Chapter 44 Operations for Vascular Compressive Syndromes
In recent years, microvascular decompression (MVD) has become the operative treatment of choice for many disorders of the cranial nerves, augmenting and replacing ablative procedures. These cranial rhizopathies have long defied categorization, clarification of pathophysiology, and definitive treatment despite efforts by clinicians in several disciplines. Although the clinical presentations of disorders such as trigeminal neuralgia, hemifacial spasm, glossopharyngeal neuralgia, tinnitus, spasmodic torticollis, disabling positional vertigo, and Meniere’s disease are quite different, these problems all share a common underlying pathology: vascular compression of the respective cranial nerve in the proximal nonfascicular region. Several studies have shown improved blood pressure control in medically refractory, severely hypertensive patients after MVD of the left lateral medulla oblongata.1,2
Beginning in 1966, a patient with trigeminal neuralgia was noted at operation to have compression of the trigeminal nerve by a small artery near the brainstem.3 The same year, a patient with hemifacial spasm was cured after coagulation of a vein that was distorting the facial nerve at the brainstem. As we performed operations to relieve vascular compression of the trigeminal and facial nerves, it became apparent that pulsatile, mechanical forces from a blood vessel were the pathophysiologic mechanism responsible for these cranial hyperactive syndromes. These syndromes later included glossopharyngeal neuralgia, tinnitus, and vertigo. All the cranial nerves are subject to the forces of vascular compression with arteriosclerosis, elongation, and brain sag as operant factors. This chapter describes the patient selection criteria, operative technique, perioperative management, results, and complications after more than 8000 MVDs for the aforementioned cranial rhizopathies.
PREOPERATIVE EVALUATION
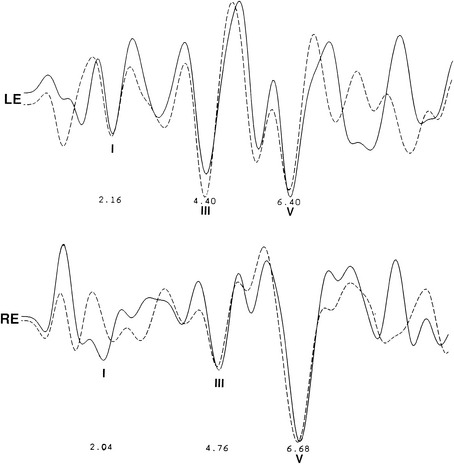
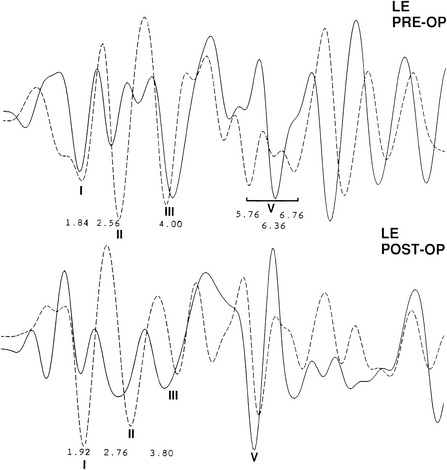
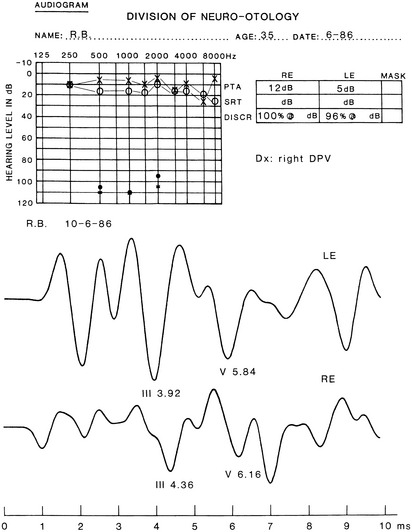
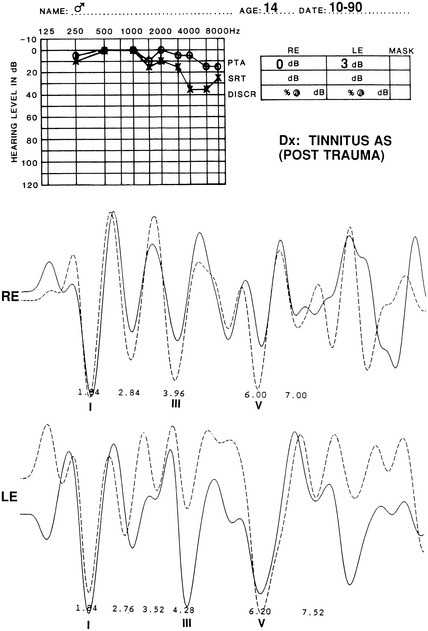
The audiometric tests are performed preoperatively to obtain a baseline for quantitatively determining deteriorations or improvement in hearing function. The pure tone audiogram often shows anomalies represented by small dips in the frequency range of 1500 to 2000 Hz.4 Additionally, preoperative BAEPs provide baseline information for the clinical neurophysiology team so that they may warn the surgeon of any deviations during monitoring of the intraoperative auditory evoked potentials. Typical changes observed in the BAEP are an increased interpeak latency between peaks I and III ipsilaterally or prolongation of interpeak latency between III and V contralaterally (Figs. 44-1 to 44-4). These findings are based on our knowledge of the neural generators of BAEPs.5–8
TRIGEMINAL NEURALGIA
Patient Selection
Patients with trigeminal neuralgia refractory to medical management are selected for MVD on the basis of their symptoms, history, and ability to undergo a general anesthetic. Patients with contraindications to general anesthetics or intracranial procedures may be treated with ablation procedures, including percutaneous glycerol rhizotomy, percutaneous radiofrequency rhizotomy, trigeminal balloon microcompression, stereotactic radiosurgery, and peripheral neurectomy.9,10 A discussion of these other surgical techniques is imperative for understanding why surgeons in many centers consider MVD to be the operative procedure of choice for most patients.
