Ophthalmic Trauma: Introduction
Ophthalmic trauma occurs in many settings and manifests in many ways, with widely different degrees of severity. It can result in a broad range of permanent problems, including mild to total visual loss in one or both eyes, temporary or persistent diplopia, minor to severe cosmetic abnormalities of the eyes and face, and ocular or periocular pain.
Patients with ophthalmic trauma may be of any age and either sex, and may have any extent of preexistent abnormality of the eyes, eyelids, or orbits. Their injuries may be confined to the eyes or associated with facial, head, or other potentially life-threatening injuries. Commonly the patients are fully conscious and aware of their circumstances and surroundings, but they may be affected by drugs, alcohol, or psychiatric disease. In cases of severe trauma with head injury, including when elective sedation and ventilation have been undertaken to manage cerebral injury, or when sedation has been required for other reasons, such as intubation and ventilation for airway compromise in facial injuries or severe chest injury, they may be unconscious and unresponsive.
Initial evaluation of a patient with ophthalmic trauma is frequently undertaken by a paramedic at the scene of the incident, or in an emergency room by a triage nurse or physician, who primarily is responsible for assessing the injured person’s overall condition, identifying any potentially life-threatening problems that require priority treatment. Once the management of any immediately life-threatening injuries has been determined, and the patient’s general condition has been stabilized, the ophthalmic injuries can be assessed, either by emergency room staff or an ophthalmologist depending upon the circumstances.
It is essential to establish as precisely as possible the circumstances and mechanism of injury and any preexisting ophthalmic abnormality, not only to optimize the ophthalmic care but also in case of subsequent legal action for personal injury. Surprisingly frequently the crucial history of hammering metal on metal, from which penetrating injury needs to be assumed until proven otherwise, is missed. Particularly if the patient is unconscious or unable to provide enough information, persons present at the time of the injury or when the patient was found, including paramedics, should be questioned about the circumstances, and family members or friends should be asked about any preexisting ophthalmic condition.
Cooperative patients should be questioned about any subjective change in vision of either eye, pain, including foreign body sensation that would suggest ocular surface abnormality including corneal or subtarsal foreign body, or corneal abrasion, and tetanus immunization status, which might also be obtainable from a family member, especially for children.
Although it is vitally important to obtain as much information as possible about vision, ocular motility, pupillary function, and any structural damage to the eyes and periocular tissues, it is crucial that examination does not exacerbate any ocular damage, a particular example being pressure on the globe to open swollen eyelids causing extrusion of intraocular contents when there is an open globe injury. Emergency room staff should not hesitate to seek assistance from an ophthalmologist. If an open globe injury is suspected, the eye should be protected by an eye shield to avoid inadvertent pressure on the globe. In some cases of severe trauma, it is quickly apparent that little can be achieved without examination under anesthesia, although even then assessment, if possible, should include measurement of vision and assessment of pupillary function.
An important general rule is that whenever possible the first step in assessment of ophthalmic trauma is to assess vision in each eye, preferably using a Snellen or other vision testing chart. It is important to bear in mind that the patient may have broken or lost glasses or contact lenses as a result of the trauma, such that pinhole testing to overcome refractive error may be important. Visual acuity less than counting fingers, not explained by refractive error or preexisting abnormality, is a strong indication of severe globe injury.
The periocular tissues are examined for any obvious abnormalities, particular attention being paid to eyelid wounds involving the margin or lacrimal canaliculi (Figure 19–1), both requiring management by an ophthalmologist, and proptosis, which may be due to orbital hemorrhage, air (orbital emphysema that characteristically causes crepitus) from a paranasal sinus fracture, infection (orbital cellulitis) including abscess formation, or carotid artery-cavernous sinus fistula.
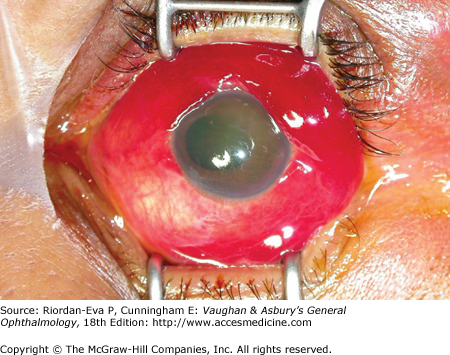
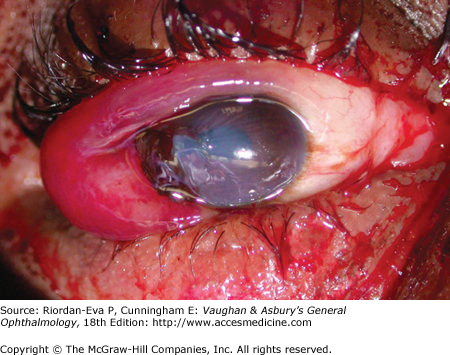
Figure 19-1.


Eyelid laceration with concurrent open globe injury. A: Rather innocuous-appearing V-shaped eyelid laceration involving the upper and lower lids and medial canthal skin. B: Total dark red hyphema and hemorrhagic chemosis are evident when the lids are separated. Note also that laceration extends through both lacrimal canaliculi.
