In this chapter, we provide the reader with a cursory overview of orbital pathology as it may relate to the practicing Otolaryngologist. This chapter outlines the most common categories of orbital tumors and other common orbital pathologic processes. We discuss various classifications of the pathologies presented, as well as the most common associated signs/symptoms, radiographic findings, and recommended workup and treatment for these lesions. We only briefly discuss secondary lesions affecting the orbit, as these are covered in greater depth in the rhinology and skull base sections of this text. We also specifically discuss the surgical approaches that can be utilized in addressing these pathologic processes.
Classification
Orbital tumors are rare, yet constitute a wide range of lesions. They are often classified based on their origin. Primary orbital tumors originate within the bony orbit, while secondary tumors extend into the orbit from the paranasal sinuses, skin, and/or intracranial compartment. Primary tumors can further be classified based on their anatomic location, with intraconal lesions being confined within the extraocular muscle cone, and extraconal lesions occurring outside of these muscles. Lastly, metastatic orbital tumors originate from distant tissues and spread to the orbit through lymphovascular and/or hematogenous spread.
Primary orbital tumors can originate from the tissues that are present within the orbit, including vascular, lymphoid, nervous, and mesenchymal structures. Lacrimal gland tumors of epithelial and/or lymphoid origin can also present as orbital tumors. In a 40-year study of orbital tumors at the Mayo Clinic, Henderson (
1) found that the five most common primary tumors of the orbit were hemangioma, non-Hodgkin lymphoma, inflammatory tumors, meningioma, and optic nerve glioma. Similarly, in a study of 1,264 patients from the Wills Eye Institute, Shields et al. (
2) showed again that there is a very wide range of pathologic types of orbital tumors and that the five most common categories of orbital lesions in their series were vasculogenic (17%), inflammatory (11%), lymphoid/leukemic (10%), lacrimal gland (9%), and optic nerve or meningeal lesions (8%).
In another large series out of MD Anderson, Shinder et al. (
3) found that the five most common lesions were lymphoproliferative (25%), lacrimal (10%), inflammatory (8%), vascular (7%), and mesenchymal (7%). In a metaanalysis of five large series, Wilson and Grossniklaus (
4) evaluated a total of 4,563 orbital lesions and found that the most common primary orbital tumors were meningiomas, cavernous hemangiomas, and lymphomas. While some series have shown that secondary orbital tumors can account for 33% to 45% of all orbital neoplasms (
1), more recent series have found that only 11% to 26% of all orbital tumors are secondary in nature (
2,
3). This could be due to improved recognition and treatment of the primary processes that most often cause secondary lesions of the orbit, mainly paranasal sinus mucoceles, squamous cell carcinomas (SCCs) of the paranasal sinuses, meningiomas of the cranial base, vascular malformations, and basal cell carcinomas (BCCs) of the skin. Metastatic disease to the orbit has been found to account for anywhere between 2% and 10% of orbital tumors (
1,
2,
3). (See
Tables 130.1 and
130.2 for the most common orbital tumor percentages and the most common metastatic lesions.)
Interestingly, Shields et al. found that malignant lesions comprised 36% of the tumors in their series, while Shinder et al. found that 63% of their tumors were malignant (
2,
3). Obviously, the type of high volume referral centers where series such as these are put together largely determines the types and distribution of lesions seen, treated, and reported. Not surprisingly, the rates of malignant lesions,
as a percentage of all orbital tumors, increase significantly as age increases. Most pediatric tumors are benign, with most series reporting between 10% and 30% of all pediatric orbital tumors being malignant (
1,
2). However, some cancer centers treat a larger proportion of pediatric malignant orbital tumors, with the MD Anderson group reporting 68% of their pediatric tumors being malignant (
3).
Presentation
The volume of the orbit is roughly 30 mL, and therefore, mass occupying lesions have scant room for expansion before signs and symptoms arise. Proptosis is the cardinal clinical sign of an orbital space-occupying lesion. Direction and laterality of the proptosis are important factors that aid in the identification of the location, origin, and ultimate diagnosis of the lesion. Axial proptosis often occurs with lesions that exist within the intraconal space, while nonaxial proptosis tends to occur in tumors occupying an extraconal location. The timing of the proptosis also can help differentiate various processes, with acute proptosis developing over hours to days favoring inflammatory and infectious processes. Malignant tumors tend to present in a subacute time frame, while benign tumors tend to have a more indolent progression of symptoms. Age of onset can also help narrow the differential in consideration.
Diplopia and ocular motility disturbances are also common findings in patients with orbital tumors. Lesions may cause displacement of the globe with resultant diplopia. Similarly, infiltrative processes may affect the extraocular muscles and associated nerves, causing gaze restriction and diplopia. Deterioration of a patient’s visual acuity, including the rate and extent, is also of importance when distinguishing between various etiologies. For example, optic nerve gliomas or meningiomas may cause significant visual acuity changes, while secondary processes affecting the nerve often cause mild symptoms related to compressive effects. Orbital pain is most often a symptom of inflammatory and/or infectious processes. However, aggressive malignant tumors and metastatic lesions can also present in this manner. Slower growing lesions more often cause a sensation of pressure rather than pain. Pupillary changes can be found when tumors invade or compress the sympathetic or parasympathetic fibers supplying the iris dilator and
pupillary sphincter. Finally, while not part of the practicing otolaryngologist’s clinical exam, fundus changes within the globe are common ophthalmologic exam findings and may include optic atrophy or edema, optociliary shunt vessels, retinal venous dilation, and choroidal folds (
5).
