20 Otosclerosis
A Brief History of Stapedectomy
The first description of stapes ankylosis was mentioned by Valsalva in Bologna in 1740 while doing a postmortem examination of a deaf patient. He described otosclerosis as ankylosis of the stapes to the margins of the oval window.1
Meniere described a patient who was able to temporarily improve his hearing by tapping directly on the stapes with a small gold rod.2
Otosclerosis is a disorder of bone remodeling that primarily affects the otic capsule. It very frequently involves the stapes, the cochlea, and other parts of the labyrinth.3,4
Kessel from Graz is credited to be the founder of stapes surgery.5 He published a description of stapes’ mobilization as a method for the improvement of hearing in stapes ankylosis. Kessel demonstrated that opening the oval window did not necessarily result in destruction of the inner ear.
Lempert’s one-stage fenestration opened the door for successful stapes surgery.6 Finally, Shea described that the ossicular chain must be reconstructed following removal of the stapes.7 He did this by placing a tissue seal over the open oval window and using a prosthesis from the long process of the incus to the tissue seal. Thus “stapedectomy” came into existence.
Epidemiology
Otosclerosis is a primary and exclusive disease affecting only the otic capsule and the ossicles. Otosclerosis is a localized disorder of bone metabolism of otic capsule avascular enchondral bone that is characterized by disordered resorption and deposition of bone. Otosclerosis occurs only in the temporal bone.8
Etiology
The exact etiology of otosclerosis is not known at this time. Postulated theories are hereditary factors, endocrine and metabolic factors, and vascular factors. More recently the measles virus (MeV) has been implicated.
Alterations in vascularity (either an increase or a decrease in blood supply) have been postulated by Witmaack,9 Wolff,10 and Mendoza and Ruis11 to play a role in the etiology of otosclerosis. Intrinsic and extrinsic mechanical stresses as the result of an erect posture were one considered Mayer12 as a cause of otosclerosis, because the petrous pyramid is located at the base of the skull. This has not been proved. Fowler13 suggested that otosclerosis might be an expression of a general mesenchymal hypoplasia. This was further supported by Ogilvie and Hall who postulated that otosclerosis was a local manifestation of osteogenesis imperfecta.14 In recent times viral infections and autoimmune factors have also been postulated to trigger the otosclerotic processes.
Ruedi demonstrated shunts between the vascular system of the otosclerotic bone and inner ear, and suggested that venous stasis from these shunts might be responsible for sensorineural hearing loss.15
Clinical Presentation
Age of Onset
Clinical otosclerosis is commonly seen between the ages of 30 and 40 with the average age of presentation being 33 years of age.16 DeJuan comparing the age of onset among various age groups noted that 28% of cases occurred between the ages 18 and 21, 40% presented between the ages 21 and 30, and 22% presented between the ages 31 and 40.17 The onset of hearing loss is usually between the fourth and fifth decade, with a higher prevalence in women than men in the ratio of 2:1. Hearing impairment reaches its maximum in the third decade and then usually remains stable.18
A study by Thys and Van Camp19 shows that the average age of patients is increasing possibly because of general improved health awareness, the use of low dose of contraception, changing socioeconomic factors, and measles vaccination strategies.20
Prevalence
The prevalence of otosclerosis has been reported as 0.1 to 1% with an average of 0.3%.21 Autopsy studies have found histologic otosclerosis in 5 to 18% of the general population.22 Jahn and Vernick stated that 10% of Caucasians develop histologic otosclerosis and 1% go on to develop clinical otosclerosis.23 Shambaugh found that histologic otosclerosis was 10 times more common than clinical otosclerosis.24 Friedmann25 and Morrison,26 however, found the incidence to be approximately 2%. Declau et al27,28 found that in a large study of temporal bones of European origin showed a prevalence of 2.5% with no difference between the sexes.
