Figure 15-1 Longitudinal section of normal optic nerve. Axons of the retinal ganglion cells (R) become axonal fibers of the optic nerve. Optic nerve axons pass through the fenestrations in the lamina cribrosa (arrowheads), which is continuous with the anterior sclera (S). The posterior sclera is continuous with the dura (D). C = choroid, A = arachnoid, P = pial septa, CRA = central retinal artery, CRV = central retinal vein. (Courtesy of Tatyana Milman, MD.)
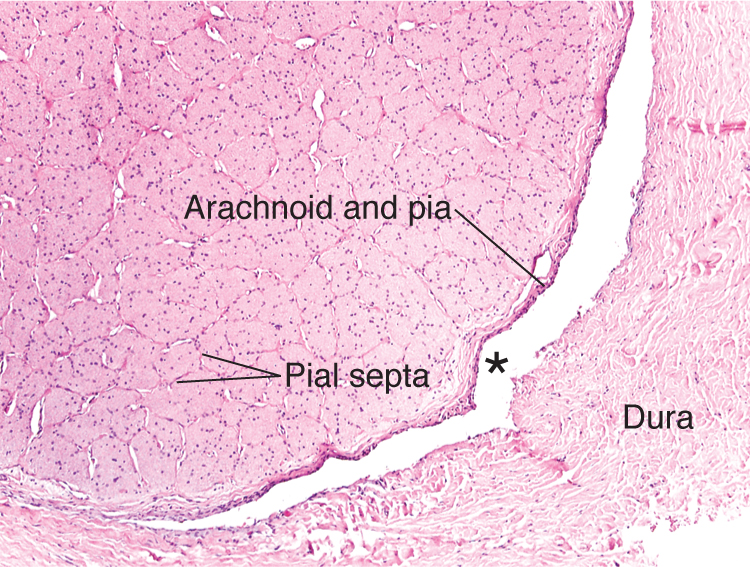
Figure 15-2 Transverse or cross section of the normal optic nerve. The axons of the optic nerve are segregated into fascicles by the delicate fibrovascular pial septa. The nuclei of oligodendrocytes, astrocytes, and microglia are present between the eosinophilic axons. The subdural space (asterisk) is relatively narrow in a normal optic nerve. (Courtesy of Tatyana Milman, MD.)
Congenital Anomalies
Numerous congenital defects can involve the optic nerve, including optic nerve hypoplasia, optic nerve head (ONH) pits (also called optic disc pits), morning glory disc anomaly, Bergmeister papilla, and optic nerve colobomas. These congenital anomalies are discussed further in BCSC Section 5, Neuro-Ophthalmology, and Section 6, Pediatric Ophthalmology and Strabismus.
Colobomas
Typical colobomas of the ONH result from defective closure of the embryonic fissure. They are often observed inferonasally in the ONH; may be associated with colobomatous defects of the retina/choroid, ciliary body, and iris; and may occur at any point along the course of the embryonic fissure (Fig 15-3A).
