Cancer of the oropharynx is relatively uncommon, accounting for fewer than 1% of all new cancers. Cancer data reported combine oral cavity sites with oropharyngeal sites. It has been estimated that over 39,000 cases of oral cavity and pharyngeal cancer will be diagnosed in the United States in 2010 (
1). Approximately one-third of these will be expected to arise in the oropharynx. Its peak incidence is between the sixth and seventh decades of life; however, cases in the fifth and fourth decades of life are not uncommon. The disease has a distinct male predominance, but recent data show an increased incidence among women. Squamous cell carcinoma (SCC) and its variants account for more than 90% of malignant oropharyngeal lesions. Historically, the most important etiologic factor was the exposure to tobacco and alcohol; however, the majority of cases seen today are HPV associated (
2). Treatment of this disease is complex, and a team including a head and neck surgeon, reconstructive surgeon, radiation oncologist, medical oncologist, prosthodontist, and speech and language pathologist offers the patient the best opportunity for disease control with management of treatment-related toxicities.
ANATOMY
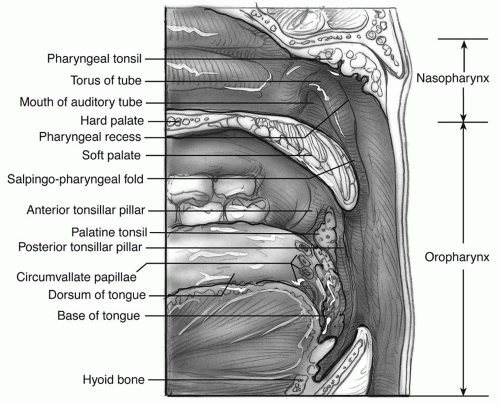
The oropharynx is the midportion of the pharynx that connects the nasopharynx superiorly to the oral cavity anteriorly and to the hypopharynx inferiorly. It extends from an imaginary horizontal plane through the hard palate to another through the hyoid bone (
Fig. 121.1). As it opens into the oral cavity, it is bounded by the circumvallate papillae, anterior tonsillar pillars, and the junction of the hard and soft palates. The posterior limit of the oropharynx is the posterior pharyngeal wall, which lies anterior to the prevertebral fascia. The lateral boundary includes the tonsillar fossae and pillars and the lateral pharyngeal walls. The superior limit is contiguous with the inferior boundary of the nasopharynx. Clinically, the oropharynx is divided into four subsites: base of tongue, soft palate, the palatine tonsillar fossa and pillars, and pharyngeal walls.
The pharyngeal walls are made of multiple layers, which include from surface to deep the mucosa, submucosa, pharyngobasilar fascia, constrictor muscles (superior and upper fibers of middle), and buccopharyngeal fascia. The superficial anatomy of the lateral walls includes the anterior tonsillar pillars (palatoglossus muscle); the palatine tonsillar tissue, which lies in the tonsillar fossae; posterior tonsillar pillars (palatopharyngeal muscle); and a small portion of lateral pharyngeal walls. The palatine tonsils, when present, often have an irregular surface filled with crypts, which are blind tubules of epithelium that invaginate deep within the lymphoid tissue of the tonsil.
The soft palate is a fibromuscular structure that projects posteriorly and downward into the oropharynx. It is composed of the palatine aponeurosis, which forms the skeleton and includes the tensor veli palatini, levator veli palatini, uvular, palatoglossus, and palatopharyngeal muscles.
The base of the tongue is the anterior wall of the oropharynx and extends from the circumvallate papillae back to the pharyngoepiglottic ligament and glossoepiglottic folds. The lingual tonsils lie superficial and lateral on either side and cause its mucosal surfaces to be irregular. The paired valleculae mark the transition of the base of the tongue into the epiglottis. This relationship explains why the submucosal spread of tumor from the base of the tongue may involve the supraglottic larynx or, conversely, laryngeal tumors may grow into the base of the tongue.
Most of the oropharynx is supplied with sensory and motor innervation through the glossopharyngeal (cranial nerve IX) and vagus (cranial nerve X) nerves. The hypoglossal nerve (cranial nerve XII) supplies motor innervation to the base of the tongue. The motor and most of the sensory innervation of the soft palate comes from the trigeminal nerve.
