Odontogenic Cysts, Tumors, and Related Jaw Lesions
William L. Chung
Kurt F. Summersgill
Mark W. Ochs
The term odontogenic implies being derived from tooth-forming structures. Odontogenic cysts and tumors are a unique group of lesions due to their complex and variable history, histologic characteristics, and clinical behavior. Odontogenic cysts vary significantly in their frequency, behavior, and treatment. Odontogenic tumors are relatively uncommon lesions (1). Collectively, lesions of the jaws deserve considerable attention by surgeons because of their potential for tissue destruction and the related challenges they pose for reconstruction. This chapter reviews the more common odontogenic cysts and tumors along with several other related jaw lesions. The salient clinical, radiographic, and histologic features of each lesion will be discussed, in addition to its treatment and prognosis. Many of the odontogenic cysts and tumors share similar radiographic features, so the patient’s history and eventual histopathology ultimately dictate the specific surgical therapy. Furthermore, a frozen section is not typically obtained for jaw lesions discussed in this chapter because they are not malignant lesions and a frozen section will not change the ultimate treatment plan for each lesion.
ODONTOGENIC CYSTS
In 1992, the World Health Organization (WHO) classified odontogenic cysts as either inflammatory or developmental, including odontogenic and nonodontogenic. Most cysts of the oral cavity are true cysts because they contain an epithelial lining. The lining of these cysts is derived from one of three epithelial structures: (a) reduced enamel epithelium —residual epithelium that surrounds the crown of the tooth after enamel formation is complete; (b) rests of Malassez—remnants of the Hertwig root sheath that persist in the periodontal ligament after root formation is complete; or (c) remnants of dental lamina (rests of Serres)— islands and strands of epithelium that originate from the oral epithelium and remain in tissues after inducing tooth development (2). Odontogenic cysts can become inflamed or infected, causing significant signs or symptoms.
INFLAMMATORY CYSTS
Radicular Cyst
The radicular cyst is by far the most common odontogenic cyst. It develops at the apex of an erupted tooth in response to pulpal necrosis secondary to dental caries or trauma. The cyst arises from inflammatory stimulation and proliferation of the rests of Malassez. The cyst lining forms as the epithelial elements proliferate. Cellular debris within the lumen produces an osmotic gradient, and fluid is transported across the lining. This gradient slowly increases the volume of fluid inside the lumen, ultimately expanding the cyst by hydraulic pressure from within the cyst.
Clinical and Radiographic Features
Most radicular cysts are asymptomatic and are discovered incidentally during routine radiographic evaluation (Fig. 132.1). Radicular cysts rarely exceed 1 cm in diameter except when several adjacent teeth become devitalized as a result of trauma. Radiographically, the radicular cyst is round to ovoid, well circumscribed, and contiguous with the apex of the involved tooth.
Histopathology
The cyst is lined by stratified squamous epithelium of varying thickness. The cyst wall typically supports a variable inflammatory cell infiltrate, including lymphocytes and neutrophils. The cystic lumen will frequently contain necrotic cellular debris. A small percentage of radicular cysts have crescent-shaped hyaline (Rushton) bodies within the epithelial lining. Although unique to odontogenic cysts, the biologic significance of Rushton bodies is unknown. Multinucleated foreign body giant cells, cholesterol crystal clefts, and hemosiderin may be seen throughout the connective tissue of the cyst wall.
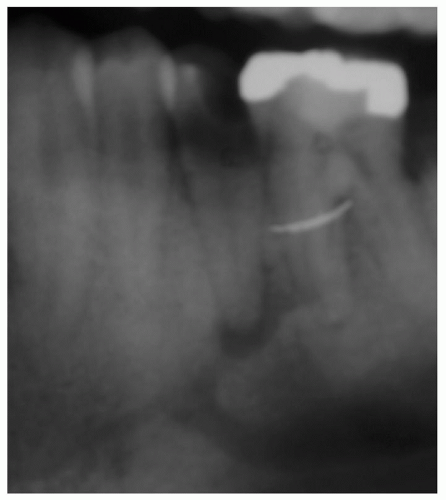 Figure 132.1 Periapical cyst. Radiograph demonstrating periapical lesion associated with grossly carious tooth # 20. |
Treatment and Prognosis
These cysts are treated by extraction of the infected tooth followed by enucleation of the cyst. Extraction of the tooth without removing the cyst may allow for persistent growth of the cyst. If the cyst is incompletely removed, a residual cyst may develop. Complete bony healing is typically seen within 6 months if the radicular cyst has been thoroughly removed.