Race
Otosclerosis is more commonly found in Caucasians. Clinical otosclerosis has been reported to be present in 1% of the population of the United Kingdom and that too among white females.29 Guild reported histologic evidence of otosclerosis in 18.5% of middle-aged white women, 9.7% of adult white men, and only 1% of adult blacks.30 Cawthorne found that otosclerosis was more prevalent in fair-haired men than in dark-haired men.31 The prevalence of otosclerosis is low among Asians,32,33 Japanese,34 Chinese, and Indonesians.35 In a comparative study conducted in Hawaii, Joseph and Frazer found the incidence to be more prevalent in Caucasians than in Japanese.36 Rosen and coworkers did not find clinical cases of otosclerosis in the Sudan.37 However, among the Todas in India the estimated prevalence of otosclerosis was found to be 17%. Kapur and Patt emphasize the custom of consanguineous marriages, a custom among the Todas.38 Consanguinity would then appear to influence the data retrieved. The prevalence of otosclerosis in American Indians is extremely low all across the American continent.39 Wiet evaluated a large number on American Indian groups and found that only 10 individuals underwent stapedectomy, of which only 3 had confirmed otosclerosis.40 This figure represented only a tiny fraction of the entire population examined. Tato and colleagues evaluated 5000 American Indians and found no cases of otosclerosis.41 When there is a racial mixture, however, otosclerosis begins to manifest itself.42
Gender
Otosclerosis is thought to be more prevalent in women. Schmidt43 quoted a female preponderance of 72.5%, whereas Shambaugh44 found an incidence of 68%, and Cawthorne45 an incidence of 67% of women who developed otosclerosis. As otosclerosis is not a genetically sex-linked characteristic, a ratio of 1:1 would have been expected. However, this has not been found to be true. Endocrinologic factors have been suspected in women. Hueb et al found a higher incidence of bilateral otosclerosis in women than in men thus prompting them to believe that women would be more likely to seek medical advice than men.46 This might possibly account for the apparent gender predisposition.
Otosclerosis and Pregnancy
Otosclerosis becomes evident during the childbearing period of life. Walsh found no evidence of a relationship between hearing loss, pregnancy, and otosclerosis.47
Does Otosclerosis Present only as a Conductive Hearing Loss?
A progressive conductive hearing loss in adults is typical of the way otosclerosis presents.48 This is due to the fixation of the stapedial footplate along its anterior annulus. On rare occasions otosclerosis can be associated with sensorineural hearing loss.49 This is due to “cochlear otosclerosis.” It is thought that some individuals may present with cochlear otosclerosis in the absence of a conductive hearing loss. Many postmortem studies of human temporal bones have shown evidence of otosclerosis without presenting with either a conductive or sensorineural hearing loss. This is known as histological otosclerosis.
Histologic Otosclerosis
Although less than 1% of the population develops clinical otosclerosis, the finding of an otosclerotic focus at autopsy is much more common. Histologic otosclerosis is a disease process without clinical symptoms or manifestations and can only be discovered by routine sectioning of temporal bones at autopsy (Fig. 20.1).30 Clinical otosclerosis is otosclerosis of a site where it causes a hearing loss, which may be conductive or sensorineural or mixed. Histologic otosclerosis has been reported as 8.3 and 11% in large random autopsy series. Clinical otosclerosis can be divided into three categories.19
Similar Disorders
Otosclerosis or otosclerotic-like lesions of the footplate and otic capsule have been observed in other inherited bone disorders. Otosclerosis is also seen in some patients with osteogenesis imperfecta who commonly develop conductive hearing losses. The lesions in the temporal bone appear similar to those of otosclerosis,50 although some patients have lesions consisting of diminished calcification and microfractures. The bony lesions of Paget disease in the otic capsule may appear similar to otosclerosis, although their distribution within the temporal bone is distinct. Large multinucleate osteoclasts are much more prominent in Paget disease than in otosclerosis. It must be stated that the