The oropharynx is abundantly supplied with blood from most branches of the external carotid artery, particularly the ascending pharyngeal. The lymphatic drainage is primarily to levels II and III, with midline structures such as the tongue base, soft palate, and posterior pharyngeal wall draining to both sides of the neck. The posterior pharyngeal wall, soft palate, and tonsillar region also drain to the retropharyngeal nodes, which in turn drain to the upper level II nodes.
The oropharynx is surrounded on three sides by potential fascial spaces. The retropharyngeal space is an area of loose connective tissue lying behind the pharynx between the buccopharyngeal fascia of the pharynx and the alar layer of the prevertebral fascia. The retropharyngeal space extends from the skull base to the superior mediastinum and communicates with the parapharyngeal space laterally. The parapharyngeal space is defined by fascial planes extending from the skull base to the greater cornu of the hyoid bone and lying lateral to the pharyngeal walls. It has the shape of an inverted pyramid, and its boundaries include the skull superiorly, pterygomandibular raphe anteriorly, prevertebral fascia posteriorly, and the pharynx medially. The lateral boundary is the most complex and is formed by the fascia overlying the medial pterygoid muscle, a portion of the mandible, deep lobe of the parotid, and the posterior belly of the digastric muscle. This fascia extends superiorly, incorporating the stylomandibular ligament, and fuses with the strong interpterygoid fascia to attach to the skull base in a line passing medial to the foramen ovale and spinosum. It also separates the parapharyngeal space from the infratemporal fossa and masticator space and places the trigeminal nerve within the latter (
3). The parapharyngeal space can be further divided by a layer of fascia running from the tensor veli palatini muscle to the styloid and its related structures into two compartments. The prestyloid compartment contains fat, variable portions of the deep lobe of the parotid, and a small branch of the trigeminal nerve to the tensor veli palatini. The poststyloid compartment contains the carotid artery, jugular vein, cranial nerves IX to XII, sympathetic chain, and lymph nodes.
There are multiple aspects of oropharyngeal anatomy that are clinically important. The irregular surfaces of the tongue base and the tonsils make it difficult to identify small tumors. The vagus and glossopharyngeal nerves have tympanic and auricular branches (Jacobson and Arnold nerves), which cause the referred otalgia associated with tumors of this area. The retropharyngeal and parapharyngeal spaces also serve as potential routes for cancer spread. Surgical margins may be difficult to achieve in some patients because oropharyngeal structures lack natural boundaries. Tumors that involve the palate or tonsillar pillar may invade or encase bone of the mandible or maxilla. Involvement of the muscles of mastication results in pain and trismus. Base of tongue tumors may spread in all directions to involve larynx, palatine tonsil, or oral tongue.
PHYSIOLOGY
The oropharynx is essential for normal speech production, respiration, and deglutition. These highly coordinated functions require intact sensory and motor input and intact structures. A detailed understanding of these coordinated events is crucial. All treatment modalities may result in dysfunction.
Deglutition is the most complex of these functions and can be divided into four phases: (a) oral preparatory, (b)
oral, (c) pharyngeal, and (d) esophageal. The oropharynx plays an important role in the first three phases. The soft palate is pulled forward while the tongue base is slightly elevated during both oral phases to prevent food from spilling prematurely into the pharynx. The food bolus at the end of the oral phase is propelled between the tongue and palate, past the tongue base and faucial arches, triggering the pharyngeal phase. This phase culminates with the propulsion of the food bolus into the esophagus through the following events: (a) velopharyngeal closure, (b) elevation and closure of the larynx, (c) contraction of the pharyngeal muscles and retraction of the tongue base, and (d) opening of the cricopharyngeal region. The major driving force of the bolus through the pharyngeal phase is the pressure developed by the tongue base; pharyngeal contraction and peristalsis serve mostly to clear the residual material present at the end (
4).
Extirpative surgery of the oropharynx may result in poor speech production, dysphagia, and aspiration. This may be a result of velopharyngeal incompetence, pharyngeal stenosis, inappropriate functioning of the tongue base tethering or volume reduction, decreased pharyngeal contraction, sensory denervation, and delayed triggering of the pharyngeal swallow because of decreased sensation. Avoidance of these undesirable sequelae may be mitigated with proper patient selection for surgery, appropriate reconstruction, and vigorous rehabilitation. Use of tissue sparing such as intensity-modulated radiation therapy (IMRT) radiation techniques and less toxic regimens may be appropriate in some cases. Evaluation of speech and swallowing should occur before, during, and after treatment to allow for the best outcomes and quality of life (
5).
