Fig. 5.1
MRI revealed a 42 × 25 × 25 mm lesion on the right side of oral tongue
The biopsy from the lesion in the tongue revealed well-differentiated squamous cell carcinoma (SCC). Right mandibulectomy and right selective neck dissection (levels I–IV) were performed with reconstruction using the major pectoral muscle. The pathology revealed moderately differentiated SCC. The tumor was 2.5 × 1.2 × 1.2 cm. There was diffuse perineural invasion (PNI). Surgical margins were negative, and 35 dissected lymph nodes were free of tumor.
The patient was staged as T2N0M0 oral tongue cancer .
Case 2
A 51-year-old male admitted to the hospital with an unhealing wound in the buccal mucosa of his left cheek.
His physical and endoscopic examination revealed a 1.5 × 1.5 cm lesion in the left buccal mucosa. There was no invasion in the nasopharynx, hard palate, oropharynx, or larynx. No lymph nodes were palpated.
The MRI detected an 18 × 11 × 15 mm lesion extending from the left buccal mucosa to left cheek fat pad (Fig. 5.2). It was located posterior to the maxilla and at the level of retromolar region. There were reactive lymph nodes, <1 cm in size in left level IA and bilateral level II.
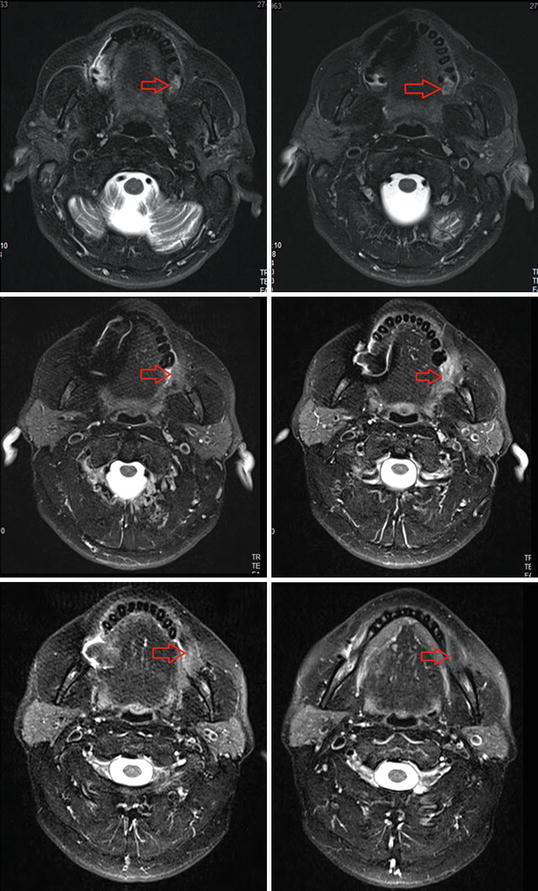
Fig. 5.2
MRI showing an 18 × 11 × 15 mm lesion extending from the left buccal mucosa to left cheek fat pad, located posterior to the maxilla, and at the level of retromolar region
The incisional biopsy from mucosal lesion revealed squamous cell carcinoma (SCC). He underwent wide local excision of the primary and left level I–V neck dissection. The pathologic evaluation was reported as moderately differentiated SCC. The tumor was 1.7 × 1.5 × 0.4 cm. Out of 37 dissected lymph nodes, 2 were metastatic and had extracapsular extension (ECE).
He was staged as T1N2bM0 buccal mucosa cancer .
2 Evidence-Based Treatment Approaches
Transoral or transcervical surgery is generally the first choice for early stage lesions [17]. More aggressive surgeries like mandibulectomy are performed when the lesion cannot be reached by these techniques or when there is bone invasion.
In early lesions of the lip, oral tongue, and floor of the mouth, radiotherapy (RT) and surgery are equivalent in terms of local control (LC) [18]. Historical series reported increased LC rates with the use of brachytherapy (BRT) either alone or in combination with external beam radiotherapy (EBRT) [19, 20]. Different authors reported LC rates that ranged from 70 to 96 % for T1 and T2 tumors [21–24].
Combined treatment modalities are preferred for locally advanced tumors [20, 25–27]. In case of mandibular invasion, definitive RT is contraindicated as LC results are poor with high risk of osteoradionecrosis . Postoperative RT is often preferred over preoperative RT to prevent a delay in surgery, to decrease the risk of wound complications, and to provide complete histologic evaluation. The disadvantage of postoperative RT is regional hypoxia which decreases the effectiveness of RT.