conductive hearing losses sometimes associated with Paget disease are not due to ossicular lesions, but may be due to the loss of mineral density in the otic capsule.51 There is recent evidence from linkage studies that chromosome 18 carries a predisposition gene for Paget disease.52 In addition there is compelling evidence of a viral etiology in Paget disease.53 Paget disease may cause conductive and/or sensorineural hearing loss by involvement of the otic capsule and ossicles. Otosclerotic-like changes have also been described in CamuratiEngelmann disease (CED). CED or progressive diaphyseal dysplasia is a rare disorder of rapid bone turnover, diaphyseal hyperostosis, and muscle hypoplasia. Affected individuals commonly experience mixed hearing loss and vertigo. Radiologically, lesions similar to otic capsule otosclerosis have been seen.54
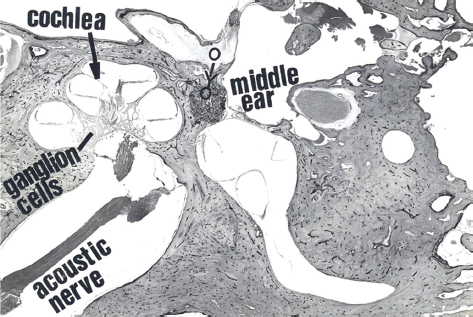
Figure 20.1 Section of human temporal bone with focus of otosclerosis (O). Note that it is also situated anteriorly.
Sites of Involvement
Any part of the bony labyrinth may be affected by otosclerosis. Otosclerotic foci are commonly found in front of the oval window. This location has been reported in 80 to 90% of temporal bones with otosclerosis.30 The focus extends and fixes the footplate by infiltration. Initially this may be by fibrous ankylosis, but later on bony ankylosis occurs resulting in total footplate fixation, while the entire footplate can be involved it is more common for the anterior portion of the footplate to be involved leaving the center intact.
The second most common site is the round window. Rarely will the round window be occluded by otosclerosis, with complete obliteration of the round window accounting for 6% of temporal bones examined.46 Reports of round window involvement range from 30 to 50%. However, it was also noted that in spite of being very close to the round window it merged in approximately 12% of cases.16 The surgical findings of extensive otosclerosis obliterating the round window have been reported to be approximately 1%. Shea and Farrior have reported this finding in 30,000 patients who underwent stapedectomy.55 Schuknecht and Barber reported involvement of the round window in 30% of cases of clinical otosclerosis and 17% of temporal bones of histologic otosclerosis.56
Otosclerosis usually affects both temporal bones symmetrically. Nylen found that 70 to 80% of cases were involved bilaterally and were symmetrical in the areas of involvement.57
Histopathology
Light Microscopy
Early phases are characterized by resorption of bone around blood vessels with an increase in space and size around vascular channels. Vascular spaces become wider. There is a decalcifying process related to the lacunar system and osteophytes. The initial stages are characterized by diffuse or patchy demineralization that coincides with preotosclerotic lesions in light microscopy.58,59 The blood vessels in the marrow spaces are increased and become dilated. If the active focus reaches the periosteal surface of the promontory, dilated blood vessels may cause a reddish pink glow which can be seen through the tympanic membrane. This is known as Schwartze sign. Schwartze sign represents vascular shunts between vessels in the otosclerotic focus and the submucosal vessels of the promontory.
Otosclerotic foci may appear as dense mineralized bone (sclerotic bone) or as active well-vascularized bone (spongiotic bone). One of the earliest manifestations of otosclerosis is the “blue mantle” within the otic capsule. Blue mantles are basophilic staining regions that are seen in the otic capsule near regions of otosclerosis in temporal bones that have been stained with hematoxylin and eosin.60,61 Blue mantles (of Manasse) are nonspecific histologic changes characterized by plexus-like projections. They are formed by resorptive spaces in the otic capsule surrounding vascular spaces which stain markedly with the blue of hematoxylin and have a mantle-like appearance, hence the name. They may be the earliest histologic evidence of otosclerosis and may occur in isolation. These regions probably represent bone that has been remodeled recently. This basophilic bone may be new bone that has been deposited in a Howship lacuna after osteoclastic resorption in the vicinity of a blood vessel or merely a change in the staining pattern of bone adjacent to the bone lining cells of vascular spaces.