ETIOLOGY
SCC of the head and neck is known to arise from the accumulation of multiple genetic alterations to genes important to the regulation of cellular growth and death. These alterations, which may be inherited but are more often acquired from exposure to environmental agents, provide the cell with a selective growth advantage. The cells then undergo further selection, which eventually results in a clone that overcomes the normal growth controls and host defenses to establish the tumor (
6).
Multiple environmental factors are associated with SCC of the oropharynx. Historically the most important was exposure to tobacco and alcohol. Heavy tobacco users have a 5- to 25-fold higher risk of developing head and neck cancer than nonsmokers (
7). The effect of these agents is dose related, and concurrent exposure is synergistic, resulting in a risk that is greater than the sums of the risks of either one alone (
8). The relative risk of developing cancer increases from 2.7 in those who smoke up to 10 cigarettes per day to 9 in those who smoke 1 pack per day. The relative risk also increases with an increase in alcohol consumption; the relative risk rises to 8.8 in those who consume 30 or more drinks per week compared to 1.2 in those who consume 1 to 4 drinks per week. The combination of smoking and drinking has a greater than additive effect as mentioned earlier; a person who has greater than a 40-pack-year history of smoking who consumes 5 alcoholic drinks per day has a relative risk of 40 (
9,
10).
Viruses have been shown to be a probable etiologic agent in development of SCC. The most extensively studied virus is the human papillomavirus (HPV) (
11). In a study by Kerimer et al., a systematic review of 5,046 head and neck SCC specimens from 60 studies worldwide was performed to determine the worldwide prevalence and types of HPV in head and neck cancer (
11). The overall prevalence of HPV was 25.9%: 35.6% in oropharyngeal SCC, 23.5% in oral cavity SCC, and 24.0% in laryngeal SCC. HPV 16 was the most common type detected: It accounted for 30.9% of oropharyngeal SCC, 16% of oral cavity SCC, and 16.6% of laryngeal SCC. HPV-positive tumors are more likely to originate in the oropharynx, to be poorly differentiated, have basaloid features, and present with a lower T stage than HPV-negative tumors. Prognosis and response to treatment are strongly associated with HPV status, and those who are positive appear to be more responsive to treatment and thus have a survival advantage (
12).
Individuals with HPV-positive tumors have different risk factors than those who are HPV negative. HPVpositive SCC’s were independently associated with sexual behavior and marijuana use but not with tobacco or alcohol use or poor oral hygiene. On the other hand, those tumors that were HPV negative were associated with heavy alcohol and tobacco use and poor oral hygiene, but not sexual behavior or marijuana use (
13). D’Souza et al. (
14) found that oral HPV infection is strongly associated with oropharyngeal SCC among those with or without established risk factors of alcohol and tobacco use. In addition, Mork et al. (
15) found a 14-fold increase in risk of developing oropharyngeal SCC in those who are seropositive for PGY 16. Oropharyngeal tumors should be tested for HPV 16 status.
Dietary factors such as vitamin deficiency (Vitamin A, iron deficiency of Plummer-Vinson syndrome), poor nutrition, poor oral hygiene, syphilis, occupational exposure, and previous irradiation also have been implicated as etiologic agents; however, evidence is limited overshadowed by the evidence supporting the carcinogenic effects of tobacco and alcohol.
Immunosuppression due to heredity, transplantation, or human immunodeficiency virus (
16,
17) may accelerate the development of SCC, lymphoma, and other tumors of the oropharynx by impairing normal immune surveillance mechanisms.
HISTOPATHOLOGY
The oropharynx consists of different types of epithelium pending on the subsite. The oropharyngeal epithelium arises from stratified squamous epithelium and transitions
where the soft palate contacts the posterior pharyngeal wall (Passavant ridge) into ciliated respiratory epithelium of the nasopharynx.
