6 Otosclerosis • An autosomal dominant disease of incomplete penetrance affecting bone derived from the otic capsule in which mature lamellar bone is replaced by woven bone of greater cellularity and vascularity • Aetiology • Confined to human temporal bone derived from otic capsule; the new woven bone has increased cellularity and vascularity alongside fibrous replacement and sclerosis; alternating phases of bone resorption and formation • During embryonic ossification of cochlea the area anterior to oval window remains cartilaginous before degenerating to simple fibrous tissue and forming fissula ante fenestram, which becomes the most common site for otosclerotic focus • Vascular connective tissue replaced by neo-osteogenesis • M:F 1:2, middle-aged; positive family history in 50%; effect • Gradual onset of conductive hearing loss (CHL); in time ~10% develop sensorineural hearing loss (SNHL) • Active progression during pregnancy • Paracusis of Willis—speech perceived better in a noisy background because better discrimination when stimulus is raised above normal conversational level • Bilateral in ~80% • Tinnitus common • Vertigo can occur with an otosclerotic focus in labyrinth • May coexist with Ménière disease (relative contraindication to stapedectomy) • tympanic membrane (TM) usually unremarkable • Schwartze sign—vascular or “flamingo” flush over the promontory • CHL ± SNHL • Tuning forks: usually Rinne–ve (256 Hz flips at ~15–20 dB air–bone gap (ABG), 512 Hz at ~25 dB, 1024 Hz at ~30–35 dB) • pure tone audiogram: • Speech audiometry: • Tympanometry—usually normal (reduced mobility unreliably shown) • Stapedial reflex (as measured by changes in compliance): • Vestibulometry
6.1 Definition
6.2 Pathology
 Genetics: autosomal dominant with incomplete penetrance
Genetics: autosomal dominant with incomplete penetrance
 Autoimmune: there may be an autoimmune component to the aetiology (autoimmunity to type II collagen)
Autoimmune: there may be an autoimmune component to the aetiology (autoimmunity to type II collagen)
 Hormonal: oestrogens stimulate osteoclastic activity; disease noted to progress with pregnancy/menopause
Hormonal: oestrogens stimulate osteoclastic activity; disease noted to progress with pregnancy/menopause
 Viral: measles infection in particular may have a secondary role in those with a genetic predisposition
Viral: measles infection in particular may have a secondary role in those with a genetic predisposition
6.3 Clinical Presentation
6.3.1 History
6.3.2 Examination
6.3.3 Audiometry
 Progressive conductive hearing loss (HL)
Progressive conductive hearing loss (HL)
 When cochlea involved, SNHL added component
When cochlea involved, SNHL added component
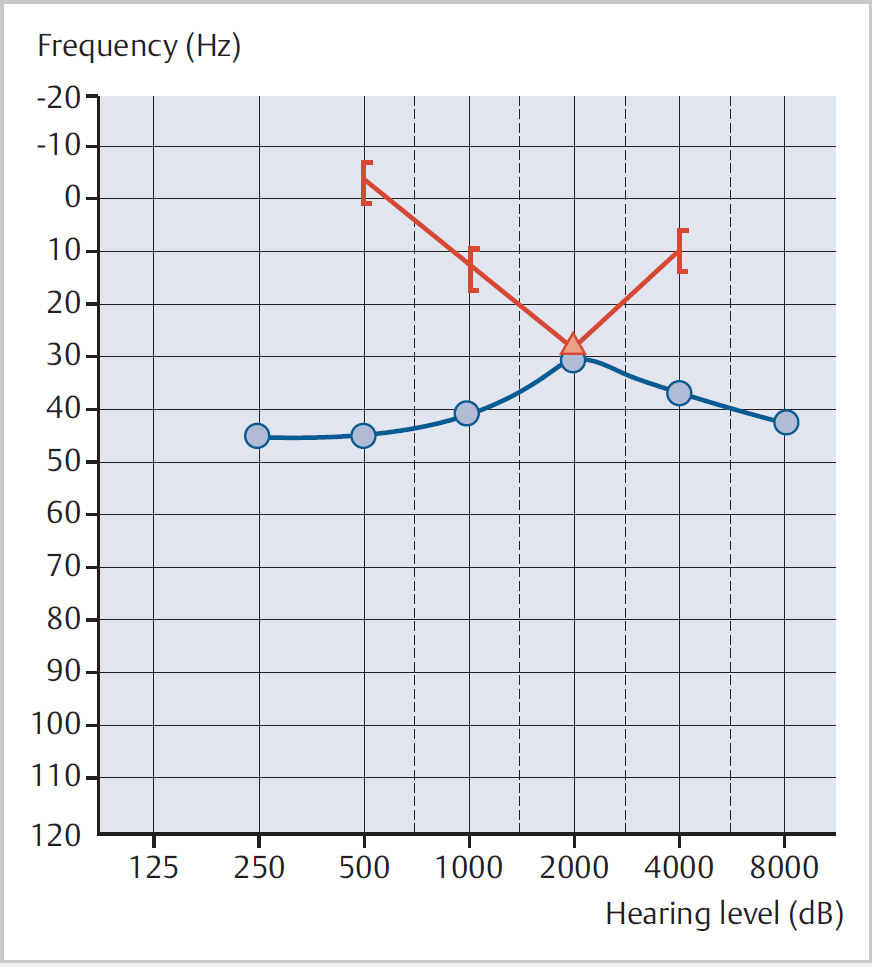
 Carhart notch (Fig. 6.1) is an elevation of bone conduction (BC) threshold of ≥10 dB at one or more frequencies (usually centred at 3 kHz); may disappear after stapes surgery or show apparent overclosure of the ABG (Carhart effect)
Carhart notch (Fig. 6.1) is an elevation of bone conduction (BC) threshold of ≥10 dB at one or more frequencies (usually centred at 3 kHz); may disappear after stapes surgery or show apparent overclosure of the ABG (Carhart effect)
 Want optimal discrimination score >70% when considering surgery
Want optimal discrimination score >70% when considering surgery
 Loss of reflex may help distinguish otosclerosis from superior semicircular canal dehiscence
Loss of reflex may help distinguish otosclerosis from superior semicircular canal dehiscence
 In earlier stages of disease may show overcompliance, followed by undercompliance (“on–off” effect)—may precede ABG
In earlier stages of disease may show overcompliance, followed by undercompliance (“on–off” effect)—may precede ABG
 Caloric stimulation can show evidence of reduced labyrinthine function, especially after stapedectomy; indicated prior to operating on second ear if significant dizziness after the first procedure
Caloric stimulation can show evidence of reduced labyrinthine function, especially after stapedectomy; indicated prior to operating on second ear if significant dizziness after the first procedure
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


