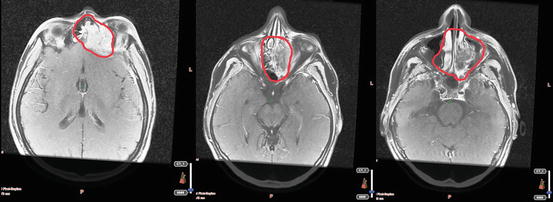
Fig. 4.1
A giant mass completely obliterating the superior 2/3 portion of the left nasal cavity and eroding superior nasal conchae seen on MRI
Biopsy from the nasal mucosa revealed undifferentiated carcinoma. Endoscopic resection was performed. The pathology revealed the same histology.
He was diagnosed with T4bN2bM0 maxillary sinus carcinoma .
2 Evidence-Based Treatment Approaches
Nasal Vestibule Tumors
Primary radiotherapy (RT) is preferred for small superficial tumors because of cosmetic concerns. However, surgery may also lead to high local control (LC) rates with excellent cosmetic results in selected cases. The size and location of the tumor guide us to choose the appropriate technique of RT. Brachytherapy (BRT) and external beam radiotherapy (EBRT) have similar cure rates reaching to 90 % for tumors up to 2 cm. For tumors larger than 2 cm, higher doses are needed to reach 80 % LC rates [7–11].
Large tumors with deep extensions require surgery in combination with neoadjuvant or adjuvant RT. Mazeron et al. evaluated 1,676 patients with nasal vestibule and skin of the nose cancers who were treated with BRT or EBRT. They reported 93 % overall LC rate. Tumors smaller than 2 cm and located externally (skin of the nose) have better LC rates (96 % for <2 cm vs. 81 % for >4 cm, and 94 % for skin of the nose vs. 75 % for the vestibule). However, LC rate with surgery only was no more than 90 % [12].
Nasal Cavity Tumors
Surgery and RT have similar results for small tumors in terms of cure. Daly et al. reported 91 % 5-year overall survival (OS) rates with either treatment modality [13]. Surgery may be preferred for posterior nasal septum tumors, whereas BRT is the treatment of choice for anterior and inferior septum tumors not larger than 1.5 cm. For lateral wall tumors, EBRT rather than BRT is preferred because of cosmetic concerns. In a study of 45 patients who were treated with solely RT, or RT combined with surgery, 5-year OS rate was 75 % [14]. In this study, Ang et al. reported that lateral wall and floor tumors had inferior prognosis compared to septum tumors (LC rates, 68 % vs. 86 %). For stages II–IVa, surgery should be performed with or without adjuvant RT.
Paranasal Sinus Tumors
Surgery and adjuvant RT are the treatment of choice for ethmoid sinus tumors. If cosmetic or functional result is an issue, RT alone or concurrent chemoradiotherapy (CRT) may be an option [15]. Choussy et al. reported tumor extension, lymph node involvement, and the presence of brain invasion as prognostic factors for ethmoid tumors. They found nearly half of the patients who received adjuvant RT after surgery had recurrences, 75 % of which were local [16]. Blanco et al. reported 5-year LC, DFS, and OS rates as 61, 35, and 29 %, respectively, in 106 patients with paranasal sinus cancers who received RT [17].
Surgery alone is efficient for early-stage maxillary sinus tumors. Adjuvant RT is indicated in patients with locally advanced disease. Combination therapy has better 5-year LC and OS rates than single treatment modalities, both ranging from 44 to 80 %. 5-year LC and OS rates with RT alone were reported as 39 and 40 %, respectively. Parsons et al. reported survival rates of 60, 70, 30, and 40 % for T1, T2, T3, and T4 lesions treated with surgery and RT, respectively [18]. In locally advanced tumors, solely RT results are dismal with 5-year survival rates of 10–15.
Intensity-modulated radiation therapy (IMRT) is accepted as the standard RT modality. A previous study from UCSF observed no difference in LC rates between IMRT and conventional RT [13]. 2- and 5-year LC rates were 62 and 58 %, respectively. However, the complication rate was significantly different with fewer complications in IMRT arm. In 2010, Dirix et al. reported 2-year LC and OS 76 and 89 %, respectively, with postoperative IMRT [19]. Madani et al. found 5-year LC and OS rates of 70.7 and 58.5 %, respectively, in 105 patients more than half of whom had ethmoid sinus tumors [20]. Also in 2012, Duprez et al. showed 5-year LC and OS as 59 and 52 %, respectively [21]. Claus et al. reported their IMRT experience in 62 patients with sinonasal cancers following R0 resection [22]. With PTV doses of 60–70 Gy, they found that none of the patients with cribriform plate invasion were locally controlled. However, 5-year actuarial LC rate was 84 % in patients without cribriform plate invasion.
