Otoplasty: Anatomy, Embryology, and Technique
Steven Ross Mobley
Nathan Todd Nelson Schreiber
In addition to its function in directing sound to the tympanic membrane, the ear plays a complementary role in one’s appearance. If abnormal in appearance, however, the ear can command unwanted attention, drawing an observer’s eyes away from the rest of the face. Classically, auricular anomalies have resulted in significant social stigma. In a criminology text from 1876, author Cesare Lombroso wrote, “nearly all criminals have jug ears” (1); a number of overtly discriminatory texts from this period contain overtly belittling references to prominent ears as well (2). Although such beliefs are, for the most part, not consciously encouraged today, they persist in more subtle forms. In popular culture, large ears are often exaggerated in jest for cartoons and caricatures. For children especially, prominent or malformed ears may be the subject of ridicule, possibly affecting self-esteem and psychosocial development. It is for this reason that surgical correction of the anomalous ear is often sought.
The goal of otoplasty is to create a more natural appearance and position of the ear. Its origins can be traced back to India in 800 bc, when reconstruction of the lobule using a local cheek flap was first described by Indian surgeon Sushruta (3). Reconstruction of larger ear defects using postauricular scalp flaps was not described until centuries later in textbooks, by Italian surgeon Gaspare Tagliacozzi in 1597, and again by Prussian surgeon Johann Friedrich Dieffenbach in 1845 (4,5,6). The first truly cosmetic otoplasty, however, was performed in 1881, by American surgeon Edward Ely, on a 12-year-old boy who was ridiculed for having a prominent ear (7,8). In the ensuing years, multiple variations of this operation have been described and provide a number of techniques that may be used to create a more anatomically natural-appearing ear. Given the multitude of techniques, one must understand normal auricular anatomy as well as the goals of surgery in order to successfully perform otoplasty.
ANATOMY AND EMBRYOLOGY
The auricle is essentially an extension of fibroelastic cartilage from the external auditory canal that is covered by perichondrium and a thin layer of skin. The skin is directly adherent to perichondrium anteriorly but is separated from perichondrium by loose areolar tissue posteriorly. Cartilage is deficient at the lobule as well as between the tragus and the beginning of the helix anteriorly. Projections of cartilage from the anterior and inferior ends of the helix are called the spina helicis and the cauda helicis, respectively. Attached to portions of the cartilage itself are six internal auricular muscles: the helicis major, helicis minor, tragicus, and antitragicus along the lateral side of the cartilage and the transversus auriculae and obliquus auriculae along the medial side of the cartilage. Three external auricular muscles, anterior, superior, and posterior, provide additional fixation to the temporal bone and, through the facial nerve, the ability to move one’s ear. Auricular sensation is provided by multiple nerves. C2 and C3 through the greater auricular nerve provide sensation posteriorly at the helix, antihelix, and lobule. Cranial nerves IX and X provide sensation to the conchal bowl and posterior external auditory canal. The auriculotemporal branch of the mandibular division of the fifth cranial nerve provides sensation to the tragus, superior helix, and superior and anterior external auditory canal. The superficial temporal, posterior auricular, and occipital branches of the external carotid artery provide the auricle’s arterial supply, while the superficial temporal vein, retromandibular vein, external jugular vein, and, in some cases, the mastoid emissary vein provide venous drainage. Lymphatic drainage occurs through the parotid, posterior auricular, and cervical levels 2 and 5 lymph nodes (9). The normal anatomy of the auricle is shown in Figure 190.1.
The external ear develops from six swellings called hillocks of His, which are present at 6 weeks’ gestation. The first
three hillocks of His develop from the first branchial arch into the tragus, helical crus, and helix, while the second three hillocks of His develop from the second branchial arch into the antihelix, antitragus, and lobule (Fig. 190.2). The hillocks of His are fused by 12 weeks’ gestation and reach a final shape around 20 weeks’ gestation (9,10).
three hillocks of His develop from the first branchial arch into the tragus, helical crus, and helix, while the second three hillocks of His develop from the second branchial arch into the antihelix, antitragus, and lobule (Fig. 190.2). The hillocks of His are fused by 12 weeks’ gestation and reach a final shape around 20 weeks’ gestation (9,10).
