Ophthalmologic Examination: Introduction
Of all the organs of the body, the eye is most accessible to direct examination. Visual function can be quantified by simple subjective testing. The external anatomy of the eye is visible to inspection with the unaided eye and with fairly simple instruments. With more complicated instruments, the interior of the eye is visible through the clear cornea. The eye is the only part of the body where blood vessels and central nervous system tissue (retina and optic nerve) can be viewed directly. Important systemic effects of infectious, autoimmune, neoplastic, and vascular diseases may be identified from ocular examination.
Ocular History
The chief complaint is characterized according to its duration, frequency, intermittency, and rapidity of onset. The location, the severity, and the circumstances surrounding onset are important, as well as any associated symptoms. Current eye medications being used and all other current and past ocular disorders are recorded, and a review of other pertinent ocular symptoms is performed.
The past medical history centers on the patient’s general state of health and principal systemic illnesses, if any. Vascular disorders commonly associated with ocular manifestations—such as diabetes and hypertension—should be asked about specifically. Just as a general medical history should include ocular medications being used, the eye history should list the patient’s systemic medications. This provides a general indication of health status and may include medications that affect ocular health, such as corticosteroids. Finally, any drug allergies should be recorded.
The family history is pertinent for ocular disorders, such as strabismus, amblyopia, glaucoma, or cataracts, and retinal problems, such as retinal detachment or macular degeneration. Medical diseases such as diabetes may be relevant as well.
A basic understanding of ocular symptomatology is necessary for performing a proper ophthalmic examination. Ocular symptoms can be divided into three basic categories: abnormalities of vision, abnormalities of ocular appearance, and abnormalities of ocular sensation—pain and discomfort.
Symptoms and complaints should always be fully characterized. Was the onset gradual, rapid, or asymptomatic? (For example, was blurred vision in one eye not discovered until the opposite eye was inadvertently covered?) Was the duration brief, or has the symptom continued until the present visit? If the symptom was intermittent, what was the frequency? Is the location focal or diffuse, and is involvement unilateral or bilateral? Finally, does the patient characterize the degree as mild, moderate, or severe?
One should also determine what therapeutic measures have been tried and to what extent they have helped. Has the patient identified circumstances that trigger or worsen the symptom? Have similar instances occurred before, and are there any other associated symptoms?
The following is a brief overview of ocular complaints. Representative examples of some causes are given here and discussed more fully elsewhere in this book.
Loss of visual acuity may be due to abnormalities anywhere along the optical and neurologic visual pathway. One must therefore consider refractive (focusing) error, lid ptosis, clouding or interference from the ocular media (eg, corneal edema, cataract, or hemorrhage in the vitreous or aqueous space), and malfunction of the retina (macula), optic nerve, or intracranial visual pathway.
A distinction should be made between decreased central acuity and peripheral vision. The latter may be focal, such as a scotoma, or more expansive, as with hemianopia. Abnormalities of the intracranial visual pathway usually disturb the visual field more than central visual acuity.
Transient loss of central or peripheral vision is frequently due to circulatory changes anywhere along the neurologic visual pathway from the retina to the occipital cortex, for example amaurosis fugax and migrainous scotoma.
The degree of visual impairment may vary under different circumstances. For example, uncorrected nearsighted refractive error may seem worse in dark environments. This is because pupillary dilation allows more misfocused rays to reach the retina, increasing the blur. A central focal cataract may seem worse in sunlight. In this case, pupillary constriction prevents more rays from entering and passing around the lens opacity. Blurred vision from corneal edema may improve as the day progresses owing to corneal dehydration from surface evaporation.
Glare or halos may result from uncorrected refractive error, scratches on spectacle lenses, excessive pupillary dilation, and hazy ocular media, such as corneal edema or cataract. Visual distortion (apart from blurring) may be manifested as an irregular pattern of dimness, wavy or jagged lines, and image magnification or minification. Causes may include the aura of migraine, optical distortion from strong corrective lenses, or lesions involving the macula and optic nerve. Flashing or flickering lights may indicate retinal traction (if instantaneous) or migrainous scintillations that last for several seconds or minutes. Floating spots may represent normal vitreous strands due to vitreous “syneresis” or separation (see Chapter 9) or the pathologic presence of pigment, blood, or inflammatory cells. Oscillopsia is a shaking field of vision due to ocular instability.
