeling have been reported to increase anatomic closure and improve visual function recovery. The closure rate after PPV and ILM peeling ranges from 78%-95%. Unfortunately, some holes fail to close after PPV, and others may reopen after the primary vitrectomy. Without successful anatomic results, visual acuity remains poor.
One of the reasons for the unsuccessful closure of the macular hole could be the residual traction above the macular area. The residual epiretinal membrane or ILM could exert tangential traction, leading to a nonclosure or reopening. Reoperation to enlarge the ILM peeling area has been reported to reclose macular holes and lead to visual improvement. However, a second invasive intervention can be significantly stressful for the patient and the surgeon. Fluid-gas exchange is a simple and cost-effective method to reclose holes. Previous reports have provided us with insights into the effectiveness of this treatment. In our study, we performed fluid-gas exchange for an open hole after PPV with ILM peeling; we present a detailed correlation between the type of anatomic closure and its functional impact.
Methods
Type of Study
This is a single-center interventional case series that was conducted in the VitreoRetina Service, Department of Ophthalmology of Chang-Gung Memorial Hospital. The surgeries were performed by retina specialists between 2000 and 2010. This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Taiwan (99-1036B, Title: Long-term surgical outcomes of macular hole repair) in 2010. Informed consent was obtained for all subjects.
Patient Data Collection
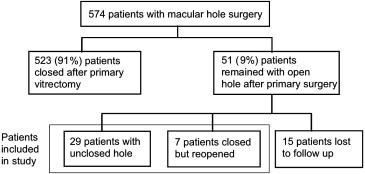
Thirty-six patients who required additional fluid-gas exchange for unclosed or reopened holes after primary surgery were reviewed ( Figure 1 ). The data obtained included the following: age, sex, affected eye, refraction, axial length, intraocular pressure (IOP) before and after exchange, systemic disease, primary vitrectomy details, macular hole initial stage, hole status after exchange, best-corrected visual acuity (BCVA) before and after the primary vitrectomy, BCVA before and after fluid-gas exchange, and lens status before and after the primary vitrectomy.
Primary Surgical Technique
The primary surgery included 20G or 23G PPV with ILM peeling under retrobulbar anesthesia. The ILM was peeled to at least 2 disc areas from the edges of the hole. At the end of the vitrectomy, a gas flush was performed with 20% sulfur hexafluoride (SF 6 ) or 15% perfluoropropane (C 3 F 8 ), according to each surgeon’s preference. After surgery, the patients were instructed to immediately assume a strictly prone position for at least 5 days.
The patients were examined 1 day after the surgery; at week 1, week 2, month 1, month 3, and month 6; and then every 6 months. Additional visits were added, depending on the patient’s condition. The BCVA of the last follow-up was transformed to logarithm of the minimal angle of resolution (logMAR) for statistical analysis. Given that no consensus exists with respect to low vision states, the transforming scale was performed according to Schulze-Bonsel and associates. Optical coherence tomography (OCT; Carl Zeiss Ophthalmic System, Dublin, California, USA) was performed to determine the closure status of the hole. If the hole remained open, a fluid-gas exchange was performed. After the procedure, the hole closure status was reassessed.
Fluid-Gas Exchange Technique
To minimize the risk of endophthalmitis, we prepared the patients with an aseptic technique, instilled povidone solution 5% on the conjunctival sac, and waited for 1 minute before performing the fluid-gas exchange under topical anesthesia. Either 20% SF 6 or 15% C 3 F 8 was prepared in a 10-mL syringe. Immediately before the procedure, the injection sites were soaked with an anesthetic solution of proparacaine hydrochloride ophthalmic solution (USP 0.5%; Alcon Laboratories, Ft. Worth, Texas, USA) using a cotton swab for 20 seconds. Using a 27-gauge needle connected to the syringe, the gas was injected into the vitreous cavity through the inferior pars plana at 3.5-4 mm, depending on the phakic status of the patient. Simultaneously, another 25-gauge needle was inserted at another site in the inferior pars plana to drain the fluid. A total of 4-8 mL of gas was injected to fill the cavity. When the gas bubble was drained out from the fluid drainage syringe, the cavity was filled. After the procedure, a topical antibiotic was prescribed for 5 days, and the patient was instructed to assume a strictly prone position for at least 7 days. Again, patients were examined with ophthalmoscopy until the gas had been absorbed, and OCT was performed afterwards. If the hole closed without any neurosensory defects, it was classified as a type 1 closure. If the hole’s edges were flattened, and the hole size reduced, while some neurosensory defect persisted, it was classified as a type 2 closure. Lastly, the hole was classified as nonclosed when the opening persisted with elevated edges and when the hole size either did not change or became even larger than the preoperative hole.
