Purpose
To evaluate the indications, visual outcomes, and complication rate after posterior implantation of an iris-claw aphakic intraocular lens (IOL) in children.
Design
Noncomparative retrospective cohort study.
Methods
setting : Institutional practice. patients/intervention procedures : Seven eyes of 4 children without adequate capsular support had posterior chamber iris-claw aphakic IOL implantation between 2007 and 2012. main outcome measures : Visual acuity, endothelial cell changes, intraoperative and postoperative complications.
Results
The mean age of the 3 boys and 1 girl was 12.0 ± 3.4 (SD) years (range 8-16 years). In all eyes, the mean postoperative best spectacle-corrected visual acuity (0.13 ± 0.17 logMAR) was statistically significantly better at the last follow-up than at 1 day preoperatively (0.60 ± 0.39 logMAR) ( P < .05). The mean follow-up was 31 months (range 10-64 months). The mean endothelial cell density decreased from 3013 ± 155 cells/mm 2 preoperatively to 2831 ± 236 cells/mm 2 at last follow-up, representing a mean endothelial cell loss of 6.4%. No corneal decompensation, iritis, secondary glaucoma, or pupillary block occurred after surgery in any eye. Postoperative complications included transient postoperative hypotony in 1 eye and a traumatic dislocation of a posterior aphakic iris-claw IOL in 1 eye.
Conclusion
The posterior implantation technique of aphakic iris-claw IOL provided good visual outcomes with a favorable complication rate and can be used as a reasonable alternative for a wide range of indications in pediatric eyes without adequate capsular support.
Primary in-the-bag placement of a posterior chamber intraocular lens (PCIOL) is one option to correct aphakia after cataract extraction in children, particularly in those 2 years of age and older. Although spectacles and contact lenses may be regarded as the standard of care in infants and young children, they are not always well tolerated. In these cases, secondary intraocular lens (IOL) implantation can be considered. However, in the absence of adequate capsular support, the surgical correction of aphakia is challenging. Options include iris-fixated or angle-supported anterior chamber (AC)IOL, scleral-fixated PCIOL, iris-fixated PCIOL, or a glued intrascleral-fixated PCIOL.
ACIOLs can be associated with severe complications, such as corneal endothelial cell loss leading to corneal decompensation, iris sphincter erosion, glaucoma, chronic inflammation, and hyphema, and they are infrequently used in children.
However, in scleral- and iris-fixated IOLs suture-related complications have been reported, including infection/endophthalmitis, IOL tilt, macular edema, dislocation of the lens into the vitreous, intraocular hemorrhage, and secondary glaucoma.
Artisan iris-claw lenses were initially developed by Fechner and Worst in 1978 and modified to a convex/concave configuration in 1997. An anterior iris-fixated IOL has become a suitable choice in the absence of capsular support, and several studies report safe implantation of these IOLs in children.
In this study, we report our experience with posterior iris-fixated Artisan iris-claw lenses for the correction of aphakia in children.
Methods
This is a retrospective case series of all consecutive cases of Artisan PCIOL (Verisyse VRS54; Ophthec BV, Groningen, The Netherlands; Advanced Medical Optics, Inc., Santa Ana, California, USA) implantation in children between April 4, 2007 and January 30, 2012 at Charité University Hospital Berlin. This noncomparative retrospective cohort study was approved by the Institutional Review Board of our hospital, namely the ethics committee of the Charité University Hospital Berlin, and adheres to the Declaration of Helsinki and all German federal and state laws.
Informed consent was obtained from all patients’ parents or guardians before surgery. Informed consent for participation of their children in this retrospective cohort study was obtained from all patients’ parents or guardians before last follow-up visit. Preoperative and postoperative evaluations included best spectacle-corrected visual acuity (BCVA), spherical equivalent (SE), Goldmann applanation tonometry, slit-lamp examination, fundus examination, number of antiglaucoma eye drops, central corneal thickness (Orbscan; Bausch & Lomb, Rochester, New York, USA), corneal endothelial cell density (ECD) (Noncon Robo-CA; Konan), and surgical complications. All patients were operated on by 1 of 2 experienced surgeons (E.B., P.R.) using the same surgical protocol in all cases. The IOL power was calculated using the Sanders-Retzlaff-Kraff theoretical formula and an A-constant of 116.9 (manufacturer’s recommendation). The target refraction ranged from slight myopia to +2.00 diopters (D), depending on the child’s age at the time of the surgery. Visual acuity was converted to logMAR values for statistical analysis, which was performed using the Student t test.