Peripheral neurectomy, although less invasive, typically has a short duration of tic relief, and may be indicated for patients with a shortened life expectancy.11 Radiofrequency lesions, created by percutaneous passage of a needle into the gasserian ganglion, have an initial success rate of 90% or greater, with long-term pain relief ranging from 20% to 78% of patients.12–15 Approximately 20% of patients have facial dysesthesias after radiofrequency rhizotomy. The greater the sensory loss, the more likely the trigeminal neuralgia will be relieved, but it is also more likely that dysesthesias leading to frank anesthesia dolorosa will supervene. Percutaneous glycerol rhizotomy rarely causes facial dysesthesias or sensory loss when performed strictly according to the technique introduced by Hakanson in 1981.16 Although glycerol rhizotomies have initial success rates of 80% to 90%,17 median time to recurrence varies from 16 to 36 months.18–21 Balloon microcompression of the trigeminal ganglion has initial pain relief ranging from 78% to 100%,17,22 with mean time to recurrence of 3.5 years.23 Minor dysesthesias occur in approximately 20% of patients,23 and mild temporary masseter weakness is seen in most patients treated with balloon microcompression.22 The corneal reflex is usually present.
Patients who have undergone radiofrequency lesions and balloon compression are initially satisfied because the trigeminal neuralgia is gone, but the side effects of numbness gradually become bothersome. In large series, new or worsening numbness or paresthesias after stereotactic radiosurgery (i.e., Gamma Knife) for trigeminal neuralgia occurred in 10%,24 10%,25 and 19%26 of patients, and complete pain relief (without medication) was achieved in 40% (2-year median follow-up),24 48% (1-year follow-up),25 and 34% (3-year follow-up).26 Median time to response (achievement of at least 50% pain relief) after stereotactic radiosurgery was 60 days,24 10 days,25 and 24 days.26 In another series of patients undergoing repeat stereotactic radiosurgery for trigeminal neuralgia, the authors concluded that most patients (85%) achieved more than 50% pain relief. New or worsening paresthesias occurred in 13% of patients, however, and complete pain relief (without medication) was achieved in only 19% of patients.27
The choice between MVD and other procedures should be governed by patient preference and ability to tolerate a craniotomy under general anesthesia. Advantages of MVD include consistently higher long-term success rates with a minimal chance of facial sensory loss or dysesthesias. These advantages are quite substantial in that the average life expectancy of the patients treated by the authors was 32 years from the initial onset of symptoms.28
The classic symptom of typical trigeminal neuralgia is lancinating pain in one or more distributions of the trigeminal nerve. Talking, eating, shaving, and feeling the wind blowing often precipitate symptoms. Patients typically have an abrupt and memorable onset of symptoms, with a variable duration of remission. A burning, aching pain without specific trigger points characterizes atypical trigeminal neuralgia,29 in contrast to typical trigeminal neuralgia. Although surgical success with these patients is less than with patients with typical symptoms, no other reasonable alternative treatments currently exist. Many patients have initial success with medical management using agents such carbamazepine, phenytoin, baclofen, valproic acid, clonazepam, and gabapentin. Carbamazepine historically has been most effective, but only 56% of patients maintain satisfactory pain relief after 10 years.30 Often, side effects, allergies, and the development of refractory symptoms to medications necessitate the need for early surgical intervention.
