(1)
Department of Pathology, Duke University Medical Center, Durham, NC, USA
Abstract
This chapter will introduce the pathology of the optic nerve. Arteritis may result in ischemic damage to the optic nerve (arteritic anterior ischemic optic neuropathy), and therefore, temporal artery biopsy is also discussed here. The optic nerve is a central nerve, not a peripheral-type nerve. It is a white matter tract containing glia and axons but not ganglion cells or Schwann cells. The axons originate from the retinal ganglion cells and course posteriorly as the retinal nerve fiber layer.
This chapter will introduce the pathology of the optic nerve. Arteritis may result in ischemic damage to the optic nerve (arteritic anterior ischemic optic neuropathy), and therefore, temporal artery biopsy is also discussed here.
The optic nerve is a central nerve, not a peripheral-type nerve. It is a white matter tract containing glia and axons but not ganglion cells or Schwann cells. The axons originate from the retinal ganglion cells and course posteriorly as the retinal nerve fiber layer.
The optic nerve has a distinct histological appearance, especially in cross section (Fig. 8.1). The optic nerves are well visualized on MRI (Fig. 8.2).
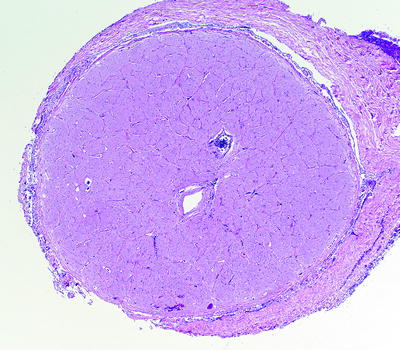
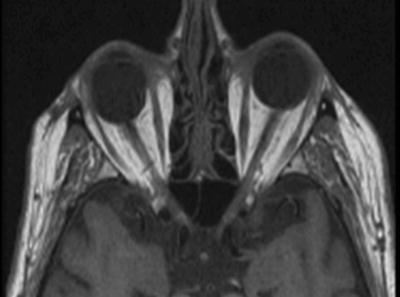
Fig. 8.1
Low-magnification cross section of the optic nerve surrounded by dura mater. Septae give the nerve a compartmentalized appearance. The central retinal artery and vein are seen
Fig. 8.2
T1-weighted MRI image showing the course of the optic nerves to the optic chiasm
Correlation with clinical and radiographic features is important when evaluating optic nerve specimens.
Outline of Optic Nerve Pathology
Optic nerve tumors:
Optic nerve gliomas
Optic nerve meningiomas
Non-neoplastic optic nerve lesions:
Optic nerve choristoma
Demyelinating disease
Granulomatous inflammation
Ischemia/infarction
Temporal Artery Biopsy
Giant cell arteritis
Healing/healed arteritis
Optic Nerve Tumors
Optic Nerve Gliomas
Gliomas of the optic nerve are traditionally thought of as pilocytic astrocytomas.
However, low-grade (pilocytic astrocytoma, diffuse astrocytoma) and high-grade (glioblastoma) astrocytomas may involve the nerve, and therefore, an attempt to best grade and classify these tumors should be made. Correlation with clinical features, neuroimaging, and intraoperative findings is recommended in these cases.
While the term “glioma” comprises astrocytic, oligodendroglial, and ependymal neoplasms, ependymal tumors have not been reported in the optic nerve, and only rare putative cases of oligodendroglioma are in the literature.
Glioneuronal tumors (ganglioglioma) are exceptionally rare in the optic nerve.
Some of the more common features of pilocytic astrocytoma and glioblastoma involving the optic nerve will be discussed:
Pilocytic Astrocytoma (WHO Grade I)
Often thought of as the traditional “optic nerve glioma”
Typically occurs in children and young adults
Usually slow growing with a favorable prognosis
Associated with NF1
Histology:
Pilocytic astrocytomas may expand the septae of the optic nerve (Fig. 8.3) or exhibit a biphasic growth pattern. Malignant astrocytomas also expand the septae and must be considered in the differential diagnosis.