Surgical Technique
Under general anesthesia, a 5.5-mm sclerocorneal tunnel incision was made at 12 o’clock and 2 paracenteses were created at the 3-o’clock and 9-o’clock positions. The pupil was not dilated initially. A cohesive ophthalmic viscosurgical device (OVD) was placed in the anterior chamber through the paracentesis. If vitreous was seen in the anterior chamber, anterior vitrectomy was performed. Then, the iris-claw IOL was inserted through the scleral tunnel upside-down in a reversed position into the anterior chamber. The PCIOL was rotated with a hook into a horizontal position from 3 to 9 o’clock and centered over the pupil. After IOL insertion, acetylcholine chloride 1% (Miochol-E, Bausch & Lomb) was injected in the anterior chamber. With the aid of lens fixation forceps, the iris-claw IOL was slipped through the pupil area, maintained horizontally with the forceps, then recentered over the pupil behind the iris plane with the haptics positioned again at 3 and 9 o’clock. The correct orientation of the iris-claw IOL using the Purkinje images was checked before iris entrapment by haptics. IOL-claws were enclavated into the iris with a spatula long enough that both haptics could be reached through 1 paracentesis without hand exchange. The surgeons avoided placing too much pressure on the pupillary margin by not engaging too much tissue in the claw mechanism, and the claw was placed far enough from the iris root to prevent interference with iris movement. Displacement, ovalization, and pupil deformation were prevented by meticulously positioning the iris claw with an adequate amount of iris tissue to guarantee pupil movement. Peripheral slit iridectomy was not performed. All the OVD was removed, and the incision was closed with interrupted 10-0 nylon sutures. Then, the conjunctiva was sutured with interrupted 9-0 polyglactin (Vicryl; Ethicon Inc., Johnson & Johnson Co, Somerville, New Jersey, USA) sutures. Ofloxacin and dexamethasone drops were prescribed after surgery and slowly tapered over 4 weeks.
Results
The study comprised 7 eyes of 4 patients. The mean age of the 3 boys and 1 girl was 12.0 ± 3.4 (SD) years (range 8-16 years). The mean follow-up was 31 ± 21 months (range 10-64 months; median 24 months).
The IOLs were inserted during primary IOL implantation in 2 eyes of 1 patient with idiopathic subluxated crystalline lenses and in 2 eyes of 1 patient with subluxated crystalline lenses attributable to Marfan syndrome. The posterior iris-claw IOL was implanted as a secondary procedure in 2 eyes of 1 patient after bilateral congenital cataract extraction and in 1 eye after cataract extraction attributable to Marinesco-Sjogren syndrome without adequate capsular support.
In all eyes, the mean postoperative BCVA (0.13 ± 0.17 logMAR) was statistically significantly better at the last follow-up than at 1 day preoperatively (0.60 ± 0.39 logMAR) ( P < .05) ( Table ). Five eyes gained more than 2 lines after surgery.
| Patient Number | Age at Surgery (y) | Preoperative BCVA (logMAR) | Postoperative BCVA (1 mo, logMAR) | Postoperative BCVA (Last Visit, logMAR) | Follow-up (mo) |
|---|---|---|---|---|---|
| 1 | 16 | 0.70 | 0.50 | 0.10 | 23 |
| 1 | 16 | 0.60 | 0.80 | 0.00 | 24 |
| 2 | 8 | 1.30 | 0.20 | 0.50 | 64 |
| 2 | 9 | 0.70 | 0.25 | 0.10 | 55 |
| 3 | 9 | 0.60 | 0.40 | 0.00 | 28 |
| 4 | 13 | 0.10 | 0.80 | 0.10 | 10 |
| 4 | 13 | 0.20 | 0.80 | 0.10 | 10 |
The mean postoperative SE at the last follow-up was −0.43 ± 2.47 D (range −4.0 to +4.25 D). At the last follow-up, the postoperative SE was within ±2.00 D of emmetropia in 5 eyes.
The mean corneal ECD decreased from 3013 ± 155 cells/mm 2 preoperatively to 2831 ± 236 cells/mm 2 at last follow-up, representing a mean endothelial cell loss of 6.4%. The mean central corneal thickness was 648 ± 56 μm at last follow-up. In 2 eyes endothelial cell count and central corneal thickness could not be measured because of nystagmus.
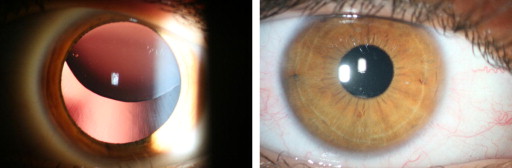
The mean intraocular pressure (IOP) at the last follow-up (16.7 ± 3.3 mm Hg) was lower than at 1 day preoperatively (17.9 ± 4.7 mm Hg) ( P > .05). The IOP data were not corrected for changes in corneal thickness. No secondary glaucoma or pupillary block occurred after surgery in any eye. All eyes achieved the desired anatomic results ( Figure , Right). Complications included transient postoperative hypotony in 1 eye and a traumatic IOL dislocation in 1 eye.
Results
The study comprised 7 eyes of 4 patients. The mean age of the 3 boys and 1 girl was 12.0 ± 3.4 (SD) years (range 8-16 years). The mean follow-up was 31 ± 21 months (range 10-64 months; median 24 months).
The IOLs were inserted during primary IOL implantation in 2 eyes of 1 patient with idiopathic subluxated crystalline lenses and in 2 eyes of 1 patient with subluxated crystalline lenses attributable to Marfan syndrome. The posterior iris-claw IOL was implanted as a secondary procedure in 2 eyes of 1 patient after bilateral congenital cataract extraction and in 1 eye after cataract extraction attributable to Marinesco-Sjogren syndrome without adequate capsular support.
In all eyes, the mean postoperative BCVA (0.13 ± 0.17 logMAR) was statistically significantly better at the last follow-up than at 1 day preoperatively (0.60 ± 0.39 logMAR) ( P < .05) ( Table ). Five eyes gained more than 2 lines after surgery.



