- the subperiosteal (subperiorbital) surgical space, which is the potential space between the bone and the periorbita
- the extraconal surgical space (peripheral surgical space), which lies between the periorbita and the muscle cone with its fascia
- the sub-Tenon (episcleral) surgical space, which lies between the Tenon capsule and the globe
- the intraconal surgical space (central surgical space), which lies within the muscle cone
- the subarachnoid surgical space, which lies between the optic nerve and the nerve sheath
A single orbital lesion may involve more than 1 surgical space, and a combination of approaches may be necessary for pathologic processes affecting the orbit. The approaches to these spaces—superior, inferior, medial, and lateral—are discussed in the following sections. Incisions used to reach these surgical spaces are shown in Figure 7-2.
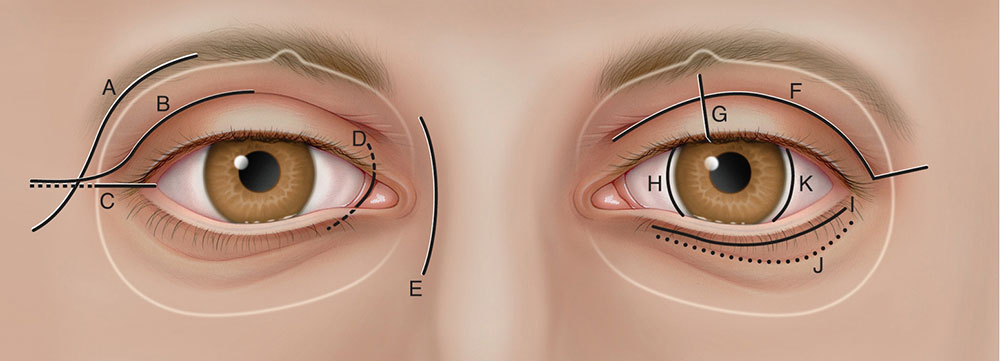
Figure 7-2 Sites of surgical entry into the orbit. A, Classic Stallard-Wright lateral orbitotomy. B, Eyelid crease lateral orbitotomy. C, Lateral canthotomy/cantholysis orbitotomy. D, Transcaruncular medial orbitotomy. E, Frontoethmoidal (Lynch) medial orbitotomy. F, Upper eyelid crease anterior orbitotomy. G, Vertical eyelid split superomedial orbitotomy. H, Medial bulbar conjunctival orbitotomy. I, Subciliary inferior orbitotomy. J, Transconjunctival inferior orbitotomy. K, Lateral bulbar conjunctival orbitotomy. (Illustration by Christine Gralapp after a drawing by Jennifer Clemens.)
More orbital lesions are found in the superoanterior part of the orbit than in any other location. Lesions in this area can usually be reached through a transcutaneous incision. With this approach, the surgeon must take care to avoid damaging the levator muscle, superior oblique muscle, trochlea, lacrimal gland, and sensory nerves and vessels entering or exiting the orbit along the superior orbital rim.
Transcutaneous incisions
For procedures in the superior subperiosteal space, an incision through the upper eyelid crease offers good access to the superior orbital rim and periosteum, with a well-hidden scar (Fig 7-3). Although this incision requires additional soft tissue dissection, the cosmetic result is better with an eyelid crease incision than with an incision directly over the superior orbital rim. After making an upper eyelid crease incision, the surgeon obtains access to the superior orbital rim by dissecting superiorly in the postorbicularis fascial plane anterior to the orbital septum. After the rim is exposed, an incision is made in the arcus marginalis of the rim, and a periosteal elevator is then used to separate the periosteum from the frontal bone of the orbital roof. The periosteal dissection is facilitated by initially keeping the periorbita intact, which prevents orbital fat from obscuring the view during reflection of the periosteum.

Upper eyelid crease incisions may also be used for entry into the medial intraconal space, which requires exposure of the medial edge of the levator muscle and dissection through the intermuscular septum extending from the superior rectus to the medial rectus muscles. This approach may be used for exposure and biopsy of the optic nerve or for fenestration of the retrobulbar optic nerve sheath in cases of idiopathic intracranial hypertension.
The coronal approach to the superior orbit is most often used in conjunction with trauma or craniofacial surgery. This approach is also used for transcranial orbitotomies to expose extensive lesions of the superior and posterior orbit and sinuses that require bone removal for access. Although the coronal incision may be used to gain access for lateral orbitotomy, this incision requires extensive elevation of the temporalis muscle, which may result in postoperative temporalis atrophy. Alopecia may occur at the site of the coronal scalp incision.
Stewart WB, Levin PS, Toth BA. Orbital surgery. The technique of coronal scalp flap approach to the lateral orbitotomy. Arch Ophthalmol. 1988;106(12):1724–1726.
Transconjunctival incision
Incisions in the superior conjunctiva can be used to reach the superonasal, sub-Tenon, intraconal, or extraconal surgical spaces; but dissection must be performed medial to the levator muscle to prevent postoperative ptosis.
Vertical eyelid splitting
Vertical splitting of the upper eyelid at the junction of the medial and central thirds allows extended transconjunctival exposure for the removal of superomedial intraconal tumors. The surgeon incises the eyelid and levator aponeurosis vertically to expose the superomedial intraconal space. Realignment of the tarsal plate and aponeurosis with vertical closure prevents postoperative ptosis and eyelid retraction.
Kersten RC, Kulwin DR. Vertical lid split orbitotomy revisited. Ophthal Plast Reconstr Surg. 1999;15(6):425–428.
The inferior approach is suitable for masses that are visible or palpable in the inferior conjunctival fornix of the lower eyelid, as well as for deeper inferior extraconal orbital masses. The surgeon can also gain access to intraconal lesions by dissecting between the inferior rectus and lateral rectus muscles. The inferior oblique muscle inserts over the macula and may be identified and retracted while intraconal lesions are accessed. This route is commonly used to approach the orbital floor for fracture repair or decompression.
Transcutaneous incisions
Visible scarring can be minimized by the use of an infraciliary blepharoplasty incision (2.5–4.0 mm below the margin) in the lower eyelid skin, followed by inferior dissection beneath the orbicularis oculi muscle to expose the inferior orbital septum and inferior orbital rim. An incision in the lower eyelid crease or directly over the inferior orbital rim can provide similar exposure, but it leaves a slightly more obvious scar. Once the skin–muscle flap is created, the surgeon can open the septum to expose the extraconal surgical space. Alternatively, for access to the inferior subperiosteal space the periosteum is incised and elevated at the arcus marginalis to expose the orbital floor. Fractures of the orbital floor are reached by the subperiosteal route.
Transconjunctival incisions
The transconjunctival approach (Fig 7-4) has largely replaced the transcutaneous route for exposure of tumors in the inferior orbit and for management of fractures of the orbital floor and medial wall. To reach the extraconal surgical space and the orbital floor, the surgeon may make an incision through the inferior conjunctiva and lower eyelid retractors. The optical cavity can be enlarged by adding a lateral canthotomy and cantholysis. The transconjunctival incision is made either just below the inferior tarsal border or in the conjunctival fornix. When using cutting cautery, the surgeon should take care not to cause thermal damage to the conjunctiva and tarsus. Opening the reflected periosteum and then retracting the muscles and intraconal fat provide access to not only the orbital floor but also the intraconal space.