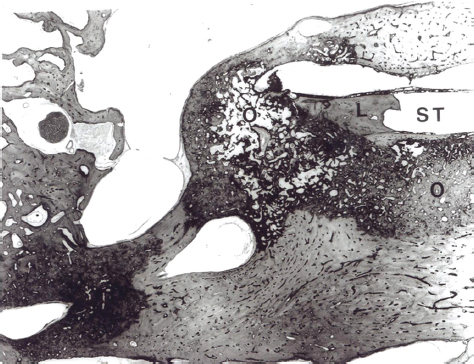
Otosclerotic remodelling distorts the contours of the labyrinth and ossicles (Figs. 20.2 and 20.3). Otosclerotic bone replaces normal enchondral bone and can become exophytic and extend into the middle ear and into the perilymphatic spaces. Within an active otosclerotic focus, osteoclasts and osteoblasts can be seen. The otosclerotic focus is made up of bone formation by osteoblasts, bone destruction by osteoclasts, vascular proliferation, and a stroma of fibroblasts and histiocytes.
The most common location of an otosclerotic focus is the area of the otic capsule anterior to the stapedial footplate (the region of the fissula ante fenestram).56 Otosclerotic foci have been found only in the temporal bone. Involvement of the otic capsule without involving the ossicles is rare.
Electron Microscopy
Light and electron microscopy studies reveal that the majority of cells present within active otosclerotic lesions are mononuclear and appear to represent osteoblasts and osteoclast precursors. The other common cells found in active lesions are histiocytes and tissue macrophages. There is a distinct absence of acute inflammatory cells. In active lesions the commonest cell type seen are osteoclasts. An extremely common feature seen in active lesions is the frequent disruption of osteoblasts with marked dilatation of the endoplasmic reticulum. Less active lesions display new woven bone formation with hypercellularity often with more than two cells situated within a single lacuna. The extracellular matrix consists of disoriented collagen fibrils with a normal banding pattern. Of particular significance is the presence of undulating filamentous structures within the dilated endoplasmic reticulum, cytosol, and occasional nuclei of osteoblasts and preosteoblasts in active lesions. They are morphologically similar to MeV nucleocapsid, and the nucleocapsid structures seen in subacute sclerosing panencephalitis. Unlike Paget disease viral-like structures have not been observed within the osteoclasts or osteoclast nuclei.62,63
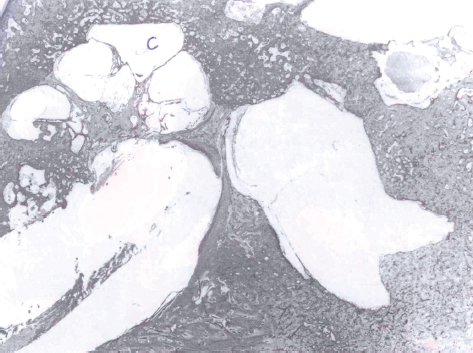
Figure 20.2 Extensive otosclerosis distorting the cochlea (C).
Otosclerosis: A Disease of Altered Localized Bone Remodeling
Stages of Otosclerosis
Most authors describe several stages of otosclerosis. They are usually categorized into “active” and “inactive” otosclerosis. However, both stages may occur together in the same temporal bone often at the same site.
Active Stage
Typical features of this stage are characterized by the presence of vascular spaces containing fibrous tissue, osteoclasts, and osteoblasts. The process at this stage is one of “otospongiosis” as new bone formation is initiated. This new bone is termed “woven bone.” There is usually a clearly defined boundary between normal and abnormal bone. The growth of the otosclerotic lesion may be diffuse with finger-like projections which are resorption spaces produced by osteoclasts dissolving some of the perivascular bone. These spaces fill up with otosclerotic bone and are referred to as “blue mantles.”