It must be determined whether double vision is monocular or binocular (ie, disappears if one eye is covered). Monocular diplopia is often a split shadow or ghost image. Causes include uncorrected refractive error, such as astigmatism, or focal media abnormalities, such as cataracts or corneal irregularities (eg, scars, keratoconus). Binocular diplopia (see Chapters 12 and 14) can be vertical, horizontal, diagonal, or torsional. If the deviation occurs or increases in one gaze direction as opposed to others, it is called “incomitant.” Neuromuscular dysfunction or mechanical restriction of globe rotation is suspected. “Comitant” deviation is one that remains constant regardless of the direction of gaze. It is usually due to childhood or long-standing strabismus.
Complaints of “red eye” call for differentiation between redness of the lids and periocular area versus redness of the globe. The latter can be caused by subconjunctival hemorrhage or by vascular congestion of the conjunctiva, sclera, or episclera (connective tissue between the sclera and conjunctiva). Causes of such congestion may be either external surface inflammation, such as conjunctivitis and keratitis, or intraocular inflammation, such as iritis and acute glaucoma (see Differential Diagnosis of Common Causes of the Inflamed Eye). Color abnormalities other than redness may include jaundice and hyperpigmented spots on the iris or outer ocular surface.
Other changes in appearance of the globe that may be noticeable to the patient include focal lesions of the ocular surface, such as a pterygium, and asymmetry of pupil size (anisocoria). The lids and periocular tissues may be the source of visible signs, such as edema, redness, focal growths, and lesions, and abnormal position or contour, such as ptosis. Finally, the patient may notice bulging or displacement of the globe, such as with exophthalmos.
“Eye pain” may be periocular, ocular, retrobulbar (behind the globe), or poorly localized. Examples of periocular pain are tenderness of the lid, tear sac, sinuses, or temporal artery. Retrobulbar pain can be due to orbital inflammation of any kind. Certain locations of inflammation, such as optic neuritis or orbital myositis, may produce pain on eye movement. Many nonspecific complaints such, as “eyestrain,” “pulling,” “pressure,” “fullness,” and certain kinds of “headaches,” are poorly localized. Causes may include fatigue from ocular accommodation or binocular fusion or referred discomfort from nonocular muscle tension or fatigue.
Ocular pain itself may seem to emanate from the surface or from deeper within the globe. Corneal epithelial damage typically produces a superficial sharp pain or foreign body sensation exacerbated by blinking. Topical anesthesia will immediately relieve this pain. Deeper internal aching pain occurs with acute glaucoma, iritis, endophthalmitis, and scleritis. The globe is often tender to palpation in these situations. Reflex spasm of the ciliary muscle and iris sphincter can occur with iritis or keratitis, producing brow ache and painful “photophobia” (light sensitivity). This discomfort is markedly improved by instillation of cycloplegic/mydriatic agents (see Chapter 22).
Superficial ocular discomfort usually results from surface abnormalities. Itching, as a primary symptom, is often a sign of allergic sensitivity. Symptoms of dryness, burning, grittiness, and mild foreign body sensation can occur with dry eyes or other types of mild corneal irritation. Tearing may be of two general types. Sudden reflex tearing is usually due to irritation of the ocular surface. In contrast, chronic watering and “epiphora” (tears rolling down the cheek) may indicate abnormal lacrimal drainage (see Chapter 4).
Ocular secretions are often diagnostically nonspecific. Severe amounts of discharge that cause the lids to be glued shut upon awakening usually indicate viral or bacterial conjunctivitis. More scant amounts of mucoid discharge can also be seen with allergic and noninfectious irritations. Dried matter and crusts on the lashes may occur acutely with conjunctivitis or chronically with blepharitis (lid margin inflammation).
Basic Ophthalmologic Examination
The purpose of the ophthalmologic physical examination is to evaluate both the function and the anatomy of the two eyes. Function includes vision and nonvisual functions, such as eye movements and alignment. Anatomically, ocular problems can be subdivided into three areas: those of the adnexa (lids and periocular tissue), the globe, and the orbit.