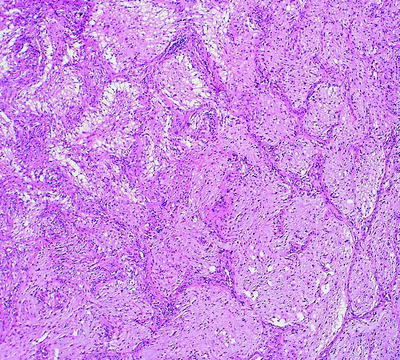
Fig. 8.3
Pilocytic astrocytoma of the optic nerve showing expansion of the septae
Squash preparations will often highlight the delicate hairlike (pilo [L.] hair) processes and granular bodies or protein droplets (Fig. 8.4).
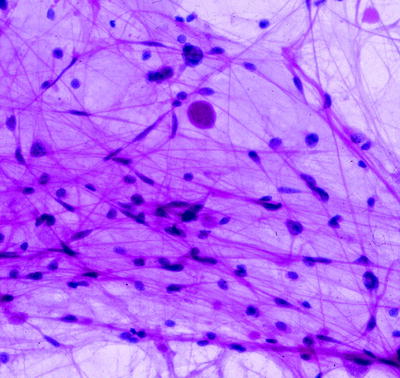
Fig. 8.4
Cytology squash preparation of an optic nerve pilocytic astrocytoma showing bipolar delicate hairlike processes and a round protein droplet. Hematoxylin and eosin staining is most useful in cytology preparations of brain tumors
Rosenthal fibers (Figs. 8.5 and 8.6) are diagnostically useful when present (sometimes they are numerous and sometimes they are scarce). The vertebrate lens protein αβ-crystallin is a major component of Rosenthal fibers.
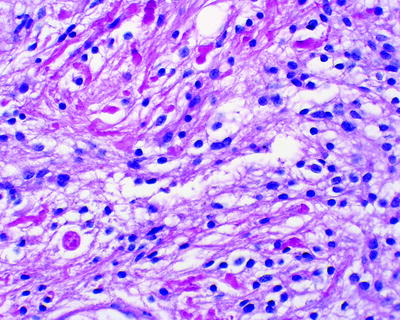
Fig. 8.5
Pilocytic astrocytoma of the optic nerve showing bright pink waxy Rosenthal fibers. A round eosinophilic granular body is seen toward the bottom left
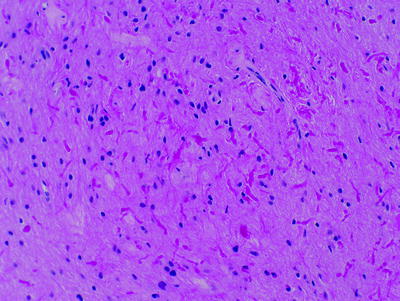
Fig. 8.6
Pilocytic astrocytoma of the optic nerve with numerous Rosenthal fibers. A case like this might be challenging to distinguish from reactive piloid gliosis
Rosenthal fibers are not specific for pilocytic astrocytoma and can also be seen in other glial tumors including ganglioglioma and pleomorphic xanthoastrocytoma. Rosenthal fibers may also be seen in hypothalamic brain tissue infiltrated by craniopharyngioma, pineal cysts, reactive tissue adjacent to syringomyelia, and Alexander disease (a neurological disorder of childhood characterized by absent myelination and numerous and often perivascular Rosenthal fibers).
Pitfalls:
Piloid gliosis can mimic and be difficult to distinguish from pilocytic astrocytoma. Optic nerve gliosis may include arachnoid gliomatosis and diffuse hyperplastic gliosis.
Diffuse leptomeningeal glioma may rarely involve the optic nerve sheath.
Optic nerve gliomas can be associated with overlying meningothelial hyperplasia that mimics meningioma. Beware of a superficial biopsy of the meninges to avoid making an incorrect diagnosis of meningioma.
On a tiny biopsy, the distinction of pilocytic astrocytoma from a diffuse or fibrillary (WHO grade II) astrocytoma might not be possible.
Some pilocytic astrocytomas exhibit anaplastic features including an increased number of mitoses, vascular proliferation, and necrosis with pseudopalisading. Beware of misdiagnosing glioblastoma (WHO grade IV) in these cases. The finding of Rosenthal fibers or eosinophilic granular bodies can be very helpful. Eosinophilic granular bodies can be identified with a periodic acid-Schiff (PAS) stain.