The clinical correlate of the active stage is a positive Schwartze sign. A pale pink glow often referred to as “flamingo pink” will be seen through the tympanic membrane. A sensorineural hearing loss may begin to present especially if cochlear otosclerosis is present.
Inactive Stage
In this stage there is a pattern of highly mineralized bone that is present. Osteoclasts have disappeared but osteoblasts will be seen. Vascular spaces may get obliterated by new bone formation. Lamellar bone which is formed in this stage is very thick and cellular as compared with normal bone.
The clinical correlation in this stage is when a conductive hearing loss begins to manifest itself.
Genetics of Otosclerosis
Otosclerosis has long been thought to have a genetic factor. Most genetic studies on families with otosclerosis support a pattern of autosomal dominant transmission with incomplete penetrance.64,65 There is growing evidence that suggests that otosclerosis may be a heterogenetic disease, with the typical clinical phenotype arising from more than one possible genetic defect.66 Evidence that supports a genetic basis comes from studies on monozygotic twins in which evidence of otosclerosis was found in nearly all the cases.67 Linkage studies between otosclerosis and the ABO M:N and Rh blood groups and half the globulin genotypes have failed to demonstrate evidence of linkage.
Recently linkage analysis of a large kindred from India with a presumptive diagnosis of otosclerosis revealed linkage to a region of chromosome 15q.68 These investigators suggest that the gene for aggrecan, an extracellular matrix protein found predominantly in cartilage may be a possible candidate gene. However, other families have been examined specifically for evidence of linkage to this region, but no evidence supporting this theory was found. This again supports the concept of a heterogenetic disorder. Thalmann and colleagues69 detected possible alterations in collagenous proteins in otosclerotic tissues. There is a recent evidence to suggest that in a small number of cases otosclerosis may be related to gene defects in COL1A1 gene, one of the genes that code for type 1 collagen, the major collagen component of bone. Association analysis has revealed an association between the COL1A1 allelic expression in cultured fibroblasts from individuals with clinical otosclerosis that is either familial or sporadic. Analysis of COL1A1 allelic expression in cultured fibroblasts from individuals with clinical otosclerosis has shown that in a small percentage of cases, ranging from 10 to 20%, one of the COL1A1 alleles is expressed in extremely low reiteration. This is similar to that which is seen in many cases of mild (type1) osteogenesis imperfecta. This suggests that in a small percentage of cases the underlying genetic mechanism may be very similar to that of osteogenesis imperfecta.70 The hearing loss in persons with type I osteogenesis imperfecta occurs almost exclusively in association with COL1A1 defects and occurs in 50% of affected persons. It shares the same autosomal dominant inheritance with incomplete penetration, as seen with otosclerosis
Mazzoli et al examined sporadic and familial (hereditary) patients suffering from otosclerosis and report that in sporadic cases of otosclerosis a genetic cause cannot be excluded, because of the possibility of a different mode of inheritance, new mutations, or the absence of expression in family members.71 They also state that environmental factors may be responsible for the high degree of variability between families.
Although a strong familial background exists, 40 to 50% of all clinical cases have been reported to be sporadic.72 Morrison and Bundey explained most sporadic cases by reduced penetrance.73 They also pointed out toward possible new mutations and other modes of inheritance besides autosomal dominant. Gordon suggested complex inheritance to explain the sporadic cases.21 Complex multifactorial diseases are caused by an interaction of several environmental and genetic factors. It is thus clear that autosomal dominant forms exist often with reduced penetrance. Complex genetic diseases and monogenic diseases need a different research strategy to identify the genes involved.