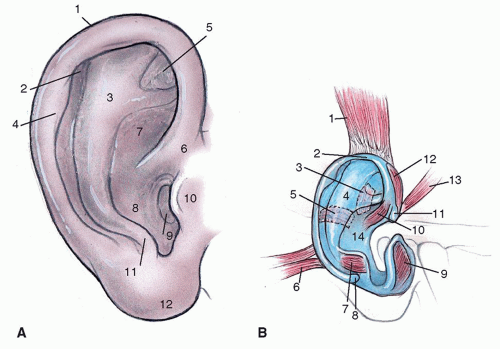 Figure 190.1 A: Normal external auricular anatomy. 1, Helix; 2, scaphoid fossa; 3, antihelix; 4, auricular (Darwin) tubercle; 5, triangular fossa; 6, crus helicis; 7, cymba concha; 8, cavum concha; 9, external auditory meatus; 10, tragus; 11, antitragus; 12, lobule. B: Normal external and internal auricular musculature. 1, Auricularis superior; 2, helix; 3, obliquus auriculae; 4, antihelix; 5, transversus auriculae; 6, auricularis posterior; 7, antitragicus; 8, cauda helicis; 9, tragicus; 10, helicis minor; 11, spina helicis; 12, helicis major; 13, auricularis anterior; 14, concha. |
The ear generally reaches 85% of its ultimate vertical height, 5 cm, by 3 years of age and is nearly full size, 6 cm, by 5 years of age. From this point on, the helix will grow relatively little, while the lobule will grow to a much greater degree, disproportionately lengthening with advancing age (9,11). In general, men have a slightly larger pinna and greater distance from the lateral orbital rim to helical root than do women; these distances are usually equal for each individual and on average measure 6 cm. Ear width, on the other hand, is usually just over half its height. Ear protrusion can be measured by either its distance from or angle to the scalp. The average distance from the helical rim to the scalp is 1.5 to 2 cm while the average auriculocephalic angle is 20 to 35 degrees (Fig. 190.3) (12,13).
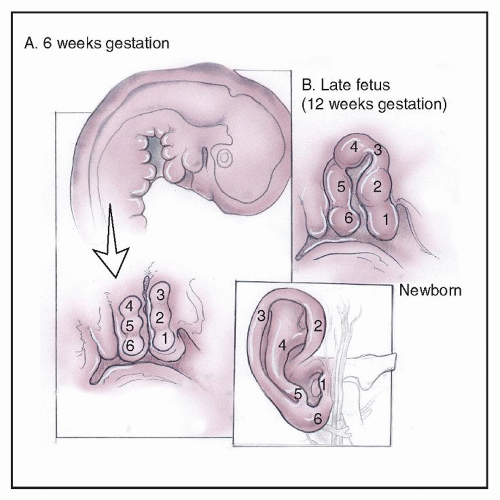 Figure 190.2 Normal ear development from the hillocks of His. |
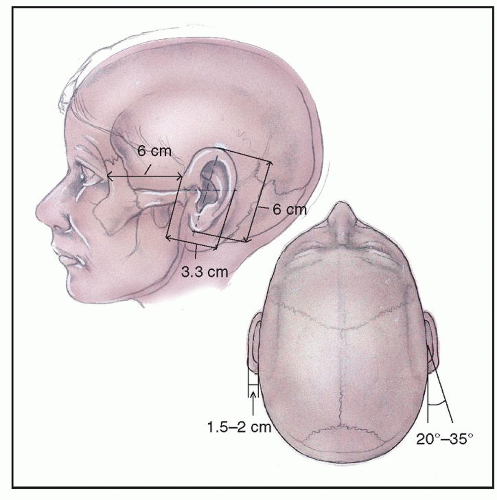 Figure 190.3 Normal ear dimensions. |
AURICULAR ANOMALIES
Etiology and Classification
Auricular anomalies occur in approximately 5% of the population, either in isolation or as part of a syndrome (14). Most auricular anomalies are sporadic, but some are hereditary. Their etiologies include genetic mutations, in utero insults from exogenous factors, compression from external forces, and abnormal intrinsic ear musculature. There is a wide range of degree to which these anomalies can occur, and there are a number of classification systems, based on extent of anomaly and extent of surgical intervention, that have been devised to group them. Many of the early classification systems were combined by Weerda in 1988, dividing anomalies into first-, second-, and thirddegree dysplasia (Table 190.1) (15). In 1997, Tan et al. proposed an even more simplified system that takes ear molding techniques into account and divides anomalies into two groups: deformational auricular anomalies and malformational auricular anomalies. Deformations result from external forces that cause abnormal architecture of tissue that is otherwise normal, while malformations result from abnormal tissue development that leads to abnormal architecture. Deformational auricular anomalies can be manually reduced to create a nearly normal appearance and can be treated early on with ear molding techniques or later with surgery. Malformational auricular anomalies, on the other hand, cannot be manually reduced to a normal appearance. These anomalies require surgery but can, in some cases, be partially treated with ear molding techniques if they also contain deformational components (16,17). In general, these classification systems are useful in clinical evaluation and determining the types of intervention that will be most helpful. However, it is important to keep in mind that auricular anomalies do not always fit cleanly within a single category and a number of treatment options should be considered in every case.