The globes are then examined, including for subconjunctival hemorrhage, corneal, conjunctival, or scleral wound, corneal clarity, corneal foreign body, hyphema, and whether the eye is deformed due to low intraocular pressure suggestive of globe rupture. If there is eyelid swelling but no evidence of globe laceration or rupture, the eyelids may need to be gently separated avoiding pressure on the globes. Examination of the pupils is important, not least whether they can be clearly visualized or the view is impaired suggesting corneal or anterior segment damage. Abnormalities of pupil shape are important clues to severe globe injury, including corneal or corneo-scleral laceration (Figure 19–2), globe rupture, or severe blunt anterior segment trauma. A dilated unreactive pupil may be due to third nerve palsy when there has been head injury, and a relative afferent pupillary defect (RAPD) is an important sign of optic nerve damage. The latter is particularly relevant to assessment of unconscious patients with mid-facial trauma possibly resulting in optic nerve damage in the region of the optic canal, with or without associated fracture.

Assessment of ocular motility not only provides information about injury to the bony orbit, typically blow-out fracture of the floor or medial orbital wall, and orbital soft tissues, but also about intracranial damage, including skull base fracture resulting in sixth nerve palsy or more extensive limitation of eye movements due to carotid artery-cavernous sinus fistula, in which case there will also be proptosis and usually a bruit that can be heard by the patient as well as by listening with a stethoscope over the orbit or temple.
Ophthalmoscopy provides assessment of the clarity of the ocular media, which will be impaired by corneal damage, hyphema (anterior chamber hemorrhage), lens damage, or vitreous hemorrhage, the last being an important clue to scleral laceration or globe rupture. The fundi are examined for retinal or optic nerve abnormalities such as hemorrhages, retinal edema or detachment, and optic nerve avulsion—characteristically occurring after rapid rotation of the globe such as from a finger being forcibly poked into the eye, as well as choroidal rupture. Whether it is appropriate to dilate the pupils for fundal examination will depend upon what ocular damage has already been identified and the patient’s neurological status.
Slitlamp examination facilitates assessment of the anterior and posterior segments, as well as allowing measurement of intraocular pressure, although this can also be assessed by digital pressure, assuming that corneal or scleral laceration and globe rupture have been adequately excluded, or with the portable Perkins tonometer or Tonopen.
Partly because its superior 3-dimensional capabilities improve localization, orbital CT generally has superseded plain x-rays for suspected metallic intraocular or orbital foreign body, MRI being specifically contraindicated. CT can also detect some glass foreign bodies but it frequently fails to identify wooden foreign bodies, for which MRI or ultrasound is preferable and which commonly lead to orbital infection. CT has increasingly been used to detect globe rupture and is the preferred modality for identification of orbital fractures, although MRI may be preferable for the assessment of associated soft tissue changes, including infection, either orbital or intracranial.
In all cases of ophthalmic trauma, it is important to fully examine uninjured eyes, in part to ensure that there is no undiagnosed preexisting abnormality. In all cases of perforating ocular or periocular trauma, adequate tetanus immunization needs to be ensured.
First aid and emergency hospital treatment can make a vital contribution to improving outcome from ophthalmic trauma.
If there is a history of chemical injury from assault with alkali or acid or airbag injury; splashing of battery acid, cleaning solution, or chemicals either industrial or domestic; spraying of pesticide or chemical dust; or foreign bodies containing noxious substances, such as lime within cement or plaster; and initial examination shows no evidence of open globe injury, prior to any further assessment the ocular surface immediately should be copiously irrigated with tap water or, if available, sterile isotonic saline solution at the scene of the injury and in the emergency room. Administration of topical anesthetic drops and insertion of an eyelid speculum may be required to perform irrigation effectively and for removal of any retained foreign bodies. Identification of the relevant chemical is helpful. Alkalis continue to cause damage to the conjunctiva and cornea long after the injury is sustained, and thus irrigation of the eye should continue for a prolonged period (more than half an hour) in most such cases. In contrast, acids tend to form a barrier of precipitated necrotic tissue that limits penetration and deep tissue damage (as long as the offending chemical is washed away), such that irrigation need not continue for as long.
Corneal laceration may be obvious, or inferred from displacement of the pupil toward the wound, flat anterior chamber, hyphema, or uveal prolapse (Figure 19–2). Similar abnormalities, as well as hemorrhagic chemosis, softening and possible collapse of the eye, and vitreous hemorrhage, occur in scleral laceration, which should be particularly suspected if there is deep eyelid laceration (Figure 19–1), and globe rupture due to blunt ocular trauma (Figures 19–3 and 19–4). Whenever there is evidence or suspicion of open globe injury, the eye is protected with an eye shield, not least to prevent the patient from causing further injury by rubbing the eye and to alert other staff to the need to avoid manipulation of the eye. Analgesia and possibly antiemetic medication, to reduce the chance of vomiting, are administered.