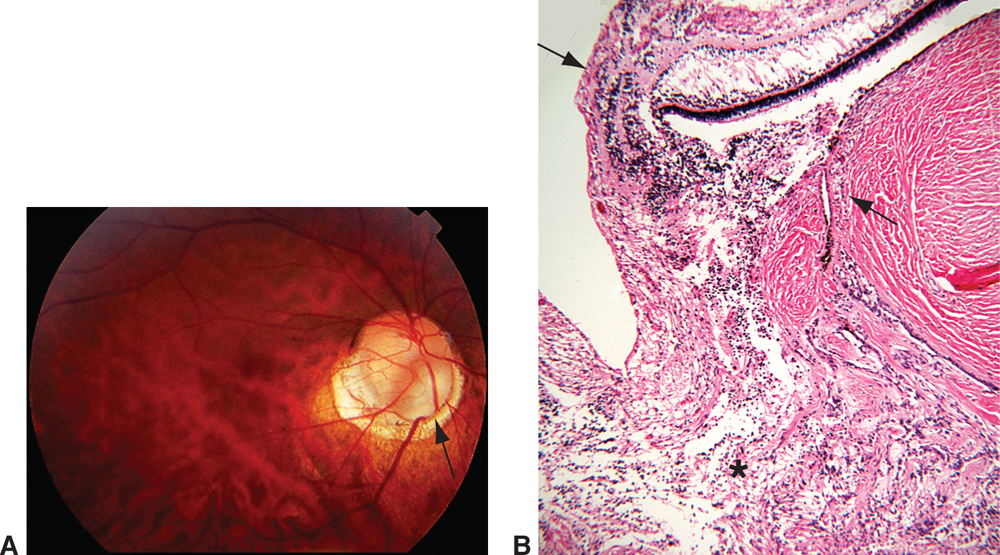
Figure 15-3 Optic nerve coloboma. A, Fundus photograph of the right eye shows a colobomatous defect in the inferonasal optic nerve (arrow). B, Photomicrograph of a gliotic, disorganized retina (asterisk) that prolapses into the defect, which is lined by excavated sclera. The normal retina, retinal pigment epithelium, and choroid terminate at the edge of the colobomatous defect (arrows). (Courtesy of Tatyana Milman, MD.)
Histologically, an optic nerve coloboma consists of a large defect in the optic nerve that involves the retina, retinal pigment epithelium, and choroid. An atrophic, gliotic retina lines the defect. The sclera is ectatic and bowed posteriorly. The wall of the defect may contain adipose tissue and even smooth muscle (see Fig 15-3B).
Inflammations
Infectious
Bacterial or fungal infections of the optic nerve can spread from adjacent anatomical structures, or they may occur as part of a systemic infection, particularly in an immunosuppressed patient. Fungal infections include mucormycosis, cryptococcosis, and coccidioidomycosis. Mucormycosis generally results from contiguous sinus infection. Cryptococcosis results from a direct extension of the infection from the CNS and often produces multiple foci of necrosis with little inflammatory reaction (Fig 15-4). Coccidioidomycosis generally begins as a primary pulmonary infection, and then spreads to the optic nerve and globe. It produces necrotizing granulomas.
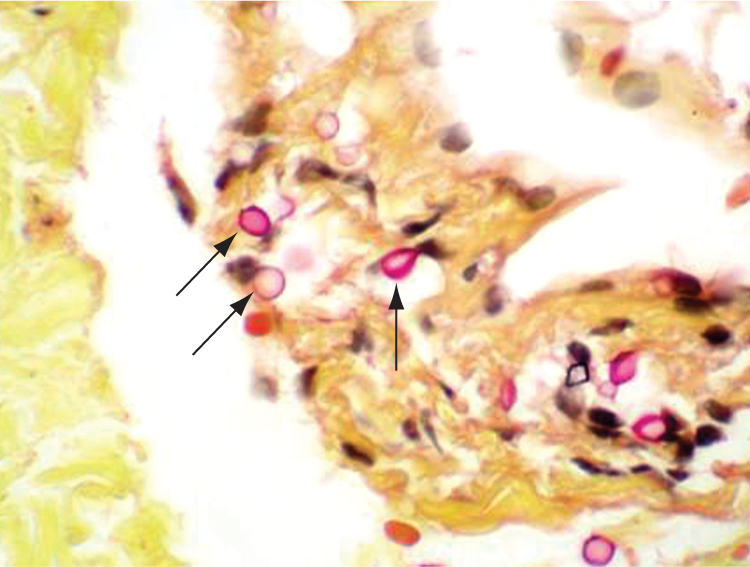
Figure 15-4 Cryptococcosis of the optic nerve in an immunocompromised patient. The dura is infiltrated by cryptococcal organisms (arrows). This yeast has a mucopolysaccharide capsule, highlighted with a mucicarmine stain. No inflammatory infiltrate is observed. (Courtesy of Tatyana Milman, MD.)