TABLE 190.1 AURICULAR DYSPLASIA CLASSIFICATION SYSTEM BY WEERDA | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Deformations
Stahl Ear
Stahl ear, alternatively known as Satyr ear, Spock ear, and Vulcan ear, is a first-degree or deformational auricular anomaly characterized by an abnormal transverse crus from the antihelix to the posterior superior helical rim and, often times, an absent superior crus (Fig. 190.4). It may be caused by external forces in utero or perhaps an abnormal course of the transversus auriculae, one of the intrinsic muscles of the ear (18). Stahl ear can be treated with molding techniques, suturing techniques, or excision of abnormal cartilage (19,20).
Cryptotia
Cryptotia, a term that means hidden or pocket ear, is a condition in which the superior helical cartilage is buried under the skin (Fig. 190.4). This deformity is thought to be caused by an abnormal attachment of the superior auricular muscle to the scapha rather than to the triangular fossa as well as a shortened transversus auriculae, effectively pulling the superior helix under the skin during development. This condition can be treated with molding or by releasing the superior helix from the scalp with skin grafting, advancing the resulting postauricular defect, performing a Z-plasty, or performing a trefoil flap, a flap consisting of three symmetric triangles based at the superior auricle that is used to cover the posterior cartilage upon release (21,22).
Prominent Ear
The prominent ear is a type of deformational auricular anomaly characterized by an absent antihelical fold and deep conchal bowl (Fig. 190.4). These deformities increase the auriculocephalic angle and the distance from the scalp to the helix. In addition, the prominent ear will often demonstrate a number of secondary findings, including a large helical root, excessive lobule projection, and inadequate helical curl. This condition has been associated with an abnormally distal insertion of the antitragicus muscle that extends along the anterior surface of the ear from the antitragus to the antihelix, pulling the helix laterally during development (23). Ear molding techniques may be successful early in life but, unlike with certain other ear deformities, often fail to adequately treat this condition if older than 3 months (16,24). This failure may be related to resistance created by the antitragicus muscle. In many cases, surgical intervention is required for definitive treatment.
Malformations
Constricted Ear
Constricted ears are characterized by partial absence of cartilage at the upper third of the helical rim and sometimes
the concha, resulting in a purse-string effect at the helix (Fig. 190.4). This type of malformation can be classified as either first- or second-degree dysplasia depending on its severity. Constricted ears will demonstrate a combination of helical lidding, protrusion, low position, and decreased size. This category is variably labeled as cup, lop, and cockleshell ear, among other names, in various sources. This malformation can be found in a number of inherited syndromes but is usually sporadic when isolated.
the concha, resulting in a purse-string effect at the helix (Fig. 190.4). This type of malformation can be classified as either first- or second-degree dysplasia depending on its severity. Constricted ears will demonstrate a combination of helical lidding, protrusion, low position, and decreased size. This category is variably labeled as cup, lop, and cockleshell ear, among other names, in various sources. This malformation can be found in a number of inherited syndromes but is usually sporadic when isolated.
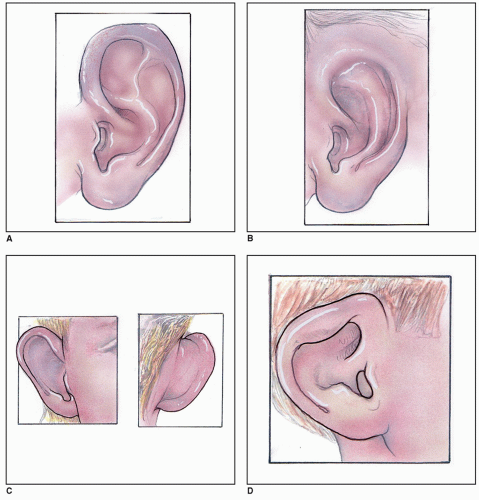 Figure 190.4 A: Stahl ear. B: Cryptotia. C: Prominent ear. D: Constricted ear. |
The findings in constricted ears can be divided into three groups based on severity and the treatment that is needed for correction. Mild constriction involves the helix only and can often be corrected with molding techniques as a neonate or later with an otoplasty technique similar to that used for prominent ears. Moderate constriction and severe constriction, however, are defined by hypoplasia of both the helix and scapha and require surgical intervention. Moderate constriction often requires a V-Y helical
root advancement as well as conchal or sometimes rib cartilage grafting (25). Severe constriction requires subtotal auricular reconstruction with rib cartilage grafting and postauricular skin recruitment (26,27).
root advancement as well as conchal or sometimes rib cartilage grafting (25). Severe constriction requires subtotal auricular reconstruction with rib cartilage grafting and postauricular skin recruitment (26,27).
