4 Many ophthalmic procedures today are safely performed under topical or local anesthesia to avoid the potentially adverse systemic consequences of general anesthetics. Topical anesthesia is rapidly growing in popularity for cataract surgery and minor anterior segment procedures; local anesthesia, including facial nerve blocks, peribulbar, subtenons, and retrobulbar blocks have become the routine for other general ophthalmic surgery. With the revolution of ambulatory surgery, many choices in ophthalmic anesthesia permit surgeons to develop their own versions of the ideal anesthetic techniques. Note: Several agents may be used for local and regional anesthesia. The following anesthetic agents and additives comprise a mixture that is among the most frequently used in ophthalmic surgery. Therefore, the final concentrations in the anesthetic mixture are lidocaine 1%, bupivacaine 0.375%, epinephrine 1:200,000, and hyaluronidase 7.5 units per ml. Figure 4.1 Figure 4.2 Figure 4.3
Ophthalmic Anesthesia
Local Anesthetic Agents
 Lidocaine 2%.
Lidocaine 2%.
 Onset of action: Approximately 5–10 minutes.
Onset of action: Approximately 5–10 minutes.
 Duration of action: Approximately 1–2 hours. Approximately 2–4 hours with epinephrine added.
Duration of action: Approximately 1–2 hours. Approximately 2–4 hours with epinephrine added.
 Bupivacaine 0.75%.
Bupivacaine 0.75%.
 Onset of action: Approximately 15–30 minutes.
Onset of action: Approximately 15–30 minutes.
 Duration of action: Approximately 5–10 hours.
Duration of action: Approximately 5–10 hours.
 Epinephrine 1:100,000.
Epinephrine 1:100,000.
 Minimizes systemic absorption of anesthetic agents.
Minimizes systemic absorption of anesthetic agents.
 Prolongs duration of action of anesthetic.
Prolongs duration of action of anesthetic.
 Minimizes bleeding (especially important in oculo-plastic procedures).
Minimizes bleeding (especially important in oculo-plastic procedures).
 Systemic sympathetic effects may be harmful.
Systemic sympathetic effects may be harmful.
 Epinephrine 1:100,000 is available premixed in either the lidocaine or bupivacaine solution.
Epinephrine 1:100,000 is available premixed in either the lidocaine or bupivacaine solution.
 Hyaluronidase.
Hyaluronidase.
 Enhances diffusion of anesthetic mixture through tissues.
Enhances diffusion of anesthetic mixture through tissues.
 Use 75 units per 10 ml of anesthetic solution. To prepare 10 ml of anesthetic solution, mix:
Use 75 units per 10 ml of anesthetic solution. To prepare 10 ml of anesthetic solution, mix:
 Lidocaine 2% with or without epinephrine 1:100,000 (5 ml).
Lidocaine 2% with or without epinephrine 1:100,000 (5 ml).
 Bupivacaine 0.75% (5 ml).
Bupivacaine 0.75% (5 ml).
 Hyaluronidase (75 units).
Hyaluronidase (75 units).
Facial Nerve (Orbicularis/Lid) Block
General Technique
 Use 25G, 1.5 inch disposable needle.
Use 25G, 1.5 inch disposable needle.
 Raise a small intradermal wheal of anesthesia at the entry site to make subsequent needle manipulations less painful.
Raise a small intradermal wheal of anesthesia at the entry site to make subsequent needle manipulations less painful.
 Direction of needle may be changed without removing it from skin.
Direction of needle may be changed without removing it from skin.
 Withdraw needle until just the tip penetrates the skin.
Withdraw needle until just the tip penetrates the skin.
 Rotate needle about its tip.
Rotate needle about its tip.
 Advance needle in the new direction.
Advance needle in the new direction.
 Always aspirate syringe before injecting anesthetic to prevent inadvertent intravascular administration.
Always aspirate syringe before injecting anesthetic to prevent inadvertent intravascular administration.
 Use a total of 3–5 ml of solution.
Use a total of 3–5 ml of solution.
 Inject anesthesia slowly.
Inject anesthesia slowly.
 Apply pressure over the injected area to facilitate effect of anesthetic on the motor nerves and to minimize hemorrhage.
Apply pressure over the injected area to facilitate effect of anesthetic on the motor nerves and to minimize hemorrhage.
Classic Van Lint Technique (Fig. 4.1)
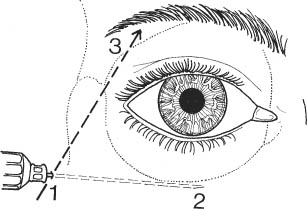
 Introduce the needle 1 cm behind the lateral margin of the orbit at the level of the inferior orbital rim.
