20
Otosclerosis
Michael J. McKenna and Ronald K. de Venecia
Otosclerosis is a bone disease that is unique to the human temporal bone.1 One of the most common causes of acquired hearing loss, otosclerosis has a well-established hereditary predisposition, with about 50% of affected individuals having other known affected family members.2 Otosclerosis occurs within the endochondral layer of the temporal bone, usually in certain sites of predilection that are associated with globuli interossei or so-called embryonic rests. The most common site of occurrence of otosclerosis is the fissula ante fenestram just anterior to the stapes footplate.3,4 As the lesion enlarges and spreads, it encroaches on the stapes footplate and produces a conductive hearing loss (clinical otosclerosis). In some cases, the lesion may spread to involve the cochlea and result in an irreversible sensorineural hearing loss (SNHL).5,6 However, the majority of lesions do not encroach on the footplate or cochlea; such lesions remain small and asymptomatic (histologic otosclerosis).7 The small histologic foci are 10-fold more common than the larger lesions that result in clinical manifestations.8 Despite intensive investigation, the etiology of otosclerosis remains unknown.
 Pathology
Pathology
Histopathologically, the otosclerotic process is characterized by a wave of abnormal bone remodeling, resulting in the replacement of otic capsule bone with a hypercellular woven bone, which may undergo further remodeling, resulting in a mosaic sclerotic appearance. The initial remodeling process consists predominantly of mononuclear cells, including histiocytes and bone cells, many of which show degeneration with cellular lysis and release of cytoplastic contents.9 There is a distinct absence of acute inflammatory cells.10 Although the most common site of predilection is the fissula ante fenestram that lies in close proximity to the anterior portion of the stapes footplate, otosclerosis also may occur in other sites including the round window, sometimes resulting in round window obliteration. The degree of stapes footplate involvement from otosclerosis is highly variable. In the majority of cases, otosclerosis results in anterior stapes fixation without involvement of the posterior footplate or the posterior annular ligament. In many cases, as the otosclerotic process begins to develop anterior to the footplate, the footplate becomes posteriorly displaced. This results in a jamming of the posterior footplate within the oval window and the development of a lowfrequency conductive hearing loss11,12 (Fig. 20–1). With bony fixation of the footplate, there is conductive hearing loss across all frequencies. This has long been recognized by stapes surgeons, who often were reluctant to operate on patients without a negative Rinne at 512- and 1024-Hz (bone conduction louder than air conduction) prior to the advent of the laser. These patients had a higher risk for footplate mobilization or a floating footplate upon down-fracture of the stapes superstructure. In some cases, the otosclerotic lesion may overgrow the footplate, resulting in obliterative otosclerosis. It is not possible to differentiate between obliterative otosclerosis and bony ankylosis of the footplate without oval window obliteration on audiometric testing alone.
Large active otosclerotic lesions that involve the cochlear capsule and penetrate the cochlear endosteum can result in a progressive SNHL.7,13 Until recently, there was no clear explanation for the cause of the SNHL in these patients. Temporal bone studies have failed to demonstrate a loss of sensory cells, both hair cells and spiral ganglion cells, in proportion to the degree of SNHL.14,15 The only pathologic correlation between SNHL and otosclerosis has been the penetration of the cochlear endosteum with hyalinization of the spiral ligament.16 Recent investigations have revealed that the spiral ligament is a dynamic organ that plays an important role in maintaining normal cochlear physiology. It plays a critical role in the recirculation of potassium ions within the cochlea.17,18 Disturbance of this function is one plausible explanation that can account for the degree of SNHL that occurs in these patients.