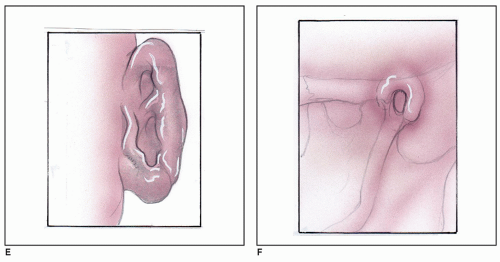 Figure 190.4 (Continued) E: Microtia. F: Anotia. |
Microtia
Microtia is hypoplasia of a majority of the pinna, while anotia is the complete absence of the pinna (Fig. 190.4). These malformations may or may not spare the external auditory canal and are types of third-degree dysplasia. Total auricular reconstruction for microtia and anotia is not addressed in this chapter.
Psychosocial Issues
There have been a handful of studies and anecdotal observations regarding the psychosocial impact of various facial anomalies. The majority of these studies, however, concern children with significant craniofacial malformations. One study that did examine children with isolated ear anomalies noted a 40% incidence of ear anomaly in children who were residents of the Mental Health Center of Norfolk, the majority of which were noted to have had adjustment reactions in childhood or adolescence (12). It is important to note, however, that no evidence of causation could be determined. A more recent study by Sheerin et al. compares children with prominent ears to children with facial port-wine stains and suggests that self-esteem, social, and attention problems may be even more severe in the group with prominent ears. Although the groups were small, the study’s authors believe this difference could in part be due to decreased familial support and recognition of deformity in those with prominent ears, who may be thought of as having an exaggeration of the normal rather than a true deformity. Regardless of the reason for this difference, this study suggests that children who are bothered by their ears are much more likely to have psychosocial problems (28). Further studies may help to determine if otoplasty can help to improve psychosocial adjustment in this population.
PATIENT SELECTION
Initial Evaluation
There are several steps that should be performed when evaluating a patient with auricular dysplasia. The patient’s unique ear anatomy should be analyzed, goals and expectations should be addressed, and treatment options should be considered that best meet the agreed-upon goals.
First, the ears should be photographed with fullface and close-up frontal, oblique, lateral, and posterior views. After physical exam, these images are an important adjunct for evaluating the anatomic causes of deformity as well as any differences on one side compared to the other. These images can be viewed with the patient to facilitate a discussion about goals and expectations for treatment, realistic outcomes, and the appropriate techniques that could be employed to achieve this result. In addition, measurements of ear height, width, and distance from the scalp as well as the auriculocephalic angle are useful. Together, these images and measurements can be used to objectively document postoperative and long-term follow-up changes (29).
Nonsurgical Treatment
If a deformational auricular anomaly is identified in a neonate or, according to some, select older individuals, molding techniques should be considered. These techniques usually involve placing a bendable splint along the helical rim, antihelix, and conchal bowl and taping it in place to hold the ear in an appropriate position for 2 to 12 weeks. Molding is able to correct up to 90% of deformational auricular anomalies if started within the first week of life (30,31). Most authors only advocate molding for neonates, but there have been some reports of successful treatment of older children (32). In general, after 3 weeks of age, molding is less successful. Yotsuyanagi noted that improvement declines from 80% if molding is started at 1 to 3 months of age, to 33% if molding is started after 9 years of age. In general, molding failures in this study were most common with moderately and severely constricted ears as well as prominent ears (24,33).
In 2011, Leclere et al. reported a series of 17 patients with prominent ears and an average age of 34.5 years who underwent laser-assisted cartilage reshaping, a new technique in which the ear is treated with an erbium/glass laser to reshape the cartilage without any anesthesia and molded into the desired shape with a silicone splint. The splint is then worn at all times for 2 weeks and then at night only for 4 weeks. At a 30-month follow-up appointment, two patients had incomplete shape correction, which was thought to be related to incorrect splint design and contact dermatitis, and five patients had slight ear asymmetry. Overall, 10 of 17 patients obtained the desired result (34). Although only small series have been published about this technique, it may become a preferred method of treatment in the future.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