Introduce the needle 1 cm behind the lateral margin of the orbit at the level of the inferior orbital rim.
 Raise a small wheal of anesthetic at the entry site.
Raise a small wheal of anesthetic at the entry site.
 Advance the needle as far as bone and inject ~0.5 ml of anesthetic.
Advance the needle as far as bone and inject ~0.5 ml of anesthetic.
 Advance needle horizontally and inject 1–2 ml subcutaneously along inferotemporal orbital rim while withdrawing needle.
Advance needle horizontally and inject 1–2 ml subcutaneously along inferotemporal orbital rim while withdrawing needle.
 Similarly, advance needle superonasally and inject along the superotemporal orbital rim.
Similarly, advance needle superonasally and inject along the superotemporal orbital rim.
Modified Van Lint Technique (Fig. 4.2)
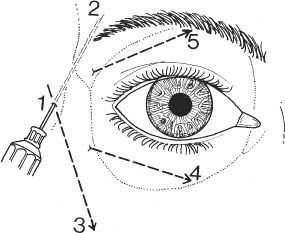
 Avoids excessive lid swelling.
Avoids excessive lid swelling.
 Introduce needle ~1 cm from lateral canthus.
Introduce needle ~1 cm from lateral canthus.
 Raise a small wheal of anesthetic at the entry site.
Raise a small wheal of anesthetic at the entry site.
 Advance needle in the subcutaneous space superiorly and slightly anteriorly and inject 1–2 ml while withdrawing needle. Do not remove needle from skin.
Advance needle in the subcutaneous space superiorly and slightly anteriorly and inject 1–2 ml while withdrawing needle. Do not remove needle from skin.
 Similarly, advance needle inferiorly and slightly anteriorly and inject anesthetic.
Similarly, advance needle inferiorly and slightly anteriorly and inject anesthetic.
 Remove needle from skin.
Remove needle from skin.
 Optional: Supplement anesthesia with horizontal injections along the orbital rims.
Optional: Supplement anesthesia with horizontal injections along the orbital rims.
 Enter skin ~1 cm inferonasal to original entry site, advance needle along inferior orbital rim, and inject the 1–2 ml subcutaneously while withdrawing needle. (Bending needle to a 30 degree angle may facilitate placement.)
Enter skin ~1 cm inferonasal to original entry site, advance needle along inferior orbital rim, and inject the 1–2 ml subcutaneously while withdrawing needle. (Bending needle to a 30 degree angle may facilitate placement.)
 Similarly, enter skin ~1 cm superotemporal to original entry site, advance needle along superior orbital rim, and inject anesthetic.
Similarly, enter skin ~1 cm superotemporal to original entry site, advance needle along superior orbital rim, and inject anesthetic.
O’Brien Technique (Fig. 4.3)
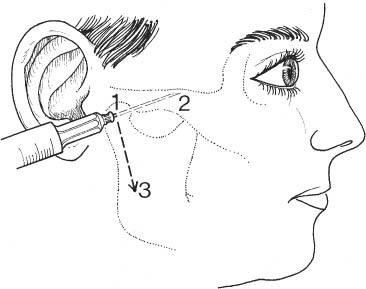
 Identify condyloid process of mandible.
Identify condyloid process of mandible.
 Located ~1 cm anterior to the tragus of the ear and inferior to the posterior aspect of the zygomatic process.
Located ~1 cm anterior to the tragus of the ear and inferior to the posterior aspect of the zygomatic process.
 May facilitate identification of condyloid process by feeling its movement at the temporomandibular joint as patient opens mouth and moves jaw from side to side.
May facilitate identification of condyloid process by feeling its movement at the temporomandibular joint as patient opens mouth and moves jaw from side to side.
 Insert needle until the periosteum of the condyloid process is reached.
Insert needle until the periosteum of the condyloid process is reached.
 Inject ~2 ml of anesthetic solution.
Inject ~2 ml of anesthetic solution.
 Do not inject into periosteum.
Do not inject into periosteum.
 Do not inject into temporomandibular joint space.
Do not inject into temporomandibular joint space.
 Withdraw needle to its tip and then advance it superiorly and anteriorly over zygomatic arch.
Withdraw needle to its tip and then advance it superiorly and anteriorly over zygomatic arch.
 Inject anesthetic solution as needle is withdrawn.
Inject anesthetic solution as needle is withdrawn.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