Viral infections of the optic nerve are usually associated with a more diffuse CNS process. Acute disseminated encephalomyelitis is an immune-mediated demyelinating disease that often follows bacterial or viral infections. Macrophages remove the damaged myelin. Astrocytic proliferation ultimately produces a glial scar, known as a plaque. The findings of acute disseminated encephalomyelitis are almost identical to those of multiple sclerosis (Fig 15-5).
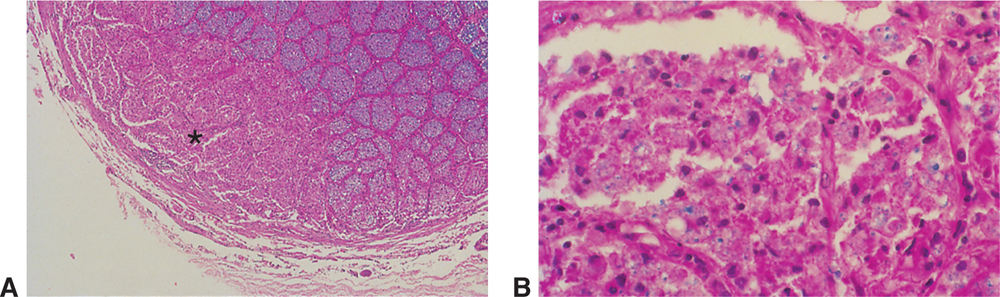
Figure 15-5 Demyelination of the optic nerve. A, Luxol fast blue stain, counterstained with H&E. The blue-staining area indicates normal myelin. Note the absence of myelin in the lower left corner of the optic nerve (asterisk), corresponding to a focal lesion. B, Higher magnification. The blue material (myelin) is engulfed by macrophages.
Noninfectious
Noninfectious inflammatory disorders of the optic nerve include giant cell arteritis and sarcoidosis. Giant cell arteritis can produce granulomatous inflammation in the blood vessel wall as well as occlusion of the posterior ciliary vessels, with liquefactive necrosis of the optic nerve. The gold standard for histologic diagnosis of giant cell arteritis is superficial temporal artery biopsy (Fig 15-6). The involvement of the vessel wall in giant cell arteritis can be patchy (ie, skip lesions). Obtaining a biopsy specimen of adequate length (approximately 2 cm) and performing a careful histologic examination of the specimen can increase its diagnostic yield.
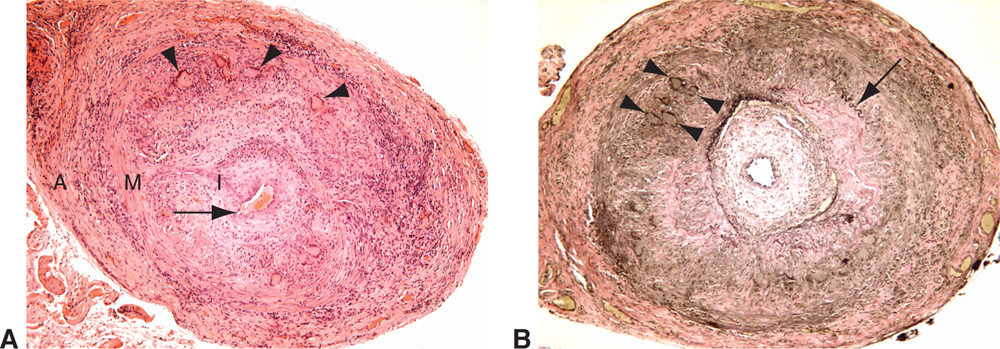
Figure 15-6 Giant cell arteritis, superficial temporal artery. A, Vascular lumen (arrow) is narrowed by concentric intimal hyperplasia. Prominent transmural inflammatory infiltrate with numerous multinucleated giant cells (arrowheads) is observed. B, An elastic stain highlights the diffuse loss of the internal elastic lamina. A short segment of remaining internal elastic lamina is marked with an arrow. Giant cells (arrowheads) are noted at the level of the internal elastic lamina. I = intima, M = media, A = adventitia. (Courtesy of Tatyana Milman, MD.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


