Optical Correction of Childhood Aphakia
Scott R. Lambert
Eric W. Hein
Introduction
The optical correction of childhood aphakia with an intraocular lens (IOL) has become the method of choice in the past decade. Despite the growing trend to follow adult patterns of aphakic correction, several underlying differences are foundational in caring for pediatric patients.1 First, a child’s eye is still growing and developing during the first few years of life. A myopic shift is often encountered, adding a new variable in calculating the power of the lens implant. Second, young children have immature visual systems making them vulnerable to amblyopia if visual input is defocused or unequal between the two eyes. Third, actuarial data would suggest that an IOL will have a longer “lifespan” in the eye of a child than in an adult. Given the cumulative incidence of many complications, certain risks that are tolerable in adults are unacceptable in children. Last, a child’s eye tends to manifest a more exuberant postoperative inflammatory response, necessitating certain modifications in the surgical implantation technique.2
Anatomy
During infancy and early childhood, the refractive elements of the eye undergo radical changes. At birth, the cornea has an average power of 52 D. By 18 months, the cornea has flattened significantly. The power decreases to 43.5 diopters (D) on average, where it essentially stabilizes into adulthood.3,4 In addition, the power of the crystalline lens progressively diminishes until age 6.5 The most important structural modification in a child’s eye is axial elongation. At birth, the mean axial length is 17 mm.6,7 The eye then undergoes a triphasic pattern of growth. The first phase occurs in the first 2 years of life as the eye lengthens 4.4 mm.4 The second phase, ages 2 through 6, brings an additional 1.5 mm. The final phase lasts through adulthood and adds another 1 mm on average, but this amount can be greater in eyes with a genetic predisposition to myopia.
Amblyopia
Animal experiments have revealed that visual deprivation during a “sensitive period” results in anatomic changes in the lateral geniculate bodies and visual cortex.8,9,10 Such changes lead to a reduction in visual acuity termed amblyopia. The sensitive period in humans arguably ranges from 6 to 9 years.11,12 Visual deprivation during the first 6 weeks of life for unilateral cataracts and 10 weeks for bilateral cataracts is unlikely to cause permanent damage because of the relative visual inattentiveness of newborns.13,14,15 Following this “grace period,” however, even short intervals of visual deprivation can have profound effects on the development of the central visual pathways. As a general rule, the earlier the visual deprivation occurs, the more severe the resultant amblyopia. Unequal stimulation of the two eyes has been shown to be particularly damaging to the developing central visual pathways.16 Thus, a unilateral cataract or uncorrected aphakia has particularly deleterious effects on the visual development of the deprived eye.17 Provision of equal visual stimulation to prevent amblyopia is fundamental in deciding how best to achieve optical correction in a child.
Intraocular Lenses
Intraocular lenses are steadily gaining consensus as the preferred means of optical correction of aphakia in children more than 1 year of age. Numerous studies have shown improved visual outcomes in age-matched children corrected with IOL versus contact lenses.18,19,20,21 Based on this experience in older children, IOL implantation in infants under 1 year of age has been reported in several studies.22,23,24,25 The Infant Aphakia Treatment Study is an ongoing investigation comparing the efficacy and safety of primary IOL implantation versus contact lens optical correction for infants ages 28 to 210 days with unilateral congenital cataracts.