Role of Measles Virus in Otosclerosis
There is, in recent times, increasing evidence that a paramyxovirus may likely be the cause of Paget disease of the bone. Paget disease of the bone and otosclerosis are of similar pathologies. This in turn led researchers to look for evidence of a similar etiology for otosclerosis. This has led to an increasing body of evidence that the MeV is a possible etiologic agent in the cause of otosclerosis. The evidence includes transmission electron microscopy that has demonstrated measles-like structures within active otosclerotic foci. Other evidence includes immunohistochemical evidence of measles antigen in active foci, reverse transcription polymerase chain reaction amplification of measles RNA from otosclerotic lesions recovered from fresh and stored tissue samples.74 Additional evidence includes elevated levels of immunoglobulin (Ig)-G specific for MeV antigens in the perilymph of patients suffering from otosclerosis. This was not found in the control group of patients.75
The results of this study suggest that a persistent MeV infection together with an underlying hereditary predisposition may lead to the development of clinical otosclerosis. This would help explain the sporadic nature of the disease as well as the observed incomplete penetrance of the phenotype. Filamentous structures resembling paramyxoviral necleocapsids in osteoblast-like cells were reported. MeV RNA in otosclerotic tissue was detected with reverse transcriptase polymerase chain reaction70 suggesting that the initial otosclerotic lesion may be initiated by measles infection of the “globuli interossei,” which can account for the sole predilection of the temporal bone. The establishment of persistent infection may be related to the relatively quiescent metabolic state or terminal differentiation of the osteocytes or chondrocytes within the “globuli interossei,” which results in restricted expression of the measles genome with little or no expression of late viral genes critical for complete viral assembly and escape.76 Infected cells produce factors that destabilize the extracellular matrix and lead to activation of the remodeling process. The progression and extension of the abnormal remodeling process is dependent on an underlying genetic defect in collagen metabolism. There may be multiple different mutations within the COL1A1 gene and in other genes within the collagen metabolism pathway that result in the generation of an unstable extracellular matrix with a high propensity for remodeling. Although multiple different mutations in COL1A1 may result in null expression of the mutant alleles, the downstream effect on other related factors that are critical determinants in the remodeling process may vary among mutations and produce a varied spectrum in clinical and histologic severity. These are new and interesting theories. However, additional studies will be required to establish which loci and genes are related to the development of otosclerosis. Furthermore, to substantiate the viral cause of otosclerosis, the virus will need to be isolated from the otosclerotic tissue.
There is convincing evidence for a chronic inflammatory reaction in otosclerosis. MeV involvement was demonstrated in morphological, biochemical, and immunological studies.77 Epidemiological data show a decrease in occurrence of otosclerosis following the introduction of MeV vaccination in 1970 in Germany. Taken together there is a strong association between MeV and otosclerosis.
Another aspect is that only humans and primates are hosts of MeV because of their complimentary cell surface structures (CD46 and CD150) and that MeV shows a certain organotropism to the otic capsule. This can explain that till date there is no good animal model for otosclerosis.
Certain authors regard the presence of MeV as an epiphenomenon and not as a causative agent.78 They also state that either way a genetic predisposition has to be presumed in both the cases.
Niedermeyer and Arnold look at MeV as to its causative or association effect. They concluded that the development of otosclerosis is triggered by a persistent MeV infection, and MeV vaccination could prevent otosclerosis to a certain extent.79
Role of Autoimmunity in Otosclerosis
Yoo et al first reported increased type II collagen antibodies in patients suffering from otosclerosis.80 On the other hand, Sorenson et al and Lolov et al found no difference in otosclerotic patients compared with controls.81,82 In another later report, Joliat et al and Bujía et al found significantly elevated levels of antibodies to types II and IX in otosclerotic patients compared with controls.83,84 Yoo et al suggest that type II collagen immunity induced in rats leads to bone lesions similar to those seen in otosclerosis.85 In a separate and identical study Harris et al found no such lesions.86 In view of such conflicting data a definite role of autoimmunity remains uncertain.
History and Physical Findings
The commonest symptom is a hearing loss, usually conductive in nature. A positive family history is found in most patients. The clinical onset is usually in early or mid-adult life. The hearing loss is usually bilateral. Vestibular symptoms are not common presentations. On occasion the patient may complain of tinnitus.