Statistical Analysis
Statistical analysis was performed with GraphPad Prism software (version 5; GraphPad Software Inc., La Jolla, CA) Interval-ratio variable covariates were assessed using a paired t test of 2 means. To compare more than 2 means, an ANOVA test was used. Nominal covariates were assessed individually with the χ 2 test. Simple linear regression was used to calculate the time between primary vitrectomy and fluid-gas exchange vs visual acuity improvement as the difference between visual acuity measures before and after fluid-gas exchange and as the perceptual increment of the visual acuity over the pre-exchange measure.
Subgroup analysis of the visual acuity improvement, expressed as logMAR, was segmented, according to the postexchange status of the hole, using an independent-sample 1-tailed t test, and a P value <.05 was considered statistically significant.
Results
Demographic Data
This study included 36 patients, and the average age was 61 years, ranging from 30-78 years. The mean refraction was −2.3 ± 4.3 diopters. The mean axial length was 23.7 ± 1.7 mm. Nineteen patients had systemic diseases, such as diabetes, hypertension, or another cardiovascular disease. Assessment of the preoperative hole stage indicated that 13 patients were stage III and 23 patients were stage IV. Among them, the holes of 29 patients failed to close primarily; in 7 patients, the hole had closed but reopened 2-6 months after the primary vitrectomy. All 36 patients underwent fluid-gas exchange to reclose the hole. SF 6 was used in 8 patients and C 3 F 8 was used in 28 patients. The mean follow-up period was 28.3 ± 36.7 months. During this period, 4 patients in the type 1 closure group required a second exchange to achieve anatomic success. Table 1 summarizes the demographic data, which are subgrouped by final closure type and P value for the comparison among these 3 closure types.
| Total | Type 1 Closure | Type 2 Closure | No Closure | P Value | |
|---|---|---|---|---|---|
| Number of patients (male/female) | 36 (13/23) | 22 (8/14) | 10 (4/6) | 4 (1/3) | NA |
| Eye affected (OD:OS) | 7:29 | 5:17 | 1:09 | 1:03 | NA |
| Age (y), mean ± SD (range) | 61 ± 10 (30-78) | 63 ± 7 (46-78) | 57 ± 14 (30-77) | 58 ± 3 (53-62) | .20 |
| Refraction, mean ± SD | −2.3 ± 4.3 | −2.1 ± 4.6 | −3.2 ± 4.0 | −1.9 ± 0.1 | .86 |
| Axial length (mm), mean ± SD | 23.7 ± 1.7 | 23.9 ± 2.0 | 23.2 ± 0.4 | 23.8 ± 1.1 | .79 |
| Systemic disease, n (%) | 19 (53%) | 13 (59%) | 4 (40%) | 2 (50%) | .60 |
| Hole stage, n (%) | .07 | ||||
| Stage III | 13 (36%) | 11 (50%) | 2 (20%) | 0 (0%) | |
| Stage IV | 23 (64%) | 11 (50%) | 8 (80%) | 4 (100%) | |
| No primary closure, n (%) | 29 (81%) | 18 (82%) | 8 (80%) | 3 (75%) | .95 |
| Closed but reopened, n (%) | 7 (19%) | 4 (18%) | 2 (20%) | 1 (25%) | |
| Gas used, n (%) (SF 6 :C 3 F 8 ) | 8:28 (22%:78%) | 4:18 (18%:82%) | 1:9 (10%:90%) | 3:1 (75%:25%) | .02 a |
| Complication, n (%) | NA | ||||
| High IOP | 3 (8%) | 2 (9%) | 0 (0%) | 1 (25%) | |
| Retinal detachment | 2 (5%) | 0 (0%) | 1 (10%) | 1 (25%) | |
| Time between the primary surgery and FGE (d), mean ± SD | 82.6 ± 125.7 | 83.1 ± 150.3 | 88.1 ± 81.8 | 66.8 ± 31.3 | .96 |
| Follow-up (mo), mean ± SD | 28.3 ± 36.7 | 23.9 ± 32.7 | 39.4 ± 46.2 | 24.3 ± 22.2 | .55 |