Operative Technique for Microvascular Trigeminal Decompression
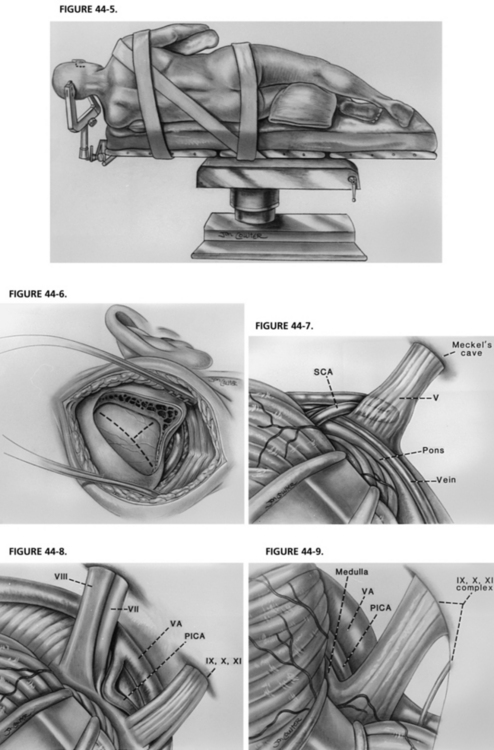
As in any operation, patient positioning is important. The patient is placed on the operating table with the head at the foot of the bed, providing maximal room for the surgeon during the microscopic portion of the case. A three-point head holder is applied and the patient is placed in the lateral decubitus position. An axillary roll and padding to other pressure points are placed. The neck is minimally put on stretch and slightly flexed, always maintaining at least two fingerbreadths between the patient’s chin and sternum. The patient is secured to the bed using straps and adhesive tape across the hips. The head holder is fastened into position. The patient’s shoulder is taped caudally for maximal working room (Fig. 44-5).31,32
After satisfactory positioning, a 2 cm strip of hair behind the ear is shaved and prepared. The incision, approximately 3 to 5 cm long (longer in a large man, shorter in a small woman), is placed 0.5 cm posterior to the hairline, extending one fourth above the iniomeatal line and three fourths below.31,32 Electrocautery is used to dissect and clear soft tissue until the mastoid eminence is adequately visualized.
Before beginning the craniectomy, the digastric groove should be visualized (5 cm behind the ear canal [4 cm in women] and 1 cm caudal to the lateral canthus, external ear canal line). The mastoid emissary vein, which is a good landmark for the junction between the sigmoid and transverse sinuses, may bleed. It should be waxed. The craniectomy is expanded until the junction of the transverse and sigmoid sinuses is definitively appreciated, with the apex of the triangular craniectomy pointed at this junction (variations are discussed with other cranial nerve syndromes) (Fig. 44-6). All air cells are waxed diligently, after which a curvilinear or T-shaped durotomy is performed, exposing a direct corridor along the petrotentorial bone down to the brainstem.31,32
When the dura is sutured back, the operating microscope is used to “turn the corner,” or expose the cerebellopontine angle. While gently retracting on the cerebellum with a Cottonoid on a sterile piece of latex (rubber dam), the surgeon must allow adequate cerebrospinal fluid to drain so that the cerebellum falls away, minimizing the need for much cerebellar retraction. Penetration of the trigeminal cistern and sharp dissection of arachnoid adhesions greatly reduce the need for significant cerebellar retraction medially. The Cottonoid and a precisely flexible, self-retaining brain retractor are placed on the supralateral portion of the cerebellum for trigeminal exposures. The cerebellum is retracted up and medially. Often, the first vessels encountered are the petrosal vein complex, which are coagulated and divided after evaluating relationships to the nerve.31,32
Before performing MVD of the trigeminal nerve, the surgeon must be aware that the dorsal root exit zone of the trigeminal nerve (the junctional area of myelin) extends to the distal portion of the nerve. The nerve must be meticulously inspected from the brainstem to Meckel’s cave, and all offending vessels must be decompressed. When performing the actual decompression, all arachnoid over the nerve must be dissected away. Shredded polytef (Teflon®) felt is placed between the vessel and the nerve. The most frequent vessel found is the superior cerebellar artery. Often multiple pieces of shredded Teflon felt are used to decompress looping arteries affecting more than one side of the trigeminal nerve.31,32
Results for Trigeminal Microvascular Decompression
The most frequent operative finding was trigeminal compression by the superior cerebellar artery in 76% of the patients (Fig. 44-7). Veins were causing neural compression in 68% of patients, but were the sole offending vessel in only 13%.38,39 In a report38 of 1204 patients who underwent initial MVD, 80% were pain-free at 1 year, and an additional 8% had greater than 75% relief, for a total success rate of 88%.38 At 10 years, 70% remained pain-free, and 4% had greater than 75% relief. Persistent mild postoperative facial numbness was noted in 17%, of which only 1% was severe. Repeat MVD was performed in 11% of patients for persistent or recurrent pain.38 Of these, 96% were pain-free or had greater than 75% pain relief 1 year after surgery (89% at 10 years).
MVD for pediatric-onset trigeminal neuralgia has a lower success rate than MVD for adults. At the time of discharge, 73% of patients had complete pain relief, with an additional 18% having greater than 75% diminution of pain.40 At last follow-up (mean 105 months), 57% of patients had either complete pain relief or greater than 75% relief of pain. The lower therapeutic response is likely due to the fact that the pathophysiology of the disease is different in pediatric patients. Venous compression was noted in 86% of the cases and was the sole offending vessel in 48%; this is markedly greater than for the adult patients. Additionally, venous compression often results in recurrence of pain because of revascularization. In 393 cases of trigeminal neuralgia caused by veins, 31% developed recurrence (most within 1 year of initial operation) after initial improvement of pain.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