It is possible to encounter patients who may suffer from chronic otitis media and otosclerosis simultaneously. In situations where the otosclerotic focus is active, a pinkish glow may seem to emanate from behind the tympanic membrane. This is known as “Schwartze sign.” This is because of increased vascularity. When the focus is inactive, the tympanic membrane appears normal. Otherwise the otological examination is normal. On tuning fork tests the patient will present with bone conduction (BC) better than air conduction (AC). This is known as “Rinne test negative.” When the patient has otosclerosis in both ears Rinne test will likely be negative in both ears. Webers test will lateralize in both ears. Other conditions can present with conductive losses. These are ossicular discontinuity, Paget disease, and tympanosclerosis.
Audiological Evaluation of the Patient with Otosclerosis
The audiological pattern in otosclerosis is unique. The patterns of abnormalities can be directly explained by alterations in the middle ear transfer function produced by stapes fixation.87
Pure Tone Audiometry
This is the most basic test that should be performed in any patient presenting with impairment in hearing. It is a subjective test and the results can vary from laboratory to laboratory.
Air Conduction
The most prominent audiologic characteristics of otosclerosis are elicited with the use of low frequency stimuli.88 The primary acoustic consequence of otosclerosis in its early stages is the increase in the stiffness reactance component of the total middle ear impedance. This results in reduction of transmission effectiveness for low frequencies as seen in elevated thresholds. Another effect is that the resonant frequency of the middle ear is elevated.89
In the early stages a gradually progressive low frequency conductive hearing loss is first seen. Initially patients may be unaware of such a hearing impairment until it crosses the 25 dB range. The hearing loss may be confined to frequencies below 1000 Hz. High frequencies are typically unaffected at this stage. This characteristic rising audiogram configuration has been referred to as the “stiffness tilt.”
As the footplate becomes completely fixed and the otosclerotic focus proliferates, a mass effect is added to the audiogram. The low frequency hearing loss doesn’t increase and appears to stabilize. However, the hearing loss progresses in the high frequencies and there is a gradual widening of the air bone gap. The audiogram configuration now changes to a flat pattern from the upward sloping pattern that it had in the early stages. In the absence of cochlear involvement, the pure conductive hearing loss produced by the complete stapes fixation is limited to 60 to 65 dB with a maximum air bone gap across the frequency range.
In cochlear otosclerosis AC thresholds continue to worsen and the loss starts to become mixed or sensorineural, with the high frequencies becoming severely affected. The typical pattern of cochlear otosclerosis in the early stages is the “cookie bite” pattern where the greatest degree of hearing loss occurs in the mid-frequency hearing range and is characteristically a mixed hearing loss.88
Tinnitus is usually present in a large percentage of patients. Usage of pulsed or warbled tones may help the patient identify tinnitus from pure tone test stimuli when being tested.
Bone Conduction
While AC curves give an indication of the hearing thresholds and its configuration may give valuable clues to the diagnosis of otosclerosis in its early stages, BC audiometry is of great value in the diagnosis of otosclerosis and in selection of patients for surgery. BC is especially useful in testing patients suffering from otosclerosis. It reveals characteristics that are typical of otosclerosis and it also helps reveal the amount of cochlear reserve in each ear. This helps identify if stapedial or cochlear otosclerosis is present. This in turn helps the surgeon make a decision as to which ear he should operate and helps predict optimum postoperative results.