Just as assessment of vital signs is a part of every physical examination, any ocular examination must include assessment of vision, regardless of whether vision is mentioned as part of the chief complaint. Good vision results from a combination of an intact neurologic visual pathway, a structurally healthy eye, and proper focus of the eye. An analogy might be made to a video camera, requiring a functioning cable connection to the monitor, a mechanically intact camera body, and a proper focus setting. Vision can be divided broadly into central and peripheral, quantified by visual acuity and visual field testing, respectively. Clinical assessment of visual acuity and visual field is subjective rather than objective, since it requires responses on the part of the patient.
Visual acuity can be tested either for distance or near, conventionally at 20 feet (6 meters) and 14 inches (33 cms) away, respectively, but distance acuity is the general standard for comparison. For diagnostic purposes visual acuity is always tested separately for each eye, whereas binocular visual acuity is useful for assessing functional vision (see Chapter 25), such as for assessing the eligibility to drive.
Visual acuity is measured with a display of different-sized optotypes shown at the appropriate distance from the eye. The familiar “Snellen chart” is composed of rows of progressively smaller letters, each row designated by a number corresponding to the distance in feet (or meters) from which a normal eye can read the letters of the row. For example, the letters in the “40” row are large enough for the normal eye to see from 40 feet away. Whereas wall-mounted illuminated charts, or projection systems are commonly used, wall-mounted LCD screens provide better standardization and calibration (Figure 2–1). Mainly for clinical trials but increasingly for specific clinical situations, LogMAR charts are being used (see Chapter 24).
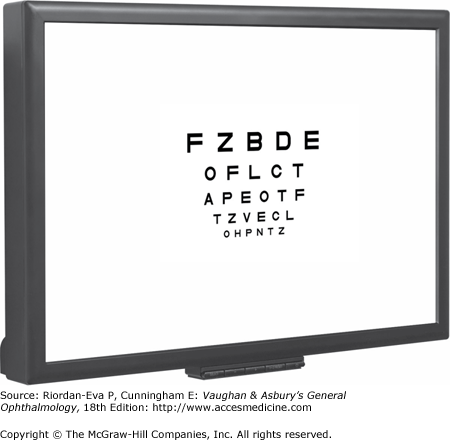
Visual acuity is scored as a fraction (eg, “20/40”). The first number represents the testing distance between the chart and the patient, and the second number represents the smallest row of letters that the patient’s eye can read. Hence normal vision is 20/20 and 20/60 acuity indicates that the patient’s eye can only read from 20 feet letters large enough for a normal eye to read from 60 feet.
Charts containing numerals can be used for patients not familiar with the English alphabet. The “illiterate E” chart is used to test small children or if there is a language barrier. “E” figures are randomly rotated in each of four different orientations throughout the chart. For each target, the patient is asked to point in the same direction as the three “bars” of the E (Figure 2–2). Most children can be tested in this manner beginning at about age 3½ years.

Uncorrected visual acuity is measured without glasses or contact lenses. Corrected acuity means that these aids were worn. Since poor uncorrected distance acuity may simply be due to refractive error, corrected visual acuity is a more relevant assessment of ocular health.
If the patient needs glasses or if his or her glasses are unavailable, the corrected acuity can be estimated by testing vision through a “pinhole.” Refractive blur (eg, myopia, hyperopia, astigmatism) is caused by multiple misfocused rays entering through the pupil and reaching the retina. This prevents formation of a sharply focused image.
Viewing the Snellen chart through a placard of multiple tiny pinhole-sized openings prevents most of the misfocused rays from entering the eye. Only a few centrally aligned focused rays will reach the retina, resulting in a sharper image. In this manner, the patient may be able to read within one or two lines of what would be possible if proper corrective glasses were being used.
The unaided distant focal point of the eye varies among normal individuals depending on the shape of the globe and the cornea (Figure 2–3). An emmetropic eye is naturally in optimal focus for distance vision. An ametropic eye (ie, one with myopia, hyperopia, or astigmatism) needs corrective lenses to be in proper focus for distance. This optical abnormality is called refractive error.
Figure 2-3.