When a careful history is taken, between 10% and 20% of patients relate symptoms of dizziness or vertigo.19 The symptoms are highly variable, ranging from benign paroxysmal positional vertigo, to waxing and waning disequilibrium, to vertigo of Meniere’s type. In some cases, although uncommon, otosclerosis may involve the endolymphatic duct, resulting in hydrops and symptoms of Meniere’s disease. This is important to recognize, as this is an absolute contraindication for stapedectomy, as hydrops may result in saccular dilatation, predisposing the membranous labyrinth to injury upon fenestration of the footplate. For reasons that are unclear, some patients who have a history of giddiness or waxing and waning disequilibrium without true vertigo experience an improvement in their vestibular symptoms following stapedectomy.20
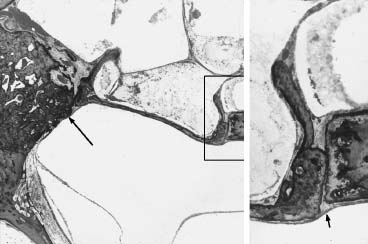
Figure 20–1 Fixation of the footplate by an anterior focus of otosclerosis (large arrow). The otosclerotic process also has resulted in posterior displacement of the footplate. Inset: Higher magnification view of the posterior footplate, which has become jammed against the bony annulus (small arrow).
 Etiology
Etiology
Although the precise etiology of otosclerosis has yet to be elucidated, significant progress has been made over the past 20 years. Fundamentally, otosclerosis is an active remodeling process of bone that occurs within the endochondral layer of the temporal bone that under normal circumstances undergoes virtually no remodeling following development.21,22 In this respect, the otic capsule is unique and different from all other bones in the body. To understand why this abnormal remodeling process occurs in the first place, it is important to first understand why the otic capsule is devoid of postdevelopmental remodeling. Sorensen et al23,24 have studied otic capsule remodeling in several species and have shown that remodeling in the otic capsule is markedly inhibited compared with other bones and that this inhibition is most prevalent in direct proximity to the inner ear. These studies have led to the hypothesis that the inner ear itself may play a direct role in the inhibition of otic capsule remodeling by producing substances that diffuse into the surrounding bone and prevent remodeling. We have recently discovered that the spiral ligament produces a compound called osteoprotegerin (OPG), which is secreted into the perilymph and diffuses into the surrounding otic capsule bone.25 OPG is a potent inhibitor of bone remodeling. It acts by inhibiting the recruitment, formation, and activity of osteoclasts, which resorb bone. Knockout mice that lack OPG have active otic capsule remodeling that closely resembles otosclerosis.26 We suspect that there are other factors involved in the inhibition of otic capsule remodeling other than OPG, although as of yet they have not been clearly defined.
One hypothesis that has gained considerable support over the past 15 years is that otosclerosis may be related to a persistent measles virus infection within the otic capsule.27 The evidence to support this hypothesis includes the demonstration of (1) viral-like particles within osteoblasts and preosteoblasts in active otosclerotic lesions by electron microscopy, (2) measles antigens within active lesions using immunohistochemical techniques, and (3) measles virus gene products in active otosclerotic lesions using reverse transcription/polymerase chain reaction techniques.28–35 This hypothesis would account for the fact that otosclerosis appears to involve only the human otic capsule, as measles virus affects only humans and closely related primates. It would also account for the significant decline in incidence of new cases of otosclerosis, which is well correlated with the measles virus vaccination.36,37
Otosclerosis is most common among whites, uncommon among Asians, and extremely rare in blacks. Otosclerosis is estimated to occur histologically in 10% of the white population and results in hearing loss in 0.5%.6 The clinical prevalence of otosclerosis is estimated to be twice as common in females as in males.38
Familial aggregation of individuals affected by otosclerosis has been recognized for many years.39,40 Most studies support a pattern of autosomal dominant transmission with incomplete penetrance in the range of 20 to 40%.41 The most compelling evidence for an underlying genetic cause for otosclerosis comes from studies on monozygotic twins with clinical otosclerosis, in which concordance has been found in nearly all cases.42 However, information does not exist on the genetic transmission of histologic otosclerosis. It is not known whether the genetic basis of inheritance is related to the formation of an otosclerosis focus within the temporal bone or the tendency for a lesion to progress once it has begun, or both. Most studies on families with otosclerosis support a pattern of autosomal dominant transmission with incomplete penetrance. A study of 65 pedigrees with otosclerosis in Tunisia suggests that otosclerosis is primarily heterogenetic, and in 13% of clinical cases studied, affected individuals who carry a dominant gene with nearly complete penetrance.43 Linkage analyses of large and unrelated families have revealed linkage to distinctly different loci, indicating that otosclerosis is heterogenetic.44–48 The otosclerosis phenotype may result from several different gene defects. Each of the families that have been studied thus far is atypical in that the penetrance is nearly complete, with approximately half of all individuals in each family being affected. Although a strong familial component exists, several studies have reported that sporadic otosclerosis represents 40 to 50% of all clinical cases.