Anatomy of the Orbit
Detailed knowledge of the anatomy of the orbit and periorbital structures is critical in developing effective surgical technique and minimizing surgical complications while operating in the tight orbital space. The following is a brief overview of orbital and eyelid anatomy.
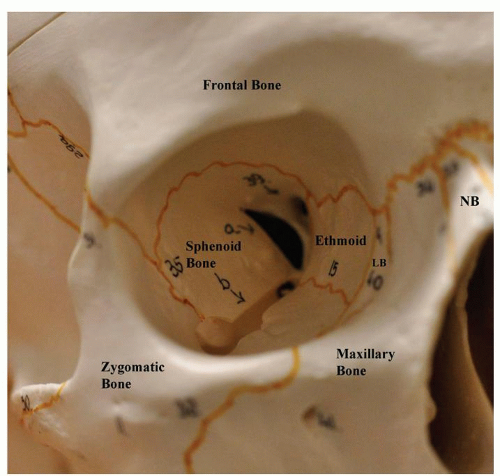
The bony orbit (
Fig. 130.1) is composed of the frontal, zygomatic, sphenoid, maxilla, lacrimal, palatine, and ethmoid bones. The adult orbit has a volume of approximately 30 mL and measures 35 mm in maximal height, 40 mm in width, and 45 mm in medial wall length. The orbital walls lie adjacent to all four paranasal sinuses: the orbital apex is located just anterolateral to the sphenoid sinus, the medial lamina papyracea borders the ethmoid sinuses, the orbital floor is adjacent to the maxillary sinus, and the roof of the orbit often forms the floor of the frontal sinus. The orbit is also intimately associated with the skull base, as the orbital roof borders the anterior cranial fossa and the orbital apex borders the middle cranial fossa. The orbit communicates with the middle cranial fossa via the superior orbital fissure and optic canal. It is contiguous with the pterygopalatine and infratemporal fossae via the inferior orbital fissure (
6).
The majority of the nerves of the orbit pass through the sphenoid bone. The superior orbital fissure lies between the greater and lesser wings of the sphenoid bone, with the optic canal located in the lesser wing. The annulus of Zinn, a tendinous ring at the orbital apex from which the rectus muscles arise, encircles the optic canal and separates the superior orbital fissure into two compartments at the origin of the lateral rectus muscle. The superolateral portion transmits the lacrimal, frontal and trochlear nerves, as well as the superior ophthalmic vein and occasionally the orbital branch of the middle meningeal artery. The medial portion outside of the optic canal transmits the upper and lower divisions of the oculomotor nerve (CN III), the nasociliary branch of CN V, and the abducens nerve (CN VI).
The intraorbital optic nerve is approximately 30 mm in length and passes through the optic canal along with the ophthalmic artery and sympathetic nerve fibers. The dura mater surrounding the nerve is continuous with the periosteum of the optic canal. The extraocular muscles are responsible for the movement of the eye and eyelid. All four rectus muscles (superior, medial, inferior, and lateral recti) originate posteriorly in the annulus of Zinn. The superior oblique muscle arises outside of the annulus, just superomedial to the optic canal, and courses anteriorly to the cartilaginous trochlea prior to inserting on the globe. The levator muscle originates superior to the annulus on the lesser sphenoid wing. The inferior oblique arises in the anterior orbital floor just inferolateral to the lacrimal sac fossa and travels posterolaterally to insert onto the globe (
7).
Orbital fat lies posterior to the orbital septum as intraconal and extraconal fat. The fat pads of the eyelids are anterior extensions of the extraconal fat and lie anterior to the levator aponeurosis in the upper lid and capsulopalpebral fascia in the lower lid. In the upper lid, there is a medial and central fat pad; the lacrimal gland lies laterally and may be mistaken for a third fat pad. In the lower lid, there is a medial, central, and lateral fat pad.
The arterial supply of the orbit arises primarily from the internal carotid artery, which gives rise to the ophthalmic artery. The ophthalmic artery lies inferolateral to the optic nerve in the optic canal, and in the majority of patients, it passes over the nerve to reach the medial orbit. As it courses anteriorly through the orbit, it gives off several branches including those to the optic nerve and retina (central retinal artery, posterior ciliary arteries), extraocular muscles, and lacrimal gland. Anteriorly it forms anastomoses with the external carotid arterial system to provide a rich blood supply to the eyelids and face. Venous blood is drained primarily by the superior ophthalmic vein, which originates in the superomedial orbit and travels posterolaterally to enter the cavernous sinus via the superior orbital fissure.
The eyelids provide a barrier for the globe against desiccation and trauma and thus play an important role in the preservation of vision. Eyelid skin is the thinnest skin of the body and lacks subcutaneous fat. Beneath the skin lies the orbicularis oculi muscle, which is responsible for
voluntary and involuntary closure of the eyelids. The orbital septum separates the eyelid anatomy from the deeper orbital contents and originates from the periosteum along the orbital rim. The orbital fat pads mentioned earlier are located posterior to the orbital septum and anterior to the upper and lower lid retractors. The main retractor of the upper lid is the levator palpebrae, which becomes the levator aponeurosis after it passes through Whitnall suspensory ligament. The capsulopebral fascia and Lockwood ligament are the analogous retractor and suspensory ligament of the lower lid. The conjunctiva is a mucous membrane that constitutes the posterior-most layer of the eyelids. The canthal tendons, which help maintain the horizontal stability of the eyelids, are fibrous bands that originate from the bony orbital walls and fuse with the upper and lower tarsal plates; the medial canthal tendon arises from the anterior and posterior lacrimal crests medially and the lateral canthal tendon originates at the lateral orbital tubercle (
8).