Common imperfections of the optical system of the eye (refractive errors). Ideally, light rays from a distant target should automatically arrive in focus on the retina if the retina is situated precisely at the eye’s natural focal point. Such an eye is called emmetropic. In hyperopia (“farsightedness”), the light rays from a distant target instead come to a focus behind the retina, causing the retinal image to be blurred. A biconvex (+) lens corrects this by increasing the refractive power of the eye and shifting the focal point forward. In myopia (“nearsightedness”), the light rays come to a focus in front of the retina, as though the eyeball is too long. Placing a biconcave (–) lens in front of the eye diverges the incoming light rays; this effectively weakens the optical power of the eye enough so that the focus is shifted backward and onto the retina. (Modified and reproduced, with permission, from Ganong WF: Review of Medical Physiology, 15th ed. McGraw-Hill, 1991.)
Refraction is the procedure by which any refractive error is characterized and quantified (Figure 2–4) (see Chapter 21), allowing the best measure of corrected visual acuity. In addition, it is the most reliable means to distinguish between blurred vision caused by refractive error or by other abnormalities of the visual system. Thus, in addition to being the basis for prescription of corrective glasses or contact lenses, refraction serves a crucial diagnostic function.
Figure 2-4.
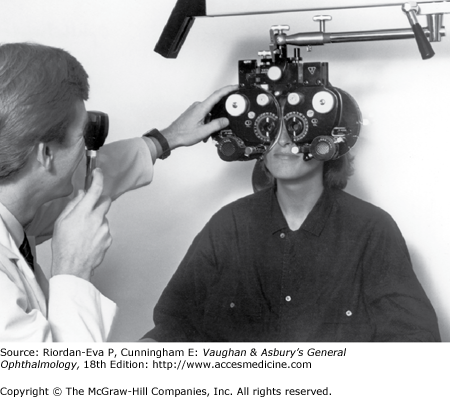
Refraction being performed using a “phoropter.” This device contains the complete range of corrective lens powers, which can quickly be changed back and forth, allowing the patient to subjectively compare various combinations while viewing the eye chart at a distance. (Photo by M Narahara.)
The patient unable to read the largest (“20/200”) letter on a Snellen chart should be moved closer to the chart until that letter can be read. The distance from the chart is then recorded as the first number. Visual acuity of “5/200” means that the patient can identify correctly the largest letter from a distance of 5 feet but not further away. An eye unable to read any letters is tested by the ability to count fingers. “CF at 2 ft” indicates that the eye was able to count fingers held 2 feet away but not farther away. If counting fingers is not possible, the eye may be able to detect a hand moving vertically or horizontally (“HM,” or “hand motions” vision). The next lower level of vision would be the ability to perceive light (“LP,” or “light perception”). An eye that is totally blind is recorded as having no light perception (“NLP”).
Visual field testing should be included in every complete ophthalmologic examination because even dense visual field abnormalities may not be apparent to the patient. Since the visual fields of the two eyes overlap, for diagnostic purposes each eye must be tested separately. Binocular visual field testing is useful in assessment of functional vision (see Chapter 25).
Assessment of visual fields can be quickly achieved using confrontation testing. The patient is seated facing the examiner with one eye covered while the examiner closes the opposite eye (eg, the patient’s left eye is covered and the examiner’s right eye is closed so that the patient’s right eye looks into the examiner’s left eye). Presentation of targets at a distance halfway between the patient and the examiner allows direct comparison of the field of vision of each eye of the patient and the examiner. Since the patient and examiner are staring eye to eye, any loss of fixation by the patient will be noticed.
For gross assessment, the examiner briefly shows a number of fingers of one hand (usually one, two, or four fingers) peripherally in each of the four quadrants. The patient must identify the number of fingers flashed while maintaining straight-ahead fixation. The upper and lower temporal and the upper and lower nasal quadrants are all tested in this fashion for each eye.
A 5-mm-diameter red sphere or disk attached to a handle as the target allows detection and quantification of more subtle visual field defects, particularly if areas of abnormal reduction in color (desaturation) are sought.
In disease of the right cerebral hemisphere, particularly involving the parietal lobe, there may be visual neglect (visual inattention) in which there is no comparable visual field loss on testing of each eye separately, but objects are not identified in the left hemifield of either eye if objects are simultaneously presented in the right hemifield. The patient functions as if there is a left homonymous hemianopia. Visual neglect is detected by simultaneous confrontation testing. The examiner holds both hands out peripherally, one on each side. The patient, with both eyes open, is asked to signify on which side (right, left, or both) the examiner is intermittently wiggling his or her fingers. The patient will still be able to detect the fingers in the left hemifield when wiggled alone but not when the fingers in the right hemifield are wiggled simultaneously.