There is evidence to suggest that some cases of otosclerosis may be related to defects in expression of the COL1A1 gene. Association analysis using multiple polymorphic markers has revealed a significant association between both familial and sporadic cases of clinical otosclerosis and the COL1A1 gene.49,50 The association has been found to increase from the 3′ to the 5′ region of the gene. Studies of the allelic expression of the COL1A1 gene in patients with clinical otosclerosis have revealed reduced expression of one COL1A1 allele in some cases, similar to that which has been described in many cases of type I osteogenesis imperfecta.51,52 Type I osteogenesis imperfecta shares both clinical and histologic similarities with otosclerosis. Approximately half of all patients with type I osteogenesis imperfecta develop hearing loss that is clinically indistinguishable from otosclerosis. It is also well known that some patients with clinical otosclerosis have blue sclera, a feature that is found in virtually all patients with type I osteogenesis imperfecta.53 The histopathology of temporal bones from patients with type I osteogenesis imperfecta is identical to that observed in patients with otosclerosis.54,55
 History of Otosclerosis Surgery
History of Otosclerosis Surgery
The history of otosclerosis surgery is among the most interesting and colorful chapters in all of otolaryngology. Students of otology are strongly encouraged to read the biography of Howard House, For the World to Hear,56 as it not only chronicles the history of otosclerosis surgery during the last century but also provides insight into the personalities of some of the great leaders in our field. Stapedectomy was first introduced as a treatment for otosclerosis in the late 1800s by Blake and Jack in Boston and shortly thereafter by DeRossi in Italy. Although initial results were encouraging, there were cases of infection that resulted in meningitis and death and led to a condemnation of all stapes surgery by prominent leaders in the field. It was John Shea Jr. in 1956 who, with the benefit of improved instrumentation and employing the operating microscope, reintroduced stapedectomy using a polyethylene strut and vein graft. Although most otologists were skeptical at the time, within 10 years it became widely apparent that stapedectomy was the most reliable and safest technique for the restoration of hearing in patients with otosclerosis and stapes fixation. What followed was one of the most exciting periods in modern otology and occupied much of the agenda of the American Otological Society, including papers and discussions. There has been an evolution in the two fundamental steps of the operation: fenestration of the oval window and introduction of a prosthesis. The fenestration of the oval window evolved from a technique of total stapedectomy with removal of the stapes footplate with micropicks; to partial stapedectomy; to the small fenestra technique, initially using microdrills; and ultimately to the introduction of otologic lasers. Similarly there has been an evolution in the development of prostheses from polyethylene tubes to fat- and gel-wires and ultimately to the piston prostheses of varying sizes and materials. Throughout this period, there have been significant improvements in the operating microscope, including superior optics and brighter illumination. Although it is not clear what the future holds in terms of further technologic innovations, with the advancements in robotic and computer technology, the evolution of stapes surgery will certainly continue.