The improved visual outcome associated with IOL is related to the constancy of the optical correction. Even the most compliant child will have periods of time when a contact lens cannot be worn because of ocular infection or a lost or damaged lens. Pseudophakic children have been reported to have superior binocularity and a lower incidence of subsequent strabismus than children corrected with contact lenses.18
Another important benefit is the convenience of IOL. Contact lenses require a considerable amount of care, even when an extended-wear lens is appropriate. The burden of contact lens care falls on the parents. Care for these contact lenses consumes time that could be better utilized interacting with the child in more positive endeavors. Also, an IOL provides an immediate optical correction after implantation compared with a standard delay of several days to weeks before contact lenses or glasses are dispensed.26
Finally, IOL, unlike contact lenses, are not associated with ongoing expenses, making them particularly well-suited for families with limited financial resources.27
Despite the widespread acceptance of IOL for the optical correction of aphakia in children, considerable controversy exists regarding the optimal technique for IOL implantation. A child’s eye differs from an adult’s in several significant ways. First, posterior lens capsular opacification is essentially universal following cataract extraction.27 This “secondary cataract” often occurs in the first few weeks postoperatively, but may be delayed until years later.28 Older children are frequently amenable to the approach utilized with adults where the posterior capsule is left intact and opened with an Nd:YAG laser once the posterior capsule opacifies.29 Such an approach requires regular follow-up visits and a patient sufficiently cooperative to perform the YAG capsulotomy in a clinic setting. Any significant delay will necessitate excessive laser energy to clear the visual axis.30 Furthermore, the anterior hyaloid face frequently opacifies after the capsulotomy, so repeat YAG procedures or a surgical membranectomy are required.31 Alternatively, a primary posterior capsulotomy may be created with or without a simultaneous anterior vitrectomy.32,33,34 Anterior vitrectomy may be performed through the limbal incision before IOL implantation or through the pars plana after IOL implantation.35 The pars plana approach makes IOL implantation in the capsular bag less technically demanding. A randomized clinical trial failed to appreciate any difference in the outcome between the two techniques.36 An additional modification has been suggested in which the optic of the IOL is seated in the primary posterior capsular opening.37,38,39,40,41,42,43 Consensus has not been garnered in numerous studies, but primary posterior capsulotomy with anterior vitrectomy appears to be gaining popularity in recent years44,45,46,47 (Fig. 45.1).
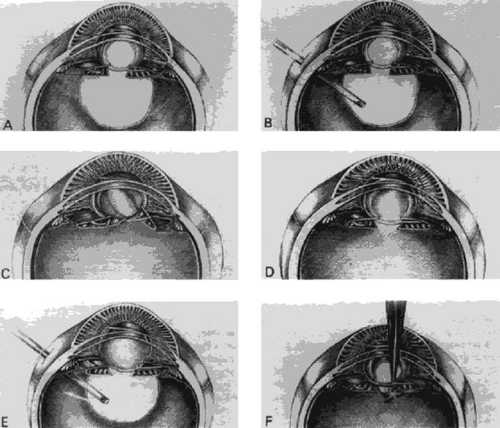 Figure 45.1. A: Intraocular lens (IOL) implanted in the capsular bag after a primary posterior capsulotomy and anterior vitrectomy through the limbal incision. B: Anterior vitrectomy and posterior capsulotomy being performed through a pars plana incision after implanting an IOL into the capsular bag through a limbal incision. C: IOL optic prolapsed through a primary posterior capsulotomy. The haptics remain in the capsular bag. The hyaloid face has been left intact. D: IOL implanted in the capsular bag after a primary posterior capsulorhexis. The hyaloid face has been left intact. E: Lensectomy and anterior vitrectomy being performed after implanting IOL in the ciliary sulcus. F: YAG laser posterior capsulotomy being performed as a secondary procedure after implanting an IOL in the capsular bag. (From Lambert SR, Drack AV: Infantile cataracts. Surv Ophthalmol 40:427–458, 1996, with permission.) |
The type of IOL implanted has an impact on the incidence of posterior capsular opacification. IOL that create a symmetric radial stretch of the posterior capsule may increase the contact between the convex IOL surface and the posterior capsule, thereby creating a barrier to the central migration of epithelial cells.48 Acrylic lenses are associated with both a lower incidence and a delayed onset of posterior capsular opacification. The reasons for this lower rate seemingly result from the square edge design of the lens, greater biocompatibility, and increased capsular adherence.49,50,51,52,53 Thus, in recent years, acrylic IOL have largely replaced polymethylmethacrylate (PMMA) lenses for pediatric aphakic correction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