More sophisticated means of visual field testing, important for detection of subtle visual field loss, such as in the diagnosis of early glaucoma and for quantification of any visual field defect, are discussed later in this chapter.
The pupils should be symmetric, and each one should be examined for size, shape (circular or irregular), and reactivity to both light and accommodation. Pupillary abnormalities may be due to (1) neurologic disease, (2) intraocular inflammation causing either spasm of the pupillary sphincter or adhesions of the iris to the lens (posterior synechiae), (3) markedly elevated intraocular pressure causing atony of the pupillary sphincter, (4) prior surgical alteration, (5) the effect of systemic or eye medications, and (6) benign variations of normal.
To avoid accommodation, the patient is asked to fixate on a distant target as a penlight is directed toward each eye. Dim lighting conditions help to accentuate the pupillary response and may best demonstrate an abnormally small pupil. Likewise, an abnormally large pupil may be more apparent in brighter background illumination. The direct response to light refers to constriction of the illuminated pupil. The reaction may be graded as either brisk or sluggish. The consensual response is the normal simultaneous constriction of the opposite nonilluminated pupil. The neuroanatomy of the pupillary pathway is discussed in Chapter 14.
As a light is swung back and forth in front of the two pupils, one can compare the reactions to stimulation of each eye, which should be equal. If the neural response to stimulation of the left eye is impaired, the pupil response in both eyes will be reduced on stimulation of the left eye compared to stimulation of the right eye. As the light is swung from the right to the left eye, both pupils will begin to dilate normally as the light is moved away from the right eye and then not constrict or paradoxically widen as the light is shone into the left eye (since the direct response in the left eye and the consensual response in the right eye are reduced compared to the consensual response in the left eye and direct response in the right eye from stimulation of the right eye). When the light is swung back to the right eye, both pupils will begin to dilate as the light is moved away from the left eye and then constrict normally as the light is shone into the right eye. This phenomenon is called a relative afferent pupillary defect (RAPD). It is usually a sign of optic nerve disease but may occur in retinal disease. Importantly, it does not occur in media opacities such as corneal disease, cataract, and vitreous hemorrhage. Because the pupils are normal in size and may appear to react normally when each is stimulated alone, the swinging flashlight test is the only means of demonstrating a relative afferent pupillary defect. Also, because the pupils react equally, detection of a relative afferent pupillary defect requires inspection of only one pupil and can still be achieved when one pupil is structurally damaged or cannot be visualized, as in dense corneal opacity. Relative afferent pupillary defect is further discussed and illustrated in Chapter 14.
The objective of ocular motility testing is to evaluate the alignment of the eyes and their movements, both individually (“ductions”) and in tandem (“versions”). A more complete discussion of ocular motility testing and eye movement abnormalities is presented in Chapters 12 and 14.
Normal patients have binocular vision. Since each eye generates a visual image separate from and independent of that of the other eye, the brain must be able to fuse the two images in order to avoid “double vision.” This is achieved by having each eye positioned so that both foveas are simultaneously fixating on the object of regard.
A simple test of binocular alignment is performed by having the patient look toward a penlight held several feet away. A pinpoint light reflection, or “reflex,” should appear on each cornea and should be centered over each pupil if the two eyes are straight in their alignment. If the eye positions are convergent, such that one eye points inward (“esotropia”), the light reflex will appear temporal to the pupil in that eye. If the eyes are divergent, such that one eye points outward (“exotropia”), the light reflex will be located more nasally in that eye. This test can be used with infants.
The cover test (see Chapter 12) is a more accurate method of verifying normal ocular alignment. The test requires good vision in both eyes. The patient is asked to gaze at a distant target with both eyes open. If both eyes are fixating together on the target, covering one eye should not affect the position or continued fixation of the other eye.
To perform the test, the examiner suddenly covers one eye and carefully watches to see that the second eye does not move (indicating that it was fixating on the same target already). If the second eye was not identically aligned but was instead turned abnormally inward or outward, it could not have been simultaneously fixating on the target. Thus, it will have to quickly move to find the target once the previously fixating eye is covered. Fixation of each eye is tested in turn.