 Diagnosis
Diagnosis
History
Most often, otosclerosis results in a gradually progressive, conductive, or mixed hearing loss. In approximately 70% of cases, both ears are affected over time. Typically, onset occurs between the ages of 20 and 40. Juvenile onset is known to occur but is relatively uncommon and warrants further investigation of other possible causes. A progressive, purely SNHL may also occur as a result of cochlear otosclerosis, but this too is relatively rare and warrants investigation of other possible causes. In patients with a past history of infection, other possible causes of the conductive hearing loss need to be considered. A family history of hearing loss can be elicited in many cases. A family history of otosclerosis or another family member who has undergone a successful stapedectomy makes the diagnosis of otosclerosis far more likely.
A history of dizziness or vertigo, although uncommon, is certainly not rare. Approximately 10 to 20% of patients, if questioned, give some past history of vestibular symptoms. The range of vestibular symptoms is highly variable, including positional vertigo, waxing and waning disequilibrium, and severe vertigo of the Meniere’s type. Although rare, Meniere’s disease may occur in patients with otosclerosis, and it is essential to establish this prior to considering stapedectomy. As mentioned above, stapedectomy in a patient with otosclerosis and Meniere’s disease is contraindicated. Some patients with superior canal dehiscence syndrome present with both conductive hearing loss and vestibular symptoms. The conductive hearing loss may closely mimic that seen in otosclerosis.57 Often these patients complain of severe autophony. A diagnosis of superior canal dehiscence syndrome should be suspected in a patient with a low-frequency conductive hearing loss with bone conduction thresholds that rise above 0 dB. Acoustic reflex testing also is helpful in differentiating otosclerosis from superior semicircular canal dehiscence (SSCD) syndrome as it should be present in SSCD and abnormal in otosclerosis.
Physical Examination
Otoscopic examination usually reveals normal-appearing tympanic membranes. Pneumo-otoscopy with magnification is helpful in both ruling out the presence of a middle ear effusion and assessing malleus mobility. The presence of tympanosclerosis or a retraction pocket should lead to the consideration of conductive hearing loss of other cause. Occasionally, a vascular hue can be seen near the stapes, known as Schwartze’s sign (Fig. 20–2), which is the result of hyperemic middle ear mucosa over an area of active otosclerosis.
Tuning fork tests, both Weber and Rinne at 512 Hz and 1024 Hz, should be performed. The results should be correlated with a complete audiogram.
Audiologic Testing
All patients undergo standard audiometry including puretone audiometry with air and bone testing and speech discrimination testing. It is important that true bone conduction thresholds be determined as this may be helpful in differentiating the conductive hearing loss in otosclerosis from that seen in SSCD. Patients with SSCD often demonstrate bone conduction thresholds above 0 dB. If the audiologist stops testing at 0 dB, this will not be appreciated. Until recently we had abandoned stapedial reflex testing as part of the standard audiometric evaluation in patients with conductive hearing loss. However, with the recognition of SSCD as a potential cause for conductive hearing loss and the fact that patients with SSCD have normal acoustic reflex testing, we have begun testing the stapedial reflex in these patients.
Early in the development of conductive hearing loss from otosclerosis, patients typically demonstrate a low-frequency conductive loss that narrows in the high frequencies. This low-frequency conductive loss is related to the posterior displacement of the footplate as a result of an encroaching anterior otosclerotic lesion. The jammed footplate with impaired mobility maintains the capacity for transmission in the higher frequencies. With bony ankylosis of the footplate, the conductive hearing loss flattens across all frequencies.

Figure 20–2 Schwartze’s sign.
It is not unusual for patients with otosclerosis and conductive hearing loss to have a depression in the bone conduction thresholds that is most significant at 2000 Hz, termed a Carhart notch, which is thought to represent an audiologic artifact, possibly from an affect of stapes fixation on middle ear resonance. It often resolves following a successful stapedectomy. For this reason, it is important that all patients who are tested postoperatively also have both air and bone thresholds tested.
Word recognition scores or speech discrimination is usually normal unless there is a significant sensorineural component to the hearing loss.