Postoperative RT is indicated in case of advanced T stage, suspected mandibular invasion, perineural invasion (PNI), close or positive surgical margins, multiple lymph node positivity, and/or extracapsular extension (ECE).
Neoadjuvant or adjuvant chemotherapy (CT), containing cis-platinum and 5-FU, was reported to have no impact on survival [28, 29]. However, adding CT concurrently to RT resulted in increased LC and overall survival (OS) rates [30].
Two prospective randomized trials investigated CRT after surgery in high-risk patients [31, 32]. The RTOG 9501 showed that in patients with positive surgical margins, two or more positive lymph nodes, or ECE, postoperative CRT increased LRC and disease-free survival (DFS) at the cost of increased toxicity but had no impact on OS. In EORTC 22931 study , in addition to these characteristics, stages III–IV, PNI, vascular tumor embolism, and level IV–V lymph node positivity were also evaluated as high-risk features. Besides the increase in LRC, and progression-free survival (PFS), OS was also superior in the CRT arm. In the report which combined these two trials, the only features that benefited from CRT were surgical margin positivity and ECE. Patients with two or more positive lymph nodes had no benefit from CRT, while patients with other high-risk features had a trend. In the 10-year update of RTOG 9501, the benefit in DFS and LC continued in patients with positive margins and ECE, and the long-term toxicity was reported to be similar to the RT alone group.
Buccal Mucosa
Primary surgery is preferred for small, superficial lesions. For deeper lesions (i.e. T2) or if there is commissure involvement, RT provides better results in terms of function and cosmesis, without any decline in cure rates. For more advanced lesions, radical surgery and adjuvant RT are indicated.
Oral Tongue
For small T1–2 lesions, RT yields better cosmetic and functional results and has similar LC rates compared to surgery. If floor of mouth is involved, partial glossectomy and partial mandibulectomy with radical neck dissection are performed. RT may be an alternative for patients who refuse surgery. Adjuvant RT is indicated in patients with locally advanced tumors, close or positive surgical margins, and PNI.
Floor of the Mouth
Surgery and RT yield comparable results in small, superficial tumors. In case of mandibular invasion, surgery should be preferred. For more advanced lesions (with invasion of bone or adjacent muscles), adjuvant RT is indicated.
Management of the Neck
Small, superficial (depth <2 mm) tumors with negative surgical margins do not require elective neck treatment (in case the patient is clinically node negative). In oral tongue and floor of the mouth tumors deeper than 2 mm, and in all tumors with perineural or perilymphatic invasion, the neck should be treated either with surgical dissection or by RT. Following neck dissection, if there is 1 positive lymph node without ECE, RT to the neck is not recommended [33]. If there are more than 1 positive lymph nodes (particularly at more than one nodal station), or ECE, the neck should be irradiated.
There are limited studies with IMRT on oral cavity tumors. Chao et al. from Washington University reported their initial results of 15 patients with oral cavity cancers whom they treated with IMRT [34]. Locoregional recurrence and distant metastasis were observed in 5 and 1 patients, respectively. There was no grade 3 or higher late toxicity. Similarly, Claus et al. treated 8 patients with oral cavity cancers via IMRT and observed no serious late toxicity, except for 1 patient who had mandibular osteoradionecrosis [35].
3 Target Volume Determination and Delineation Guidelines
Gross Tumor Volume (GTV)
GTV should include the gross tumor and involved lymph nodes detected by clinical examination, CT, MRI, PET/CT, and intraoperative findings, if operated. GTV is divided into two; GTVp defines the primary tumor, and GTVn defines the involved lymph nodes. In postoperative cases without residual tumor, GTV is not stated as it is assumed that no tumor or grossly involved lymph nodes are left.
Following structures should be evaluated carefully whether they are involved in oral tongue tumors:
Anteriorly:
Is the skin of face involved?
Laterally:
Is the skin of face involved?
Is the cortical bone of the mandible destructed?
Posteriorly:
Are the pterygoid plates involved?
Is there extension into the masticator space?
Is the carotid artery involved?
Superiorly:
Is the maxillary sinus intact?
Is the hard palate involved?
Is the skull base destructed?
Inferiorly:
Is the floor of mouth involved?