An abnormal cover test is expected in patients with diplopia. However, diplopia is not always present in many patients with long-standing ocular misalignment. When the test is abnormal, prism lenses of different power can be used to neutralize the refixation movement of the misaligned eye (prism cover test). In this way, the amount of eye deviation can be quantified based on the amount of prism power needed.
The patient is asked to follow a target with both eyes as it is moved in each of the four cardinal directions of gaze. The examiner notes the speed, smoothness, range, and symmetry of movements and observes for unsteadiness of fixation (eg, nystagmus).
Impairment of eye movements can be due to neurologic problems (eg, cranial nerve palsy), primary extraocular muscular weakness (eg, myasthenia gravis), or mechanical constraints within the orbit limiting rotation of the globe (eg, orbital floor fracture with entrapment of the inferior rectus muscle). Deviation of ocular alignment that is the same amount in all directions of gaze is called “comitant.” It is “incomitant” if the amount of deviation varies with the direction of gaze.
Before studying the eye under magnification, a general external examination of the ocular adnexa (eyelids and periocular area) is performed. Skin lesions, growths, and inflammatory signs such as swelling, erythema, warmth, and tenderness are evaluated by gross inspection and palpation.
The positions of the eyelids are checked for abnormalities, such as ptosis or lid retraction. Asymmetry can be quantified by measuring the central width (in millimeters) of the “palpebral fissure”—the space between the upper and lower lid margins. Abnormal motor function of the lids, such as impairment of upper lid elevation or forceful lid closure, may be due to either neurologic or primary muscular abnormalities.
Malposition of the globe, such as proptosis, may occur in orbital disease. Palpation of the bony orbital rim and periocular soft tissue should always be done in instances of suspected orbital trauma, infection, or neoplasm. The general facial examination may contribute other pertinent information as well. Depending on the circumstances, checking for enlarged preauricular lymph nodes, sinus tenderness, temporal artery prominence, or skin or mucous membrane abnormalities may be diagnostically relevant.
The slitlamp (Figure 2–5) is a table-mounted binocular microscope with a special adjustable illumination source attached. A linear slit beam of incandescent light is projected onto the globe, illuminating an optical cross section of the eye (Figure 2–6). The angle of illumination can be varied along with the width, length, and intensity of the light beam. The magnification can be adjusted as well (normally 10× to 16× power). Since the slitlamp is a binocular microscope, the view is “stereoscopic,” or three-dimensional.

Figure 2-6.

Slitlamp photograph of a normal right eye. The curved slit of light to the right is reflected off of the cornea (C), while the slit to the left is reflected off of the iris (I). As the latter slit passes through the pupil, the anterior lens (L) is faintly illuminated in cross section. (Photo by M Narahara.)
The patient is seated while being examined, and the head is stabilized by an adjustable chin rest and forehead strap. Using the slitlamp alone, the anterior half of the globe—the “anterior segment”—can be visualized. Details of the lid margins and lashes, the palpebral and bulbar conjunctival surfaces, the tear film and cornea, the iris, and the aqueous can be studied. Through a dilated pupil, the crystalline lens and the anterior vitreous can be examined as well.
Because the slit beam of light provides an optical cross section of the eye, the precise anteroposterior location of abnormalities can be determined within each of the clear ocular structures (eg, cornea, lens, vitreous body). The highest magnification setting is sufficient to show the abnormal presence of cells within the aqueous, such as red or white blood cells or pigment granules. Aqueous turbidity, called “flare,” resulting from increased protein concentration can be detected in the presence of intraocular inflammation. Normal aqueous is optically clear, without cells or flare.
The eye examination with the slitlamp is supplemented by the use of various techniques. Tonometry is discussed separately in a subsequent section.
Lid eversion, to examine the undersurface of the upper lid, can be performed either at the slitlamp or without the aid of that instrument. It should always be done if the presence of a superficial foreign body is suspected but not already identified (see Chapter 19). A semirigid plate of cartilage called the tarsus gives each lid its contour and shape. In the upper lid, the superior edge of the tarsus lies centrally about 8–9 mm above the lashes. On the undersurface of the lid, it is covered by the tarsal palpebral conjunctiva.