The “Carhart notch” (also known as the Carhart effect) is thought to be typical of otosclerosis.90,91 Carhart notch is characterized by elevation of BC thresholds of approximately 5 dB at 500 Hz, 10 dB at 1000 Hz, 15 dB at 2000 Hz, and 5 dB at 4000 Hz. It was previously thought that this was due to the inertial component of BC caused by stapes fixation. However, the contribution of the inertial component is maximal for frequencies below 800 Hz and thus a greater loss for bone conducted low frequencies might be predicted. This, however, is not borne out by clinical observation. Another more plausible explanation is that fixation of the stapes disrupts normal ossicular resonance, which in humans is around 2000 Hz (Fig. 20.4). Furthermore the normal compression mode of BC is disturbed because of the relative perilymph immobility caused by stapes fixation.92 Carhart notch is a mechanical artifact and is not a true representation of cochlear reserve. Evidence that the Carhart notch is an artifact is seen in overclosure following stapes surgery.
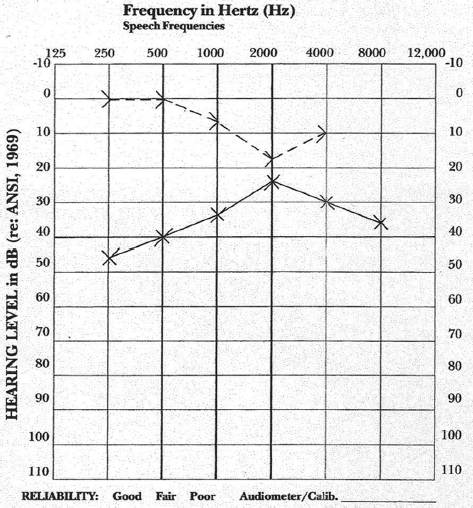
Figure 20.4 Typical pure tone audiogram of a patient suffering from otosclerosis. There is an air bone gap and a “Carhart” notch at 2 kHz.
Cross-checks on the validity of BC thresholds include careful consideration of the masking levels. Sensorineural acuity level (SAL) test is used to resolve masking dilemmas.
It must be appreciated that the Carhart notch occurs in any condition that reduces the inertial vibration of the stapes footplate during BC stimulation. One such condition is otosclerosis. It would, however, be incorrect if it is assumed that this is the only condition which can cause Carhart notch.
Carhart gives four postulates to indicate that stapes fixation induces mechanical modifications in the BC audiogram.90
1. In the Bing test, in clinical otosclerosis, there is no shift in loudness when the meatus is occluded, or when pressure is varied, as is seen in normal hearing and in sensorineural hearing loss. It is probable that the Bing test is negative in otosclerosis and on other forms of deafness because the middle ear element of BC is attenuated by the middle ear element of hearing loss.
2. It is unusual to find a patient with otosclerosis whose BC thresholds are normal.
3. Surgery improves BC thresholds and the Carhart notch disappears following surgery.
4. Animal experiments producing stapes fixation cause BC thresholds to become poorer.
It was thought that there was an abrupt shift in BC thresholds and that this may reach its full magnitude when stapes fixation has progressed to the stage where it causes a mild AC loss. Beales disagrees and has evidence of a slowly progressive increase in the size of Carhart notch.89 In chronic otitis media Carhart notch-like effects may occur but they are much less prominent than those seen in otosclerosis.
Not all high frequency BC losses are artifacts. Cochlear otosclerosis is characterized by the presence of mixed or sensorineural hearing losses in which the air bone gap is minimal. If the AC and the BC levels are roughly parallel, the elevated bone conduction thresholds probably represent a sensorineural hearing loss.
The Carhart notch is present in a wide range of frequencies and its notch was underestimated in the lower frequencies.93 The Carhart notch is not only exclusively predominant at 2 kHz, but is also seen in lower frequencies. The presence of notches in the lower frequencies in individuals with a persistent air bone gap may be indicative of other middle ear pathologies such as incus or malleus fixation.94
Kelemen and Linthicum have discovered that the severity and configuration of the pure tone audiogram do not match the frequency for frequency those areas of the cochlea.95 Sensorineural hearing losses are most commonly associated with basal turn involvement and are invariably present with endosteal layer involvement. Sensorineural hearing loss varies directly with hyalinization of the spiral ligament.
Clinical Value of Bone Conduction Audiometry
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