Is there extension to deep extrinsic muscles (genioglossus, hyoglossus, palatoglossus, and styloglossus)?
Clinical Target Volume (CTV)
Three CTVs are defined based on risk definitions.
CTV1 covers the primary tumor bed with a 0.5–2 cm margin given circumferentially around the GTV. CTV1 for the lymph nodes is the high-risk regions with a gross lymph node or, following lymph node dissection, levels with positive lymph nodes and extracapsular extension.
CTV2 covers the entire operative bed as it is the region of high risk for subclinical disease and potential routes of spread, along with the high-risk regions adjacent to it. Certain routes of spread are defined for particular locations. These are sublingual gland, midline genioglossus and geniohyoid muscles, periosteum, and mandible for floor of mouth cancers; floor of mouth, base of tongue, muscles of tongue, anterior tonsillar pillar, and mandible for oral tongue cancers; underlying muscles, skin, infratemporal fossa, parotid gland, and facial nerve for buccal mucosa cancers; and adjacent buccal mucosa, anterior tonsillar pillar, lower gum, maxilla, and mandible for retromolar trigone. CTV2 for the lymph nodes is ipsilateral submandibular, subdigastric, and midjugular nodal stations (upper neck). For tumors of the tip of the tongue, and tumors exceeding midline, upper neck should be contoured bilaterally. Periauricular and intraparotid lymph nodes are also delineated for the tumors of the upper lip. Oral cavity tumors with verrucous histology (which are often seen in the buccal mucosa) do not generally require elective neck irradiation as they rarely metastasize to lymph nodes.
CTV3 is the low-risk regions of subclinical disease. CTV3 for the lymph nodes include the contralateral upper neck and bilateral lower neck (lower jugular and supraclavicular). Ipsilateral posterior neck and retropharyngeal lymph nodes should also be delineated in the presence of jugular positive lymph nodes.
In patients who received neoadjuvant CT, CTV is defined depending on the prechemotherapy volumes.
Planning Target Volume (PTV)
A margin of 3–5 mm is added in all directions; however, it may be minimized to 1 mm in areas adjacent to critical structures.
Case Contouring
Delineation of target volumes for T2N0M0 oral tongue cancer (Case 1) is depicted in Fig. 5.3.
Fig. 5.3
(a, b) Delineation of target volumes for T2N0M0 oral tongue cancer (Case 1). (surgical bed, CTVp60Gy magenta; right neck, CTVn57Gy red; left neck, CTVn54Gy aqua) (BS brain stem, OC oral cavity, M mandible, P parotid gland, SC spinal cord, E epiglottis, V vallecula, Ps pyriform sinus, H hyoid bone, IJV internal jugular vein, L larynx, CA common carotid artery, Cr cricoid cartilage, TG thyroid gland, T trapezius muscle, E esophagus, TCV transverse cervical vessels)
Delineation of target volumes for T1N2bM0 buccal mucosa cancer (Case 2) is depicted in Figs. 5.4 and 5.5.
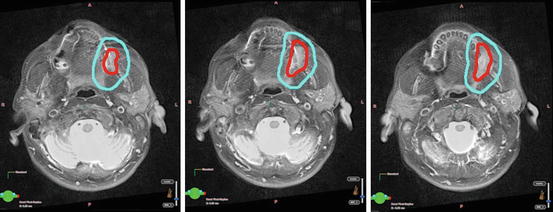
Fig. 5.4
(a–d) Delineation of target volumes for T1N2bM0 buccal mucosa cancer (Case 2) (surgical bed and right level I, CTVp60Gy red; left level I–V, CTVn57Gy yellow; right levels II–V, CTVn54Gy blue; right level Ib, CTVn60Gy blue; left level II, CTVn64Gy magenta) (M mandible, P parotid gland, SC spinal cord, H hyoid bone, IJV internal jugular vein, L larynx, CA common carotid artery, Cr cricoid cartilage, OC oral cavity, BS Brain stem, V valleculae, E Epiglottis, Ps pyriform sinus, TG thyroid gland, T trapezius muscle)
Fig. 5.5
Delineation of GTV and CTV for T1N2bM0 buccal mucosa cancer on fused MRI and BT simulation slices (Case 2)
4 Treatment Planning
Guidelines for target volume doses: Guidelines for target volume doses are summarized in Tables 5.1, 5.2, and 5.3.
Table 5.1
Guidelines for target volume doses of lip cancers< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