Following topical anesthesia, the patient is positioned at the slitlamp and instructed to look down. The examiner gently grasps the upper lashes with the thumb and index finger of one hand while using the other hand to position an applicator handle just above the superior edge of the tarsus (Figure 2–7). The lid is everted by applying slight downward pressure with the applicator as the lash margin is simultaneously lifted. The patient continues to look down, and the lashes are held pinned to the skin overlying the superior orbital rim as the applicator is withdrawn. The tarsal conjunctiva is then examined under magnification. To undo eversion, the lid margin is gently stroked downward as the patient looks up.
Figure 2-7.
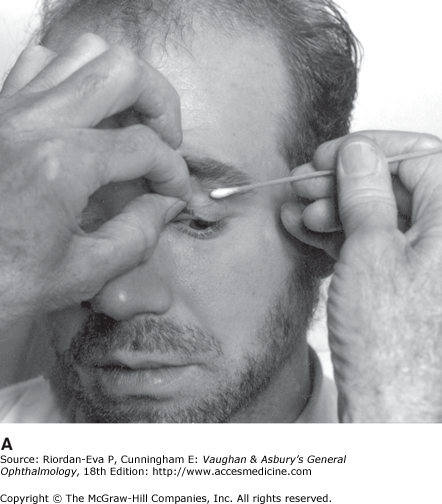
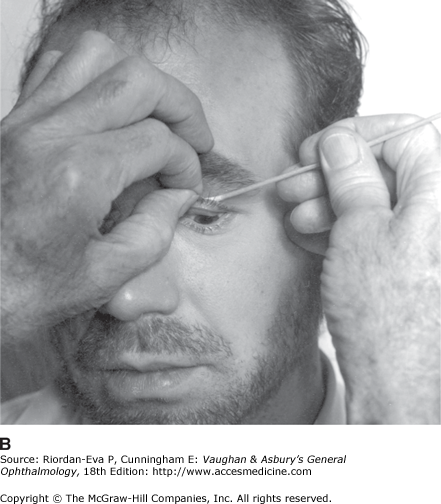
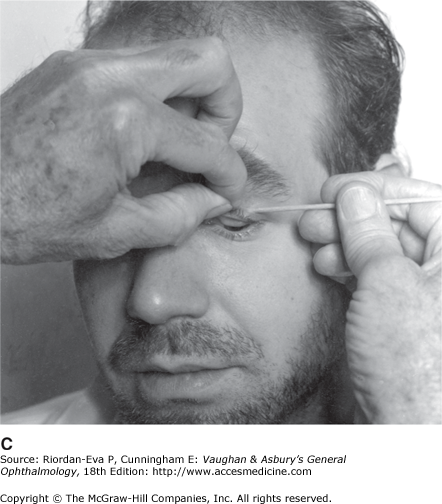
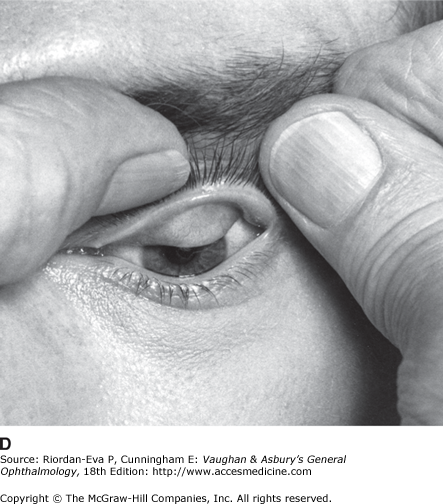
Technique of lid eversion. A: With the patient looking down, the upper lashes are grasped with one hand as an applicator stick is positioned at the superior edge of the upper tarsus (at the upper lid crease). B and C: As the lashes are lifted, slight downward pressure is simultaneously applied with the applicator stick. D: The thumb pins the lashes against the superior orbital rim, allowing examination of the undersurface of the tarsus. (Photos by M Narahara.)
Fluorescein is a specialized dye that stains the cornea and highlights any irregularities of its epithelial surface. Sterile paper strips containing fluorescein are wetted with sterile saline or local anesthetic and touched against the inner surface of the lower lid, instilling the yellowish dye into the tear film. The illuminating light of the slitlamp is made blue with a filter, causing the dye to fluoresce.