Stereotactic body radiotherapy (SBRT) may also be an alternative option particularly to spare optic pathway structures. Ozyigit et al. published their experience on 27 patients with paranasal sinus or nasal cavity tumors whom they treated with CyberKnife® (Accuray, Sunnyvale, CA, USA) [23]. Six patients received RT for recurrence. Median dose was 31 Gy in median 5 fractions. They reported local relapse-free rates of 76 % for 21.4 months in median. Overall survival rates in 1 and 2 years were 95.2 and 77.1 %, respectively, with acceptable complication rates.
Chemotherapy
The role of chemotherapy (CT) in nasal cavity and paranasal cancers is limited. Neoadjuvant CT may be used for reducing the tumor size in order to assist surgery in terms of removal of the tumor with less morbidity and also to lend a hand to radiation oncologists in terms of decreasing normal tissue toxicity. In locally advanced tumors, the LC rates are better with concurrent CRT compared to neaodjuvant CT. For unresectable tumors, and medically inoperable patients, CRT is an option.
3 Target Volume Determination and Delineation Guidelines
Gross Tumor Volume (GTV)
GTV should include the gross tumor and involved lymph nodes detected by clinical and endoscopic examination, CT, MRI, PET/CT, and intraoperative findings, if operated. GTV is divided into two: GTVp defines the primary tumor, and GTVn defines the involved lymph nodes. In postoperative cases, GTV is not stated as it is assumed that the primary lesion or grossly involved lymph nodes are removed.
Following structures should be evaluated carefully whether they are involved in case of specific tumors:
Maxillary Sinus :
Anteriorly:
Is subcutaneous tissue involved?
Is there extension to the skin of cheek (leading to destruction in zygomatic arch)?
Laterally:
Is the pterygoid fossa involved?
Is there tumor extension to the sphenoid sinuses?
Medially:
Are the middle meatus and the nasal septum intact?
Posteriorly:
Is the posterior wall intact?
Are the pterygoid plates, pterygopalatine fossa and muscles involved?
Is there extension into the infratemporal fossa (through the cribriform plate)?
Are the clivus and C1 vertebra involved?
Does the tumor extend to the nasopharynx?
Superiorly:
Are the floor and medial wall of the orbit intact?
Is the ethmoid sinus involved?
Is the cribriform plate intact?
Inferiorly:
Is the hard palate involved?
Is there loosening of the first and second molar teeth (which points out invasion of maxilla)?
Ethmoid Sinus :
Anteriorly:
Is frontal sinus involved?
Is there extension to the anterior orbit?
Is the anterior cranial fossa intact?
Does the tumor extend to the maxillary sinus?
Is the palate involved?
Laterally:
Are the orbital medial wall and floor involved?
Does the tumor extend to the nasal cavity or the orbital rectus muscle?
Medially:
Is contralateral ethmoid sinus intact?
Posteriorly:
Is the sphenoid sinus involved?
Are the pterygoid plates intact?
Is there extension into the orbital apex, brain, middle cranial fossa, or clivus?
Is the cranial nerve (CN) I (olfactory) involved?
Is the dura involved?
Does the tumor extend to the nasopharynx?
Superiorly:
Is the cribriform plate intact?
Inferiorly:
Is the maxillary sinus involved?
Is there extension to the nasal cavity?
Does the tumor extend to the hard palate?
Clinical Target Volume (CTV)
Three CTVs are defined based on risk definitions. CTV1 covers the primary tumor bed with a 1–1.5 cm margin given circumferentially around the GTV.
CTV1 for the lymph nodes is the high-risk regions with a gross lymph node, or levels with positive lymph nodes and extracapsular extension (ECE) following lymph node dissection.
CTV2 covers the entire operative bed as it is the region of high risk for subclinical disease and potential routes of spread. If the ethmoid sinus or olfactory region is involved, the cribriform plate is also included. For paranasal sinus tumors, CTV2 includes all other sinuses, if explored during surgery. If orbital exenteration was performed because of orbital invasion, the bony orbit is also delineated. In case of craniofacial resection, the frontal graft should also be included. CTV2 for the lymph nodes should include ipsilateral submandibular and subdigastric lymph nodes for squamous cell and poorly or undifferentiated carcinomas. The lower neck should be contoured in case of invasion of the palate, nasopharynx, skin of the cheek or the anterior nose, or gingiva.
CTV3 is the low-risk regions for subclinical disease. In case of perineural invasion (PNI), a CTV3 is delineated in order to encompass the whole tract of the submandibular nerve to the skull base. In all adenoid cystic histologies, local nerve pathway to the skull base should be delineated, as these tumors are highly neurotrophic.
In patients who received neoadjuvant CT, CTV is defined depending on the prechemotherapy volumes.
Planning Target Volume (PTV)
A margin of 3–5 mm is added in all directions. However, it may be minimized to 1 mm or may even be omitted in areas adjacent to critical structures such as the optic nerves.
Case Contouring
Delineation of target volumes of T4bN2bM0 maxillary sinus carcinoma is shown in Figs. 4.2 and 4.3a–c.
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Fig. 4.2
Fused MR simulation CT images of GTV for T4bN2bM0 maxillary sinus cancer
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