 Surgical Management by Stapedectomy
Surgical Management by Stapedectomy
Indications
In general there should be a conductive hearing loss of at least 25 dB in frequencies 250 to 1 kHz or higher as determined by both audiometry and the presence of a negative Rinne at 512 Hz (bone > air conduction). The presence of a concomitant SNHL in the affected ear is not necessarily a contraindication for stapes surgery. It does, however, require some thoughtful consideration. If a hearing aid will still be required after successful stapedectomy, the procedure may be considered if it would result in improved performance with amplification. If both ears are involved, generally the poorer hearing ear is operated first. If the operation is a success, the patient may be a candidate for a contralateral stapedectomy after a year has gone by and the hearing in the operated ear has remained stable.
In some cases of advanced otosclerosis it may be difficult on the basis of audiometry to determine whether or not a patient might benefit from a stapedectomy. Often the tuning fork tests are more helpful than the audiogram under such circumstances. Often these patients have very poor speech discrimination scores preoperatively because of an inadequate presentation level, which is at the limit of the audiometer. These patients may demonstrate a dramatic improvement in their speech discrimination following stapedectomy.
Contraindications
Stapedectomy on an only-hearing ear is almost always contraindicated. One exception may be a case of a profound mixed loss, which is beyond the level of benefit of a conventional hearing aid. Such a patient would otherwise be considered a cochlear implant candidate, and a stapedectomy may be considered as the first option prior to proceeding with implantation. Stapedectomy is contraindicated in cases of active infection of the middle ear or external auditory canal. It is also contraindicated in patients with tympanic membrane perforations. Patients in whom vestibular function is absolutely critical for their employment should be given special consideration. Stapedectomy is contraindicated in ears with Meniere’s disease and relatively contraindicated in patients with a contralateral otologic problem, which may threaten the hearing in their contralateral ear over time.
Informed Consent
All patients being considered for stapedectomy should be counseled regarding the potential benefits of amplification as a nonsurgical option to help improve their hearing. Patients should be made aware that there is no window of opportunity and that any delay in deciding to proceed with surgery does not impact the eventual result. After describing the details of the surgical procedure in a manner that the patient can easily understand, all of the potential risks should be discussed, including failure of the surgery to improve hearing by virtue of residual conductive hearing loss; creation of a SNHL, either partial or complete; vestibular dysfunction; perforation of the tympanic membrane; facial nerve dysfunction; disturbance in taste; development of a perilymph fistula; and late failure of the procedure. It is prudent to inform all patients to expect some disturbance in taste related to manipulation of the chorda tympani nerve, as this occurs in most cases. Thus the patient will be reassured that this was expected and does not constitute a complication. Nevertheless, this issue deserves further discussion and is included below under Early Postoperative Complications.
Primary stapedectomy can be performed with either local or general anesthesia. The primary advantage of local anesthesia is the time saved in putting patients to sleep and waking them up. There may be some advantage in monitoring vestibular symptoms, but this is certainly not borne out by differences in results with local and general anesthesia. General anesthesia provides assurance of absolute control of head motion and prevention of pain. In recent times, over half of our patients have selected general anesthesia.
Positioning
The patient is placed in a supine head-hanging position with the head turned to the opposite shoulder. A downward tilt of the head of about 10 to 15 degrees helps bring the ear canal into a straight upright position and places the tympanic membrane in an approximate horizontal plane. A head rest that is separable from the remainder of the operating table is preferred to facilitate appropriate positioning. The headrest is fitted with a fastening mechanism for a self-retaining speculum holder with sufficient degrees of freedom to allow manipulation of the speculum during surgery. The external auditory meatus is injected in four quadrants with 1% Xylocaine with 1:100,000 epinephrine. The bony canal is then injected at 12 o’clock and 6 o’clock with 2% Xylocaine with 1:50,000 epinephrine.
Surgical Technique
Exposure
A posterior tympanomeatal flap is developed such that there is some redundancy in the posterior-superior aspect to cover the area of bone that may be curetted to provide optimal visualization of the oval window (Fig. 20–3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