A uniform film of dye should cover the normal cornea. If the corneal surface is abnormal, excessive amounts of dye will absorb into or collect within the affected area. Abnormalities can range from tiny punctate dots, such as those resulting from excessive dryness or ultraviolet light damage, to large geographic defects in the epithelium, such as those seen in corneal abrasions or infectious ulcers.
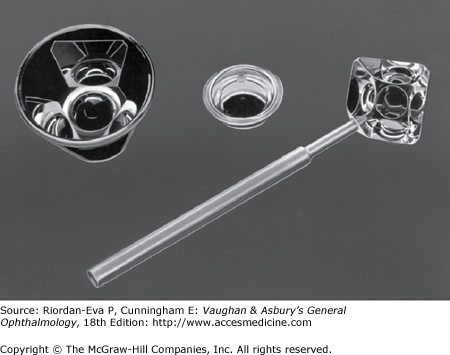
Special examining lenses can expand and further magnify the slitlamp examination of the eye’s interior. A goniolens (Figure 2–8) provides visualization of the anterior chamber “angle” formed by the iridocorneal junction. Other lenses placed on or in front of the eye allow slitlamp evaluation of the posterior half of the globe’s interior—the “posterior segment.” Since the slitlamp is a binocular microscope, these lenses provide a magnified three-dimensional view of the posterior vitreous, the fundus, and the disk. Examples are the Goldmann-style three-mirror lens (Figure 2–8) and the Volk-style range of lenses.
Special attachments to the slitlamp allow it to be used with several techniques requiring microscopic visualization. Special camera bodies can be attached for photographic documentation and for special applications such as corneal endothelial cell studies. Special instruments for the study of visual potential require attachment to the slitlamp. Finally, laser sources are attached to a slitlamp to allow microscopic visualization and control of eye treatment.
The globe can be thought of as an enclosed compartment through which there is a constant circulation of aqueous humor. This fluid maintains the shape and a relatively uniform pressure within the globe. Tonometry is the method of measuring intraocular pressure using calibrated instruments. The normal range is 10 to 21 mm Hg.
In applanation tonometry, intraocular pressure is determined by the force required to flatten the cornea by a standard amount. The force required increases with intraocular pressures. The Schiotz tonometer, now rarely used, measures the amount of corneal indentation produced by preset weights. Less corneal indentation is produced as intraocular pressure rises. Since both methods employ devices that touch the patient’s cornea, they require topical anesthetic and disinfection of the instrument tip prior to use. (Tonometer disinfection techniques are discussed in Chapter 21.) With any method of tonometry, care must be taken to avoid pressing on the globe and artificially increasing its pressure.
The Goldmann applanation tonometer (Figure 2–9) is attached to the slitlamp and measures the amount of force required to flatten the corneal apex by a standard amount. The higher the intraocular pressure, the greater the force required. Since Goldmann applanation tonometer is a more accurate method than Schiotz tonometry, it is preferred by ophthalmologists.
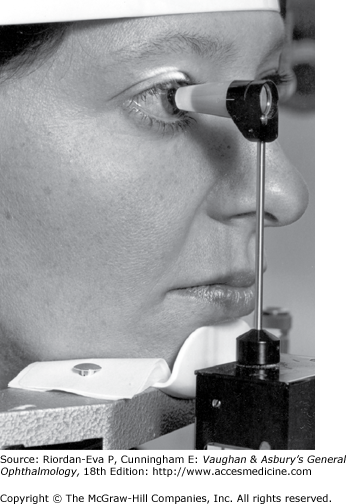
Following topical anesthesia and instillation of fluorescein, the patient is positioned at the slitlamp and the tonometer is swung into place. To visualize the fluorescein, the cobalt blue filter is used with the brightest illumination setting. After grossly aligning the tonometer in front of the cornea, the examiner looks through the slitlamp ocular just as the tip contacts the cornea. A manually controlled counterbalanced spring varies the force applied by the tonometer tip.
Upon contact, the tonometer tip flattens the central cornea and produces a thin circular outline of fluorescein. A prism in the tip visually splits this circle into two semicircles that appear green while viewed through the slitlamp oculars. The tonometer force is adjusted manually until the two semicircles just overlap, as shown in Figure 2–10. This visual end point indicates that the cornea has been flattened by the set standard amount. The amount of force required to do this is translated by the scale into a pressure reading in millimeters of mercury.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