Pilomyxoid astrocytoma (WHO grade II) is closely related to pilocytic astrocytoma, but these tumors are more aggressive and usually involve the hypothalamic/chiasmal region in young children (Fig. 8.7). Rosenthal fibers and eosinophilic granular bodies are typically absent, and the tumor cells have perivascular orientations that resemble ependymal perivascular pseudorosettes (Fig. 8.8).
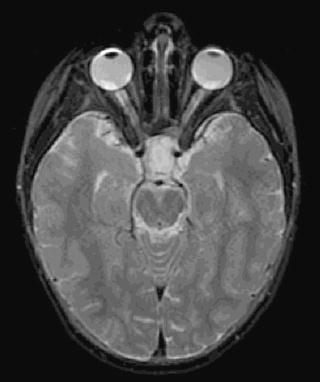
Fig. 8.7
Pilomyxoid astrocytoma. MRI FLAIR image showing a lesion in the hypothalamic/optic chiasm region
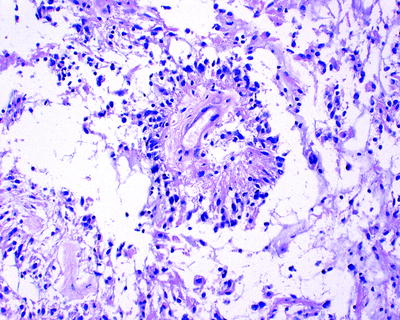
Fig. 8.8
Pilomyxoid astrocytoma characterized by perivascular tumor cell accumulations not to be mistaken for perivascular pseudorosettes of ependymoma
Glioblastoma (WHO Grade IV)
Optic nerve glioblastomas typically occur in older adults.
Patients present with unilateral or bilateral visual loss that often progresses to blindness.
They are highly invasive and usually fatal within 1 year.
Tumor may spread via the optic radiations to the occipital pole (Figs. 8.9 and 8.10). Ocular complaints may also be the initial presentation in a primary glioblastoma involving the visual cortex (Fig. 8.11).
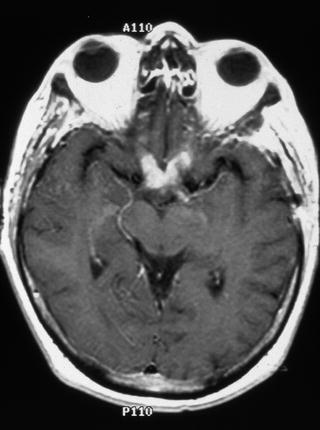
Fig. 8.9
Optic nerve glioblastoma. Contrast-enhanced T1-weighted axial magnetic resonance imaging (MRI) of the brain showing enhancement of the optic nerves and chiasm
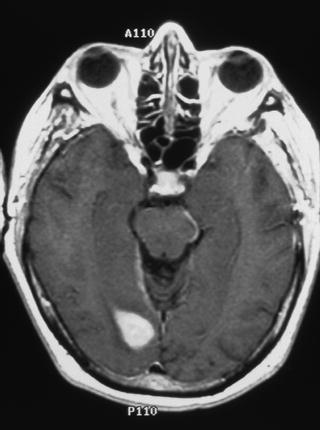
Fig. 8.10
Contrast-enhanced T1-weighted axial MRI of the brain showing extension of glioblastoma along the optic radiations to the visual cortex in the occipital pole
< div class='tao-gold-member'>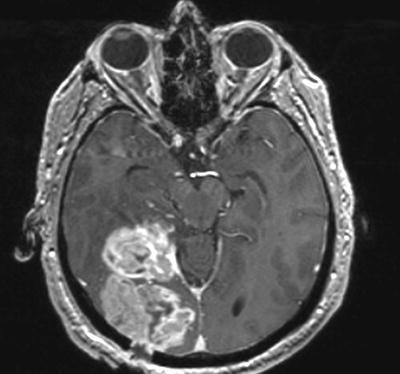 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