Anatomic Outcome
Thirty-two of 36 eyes (89%) achieved hole closure 1-3 weeks after the fluid-gas exchange; of them, 22 eyes had type 1 closure and 10 eyes had type 2 closure. Four eyes failed to achieve closure. A subgroup analysis was performed with the patients separated into the “nonprimary closure” and the “primary closure but with reopening” groups. In the nonprimary closure group, the holes of 90% (26 of 29) of the patients closed, while those of 10% (3 of 29) failed to close. In the reopened group, the holes of 86% (6 of 7) of patients closed, while those of 14% (1 of 7) failed to close. A Pearson χ 2 test showed a P value of .95, which indicated that no correlation exists between the pre-exchange status (the primary unclosed vs reopened hole) and the postexchange result.
There was a trend ( P = .07) between the preoperative hole stage and the final anatomic outcome, although it was not statistically significant. Of all the holes of the stage III patients that closed after the exchange, 85% (11 of 13) were type 1 closures and 15% (2 of 13) were type 2 closures. There were no opened holes after the exchange in stage III, whereas the holes of 83% (19 of 23) of stage IV patients closed, with 48% (11 of 23) achieving type 1 closure and 35% (8 of 23), type 2 closure. The remaining 17% (4 of 23) had a persistently open hole.
There was no association between systemic disease and anatomic outcome ( P = .60). The refraction and axial lengths were comparable between different closure types. Therefore, there is no correlation between these and the anatomic outcomes ( P = .86 for refraction and P = .79 for axial length), most likely because there were few patients with extreme myopia or very increased axial lengths in this study.
Functional Outcome
In 85% (31 of 36) of the patients, vision improved after the fluid-gas exchange. The BCVAs before the primary vitrectomy, before the fluid-gas exchange, and after the exchange are shown in Table 2 , according to the anatomic outcome. Those patients with type 1 closure had significantly improved visual acuity after the exchange ( P < .001 between the measures before and after the exchange), whereas the vision of patients with type 2 closures and nonclosures basically remained the same, with very few improvements ( Figure 2 ).
| Anatomic Outcome | Pre-Primary Surgery | Pre-Fluid-Gas Exchange | Post-Fluid-Gas Exchange | P Value ( t Test) | |
|---|---|---|---|---|---|
| Closure type 1 | Mean ± SD | 1.35 ± 0.42 | 1.66 ± 0.41 | 0.84 ± 0.41 | <.001 a |
| Median | 1.39 | 1.69 | 0.69 | ||
| Maximum | 2 | 2.41 | 1.39 | ||
| Minimum | 0.22 | 1 | 0.09 | ||
| 0.77±0.41(∞) | |||||
| Closure type 2 | Mean ± SD | 1.59 ± 0.55 | 1.77 ± 0.41 | 1.52 ± 0.41 | .05 |
| Median | 1.57 | 1.89 | 1.41 | ||
| Maximum | 2.48 | 2.48 | 2.44 | ||
| Minimum | 0.69 | 1.22 | 0.69 | ||
| 1.53 ± 0.62 b | |||||
| No closure | Mean ± SD | 1.78 ± 0.66 | 1.94 ± 0.07 | 1.73 ± 0.13 | .06 |
| Median | 1.97 | 1.96 | 1.77 | ||
| Maximum | 2.48 | 2 | 1.85 | ||
| Minimum | 0.69 | 1.82 | 1.52 | ||
| 1.73 ± 0.13 b |
b Mean visual acuity and SD of the patients who had cataract surgery, excluding those without it.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