Minor salivary glands can be found in the soft palate, tonsillar pillars, and lingual tonsils, and therefore, tumors of minor salivary gland origin can be found in these places. Lymphoepithelium can be found in the subsites that form Waldeyer ring (nasopharynx, palliative tonsils, and tongue base).
Premalignant lesions occur in the oropharynx; however, they are rarely recognized. Lesions are seen most commonly on the soft palate and anterior tonsillar pillars and include leukoplakia (white plaque lesion), erythroplakia (sharply demarcated red lesion), and lichen planus (white, lacy lesion). Diagnosis requires biopsy.
SCC (keratinizing and nonkeratinizing) and its variants account for more than 90% of malignant oropharyngeal lesions. The spindle cell variant is clinically and biologically similar to SCC, whereas others behave differently. Basaloid appearance of SCC may be an indication of HPVpositive status (
12).
Verrucous carcinoma is a fungating, slow-growing tumor with well-differentiated keratinizing epithelium and rare cellular atypia or mitosis on histology. These tumors have “pushing” margins. They rarely metastasize and are considered a low-grade malignancy. Lymphoepitheliomas arise from Waldeyer ring. This tumor is nonkeratinizing and is similar in behavior to the undifferentiated type of nasopharyngeal carcinoma. These lesions usually occur in the tonsillar region of young adults that do not have typical risk factors. Lymphoma may occur in Waldeyer ring (usually non-Hodgkin lymphoma). Minor salivary gland tumors, mucosal melanomas, and sarcomas are other malignant lesions found in the oropharynx.
Minor salivary gland malignancies are relatively rare. The most common types include adenoid cystic carcinoma, mucoepidermoid carcinoma, and adenosquamous carcinoma. These tumors are treated with primary surgical excision and postoperative radiotherapy depending on high-risk features (perineural invasion, close or positive margins, nodal metastases, high-grade disease).
Some benign lesions, such as minor salivary gland tumors, pseudoepitheliomatous hyperplasia, necrotizing sialometaplasias, Crohn disease, papillomas, pyogenic granulomas, and median rhomboid glossitis, may clinically mimic malignant lesions. Biopsy is usually required to distinguish among these entities.
NATURAL HISTORY
Prolonged exposure of the upper aerodigestive surfaces to carcinogens results in molecular changes throughout the mucosa. With time, certain areas may undergo further change, giving rise to premalignant and malignant lesions. This concept of “field cancerization” or “condemned mucosa” applies to all mucosal head and neck cancers and results in the high rates of second primaries in patients with oropharyngeal cancer (
18) (
Table 121.1).
SCC usually starts on the surface. Invasion of vessels and thick fascia such as the prevertebral fascia or periosteum is uncommon until late stages, but perineural invasion may occur at any time. Bone involvement is also rare, occurring in only 17% of the lesions (
19). Invasion into the parapharyngeal and retropharyngeal spaces allows easy spread to the skull base and neck with possible involvement of the internal carotid artery, cranial nerves IX through XII, and the sympathetic chain. Invasion of the masticator and infratemporal spaces results in trismus.
Lymphatic metastases at presentation are common because the oropharynx is richly supplied with lymphatics and the tumors are generally advanced (
20) (
Table 121.1). Tumors of the oropharynx may be remarkably asymptomatic. Symptoms of sore throat, otalgia, and dysphagia are commonly misinterpreted or overlooked. For many patients, the first acknowledged observation is the presence of a cervical metastasis.
Oropharyngeal cancer tends to metastasize early. The first echelon nodes are level II, III, or retropharyngeal. Metastasis may be altered by obstruction of the lymphatic channels caused by inflammation, previous surgery, radiation, or large metastatic deposits. Oropharyngeal cancers have a tendency to metastasize to both necks, especially if
the lesion is midline. The rate of occult neck metastases in the clinically negative neck is estimated at greater than 20% for all lesions larger than T1.
Distant metastases are rare at presentation, occurring in 2% to 5% of patients, but with control of the disease above the clavicles, the incidence of overt distant metastasis increases (
18,
21) (
Table 121.1). The most common sites affected by distant metastases are lung, liver, and bones.
 DIAGNOSIS OROPHARYNGEAL CANCER
DIAGNOSIS OROPHARYNGEAL CANCER