A foreign body injury should be suspected whenever there is a history of explosion, gunshot wound, striking of metal upon metal, metal grinding, or a sharp object hitting the eye. If there is evidence or suspicion of a perforating ocular laceration (Figures 19–1 and 19–2), or signs of an orbital injury, CT orbits should be performed to identify and localize any foreign body unless one is already apparent (Figure 19–5). Ocular examination should identify any corneal foreign body or abrasion, if necessary aided by instillation of fluorescein (Figure 19–6). Particularly if there is curvilinear fluorescein staining of the superior cornea or persisting foreign body, the upper eyelid should be everted to identify any subtarsal foreign body (see Chapter 2).


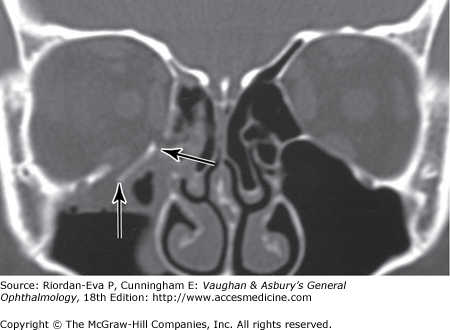
Enophthalmos, step defect on palpation of the orbital rim, massive orbital swelling, orbital crepitus, ocular motility defects, or profound visual impairment in the absence of direct ocular injuries consistent with that visual loss, should prompt CT orbits to detect rim, wall, or apex fractures (Figure 19–7), displaced bone fragments, air, hemorrhage, infection, or foreign bodies.
Categories of Ophthalmic Trauma
Mechanical ophthalmic trauma may be produced by objects that are blunt, sharp, or a combination of the two, and can be categorized into closed and open globe injuries, eyelid wounds, and orbital injuries, but these may co-exist, in which case coordination of management with maxillo-facial surgeons is important.
Corneal abrasion, which is one of the most common ophthalmic injuries encountered in an urgent care or emergency room setting, occurs when the corneal epithelium is disrupted, usually by a tangential impact such as from a fingernail or edge of a piece of paper. The patient typically complains of severe discomfort with foreign body sensation, profuse tearing, inability to keep the eyelids open, and impaired vision. If initial examination shows no obvious corneal laceration, topical anesthetic drops can be instilled, usually resulting in rapid reduction in discomfort and easier examination. Instillation of fluorescein highlights the corneal epithelial defect, which is usually in the inferior cornea, by staining the exposed basement membrane (Figure 19–6). If instead, there is curvilinear staining of the superior cornea, a subtarsal foreign body should be suspected (see later in the chapter).
Corneal abrasion is treated by instillation of an antibacterial ointment and patching of the eye. The patient is instructed to remove the patch, and apply antibacterial ointment and another patch, 2 to 4 times daily until the eye is comfortable. The patient can be reexamined periodically during the healing period to ensure that microbial infection has not developed, and certainly should be reexamined if symptoms do not settle within a few days or increase. Under no circumstance should topical anesthetic drops be provided or prescribed for the patient’s use, because they delay corneal epithelial healing, mask progression of disease, and if used for a prolonged period can cause a persistent neurotrophic corneal epithelial defect.
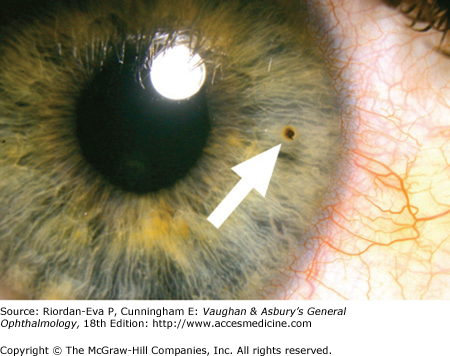
Corneal foreign body occurs when a small particle, usually with sharp rather than smooth edges, strikes the eye with insufficient momentum to cause it to pass completely through the cornea but sufficient for it become embedded within it. Alternatively, the particle may become embedded in the conjunctival surface of the upper eyelid (subtarsal foreign body). Symptoms are similar to those of a corneal abrasion, but usually not as severe and with predominance of foreign body sensation with eye opening and closing. Depending on its size, color, and transparency, metal being easier to detect than untinted glass, a corneal foreign body may be visible on diffuse flashlight examination of the ocular surface (Figure 19–8), but slitlamp examination is definitive. If examination is negative, the upper eyelid should be everted to detect any subtarsal foreign body (see Chapter 2), which usually can be removed by wiping the conjunctival surface with a sterile cotton bud, the only other required treatment being a single instillation of antibacterial ointment.
Emergency room staff trained in slitlamp examination can remove corneal foreign bodies, otherwise the patient should be referred to an ophthalmologist. The cornea should be anesthetized with topical anesthetic drops. Before attempting to remove a corneal foreign body, it must be confirmed by slitlamp examination that it is superficial and does not extend completely through the cornea, in which case removal should be performed by an ophthalmologist, generally in an operating room with an operating microscope so that tissue glue can be applied or sutures inserted if necessary. A superficial corneal foreign body can usually be removed at the slitlamp, using the tip of a sterile (18 or 21 gauge) needle. Iron or copper foreign bodies usually produce a ring of chemical tissue staining (“rust ring
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