DEVELOPMENTAL CYSTS
Dentigerous Cyst
The dentigerous cyst is the second most common odontogenic cyst. A dentigerous cyst must be associated with the crown of an unerupted tooth (3). The cyst is attached to the cervical region of the tooth, usually a mandibular third molar. However, variants exist where the cyst is seen lateral to or completely enveloping the associated tooth. Maxillary third molars, maxillary canines, and mandibular second bicuspids are also commonly involved, as these teeth are among those frequently impacted.
Clinical and Radiographic Features
Dentigerous cysts usually occur in the second and third decades with a slight male predilection. Because they are associated with an impacted tooth, the arch will appear to be missing a tooth. The cysts usually do not produce symptoms and can achieve significant size, causing bony expansion (Fig. 132.2A and B). The dentigerous cyst is usually a well-circumscribed, unilocular, radiolucency surrounding the crown of an unerupted tooth (Fig. 132.2C). Mandibular cysts can displace the tooth into the ramus or the inferior border of the mandible, while maxillary cysts can displace the tooth into the maxillary sinus toward the orbital floor. It is important to understand that the above-stated clinical and radiographic features are not specifically diagnostic
for a dentigerous cyst, although highly consistent (4). The differential diagnosis for similar-appearing radiographic lesions should include an ameloblastoma, keratocystic odontogenic tumor (KCOT), and adenomatoid odontogenic tumor (AOT).
for a dentigerous cyst, although highly consistent (4). The differential diagnosis for similar-appearing radiographic lesions should include an ameloblastoma, keratocystic odontogenic tumor (KCOT), and adenomatoid odontogenic tumor (AOT).
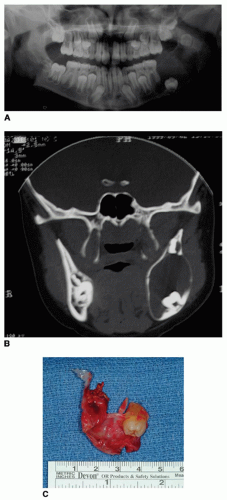 Figure 132.2 A,B: Dentigerous cyst. Panorex radiograph and computed tomography (CT) scan of 14-year-old who presented with facial swelling. Radiograph reveals considerable left mandibular angle and ramal involvement. Note thinning of buccal and lingual cortices and displacement of multiple permanent teeth within lesion on CT. C: Surgical specimen from above patient. Note adherence of cyst to permanent tooth crown. |
Histopathology
The cystic lumen is lined by nonkeratinized, stratified squamous epithelium that is anywhere from 2 to 10 cell layers thick. It is common for the lining to be inflamed. The dentigerous cyst can share several microscopic features with the radicular cyst, such as Rushton bodies, cholesterol crystal clefts, and hemosiderin deposits. Chronic dentigerous cysts may exhibit areas of keratinized epithelium, which require the lesion to be differentiated from the KCOT (5). The epithelial lining of the dentigerous cyst is capable of ameloblastoma expression (3). Thus, timely diagnosis and treatment is critical.
Treatment and Prognosis
Removal of the impacted tooth along with thorough enucleation of the cyst is usually definitive therapy. When a mandibular dentigerous cyst reaches considerable size, the cyst can be marsupialized to allow for decompression and shrinkage of the cyst with compensatory bone fill prior to definitive removal of the lesion.
Calcifying Odontogenic Cyst (Gorlin Cyst)
This lesion is thought to arise from remnants of the dental lamina within the gingiva or jaws. Approximately onefourth of all calcifying odontogenic cysts (COCs) occur extraosseously, within the gingiva anterior to the first molar in individuals older than 50 years (6).
Clinical and Radiographic Features
The COC behaves like most other odontogenic cysts, and it has little recurrence potential. The COC has a wide age range, but the peak incidence occurs in the second decade. The lesion has a predilection for females, and most are located in the anterior portion of either jaw. The extraosseous lesion may present with painless gingival expansion. These cysts are often discovered as incidental findings on routine radiographic evaluation. They initially appear lucent. As the cyst develops, calcifications may develop causing a well-circumscribed mixed radiolucent/radiopaque appearance. However, these opacities are only seen in approximately one-third to one-half of all cases.
Histopathology
These usually unilocular cysts are lined by odontogenic epithelium. The basal layer is distinct with its columnar to cuboidal cells with hyperchromatic nuclei that are polarized away from the basement membrane (Fig. 132.3). Another characteristic histologic feature of the COC is the ghost cell—an altered epithelial cell with loss of the nucleus and bright eosinophilic cytoplasm—that represents abnormal keratinization. With time, these ghost cells tend to become calcified, sometimes even forming calcified masses. When these cells contact the connective tissue, a foreign body reaction occurs due to the release of keratin.
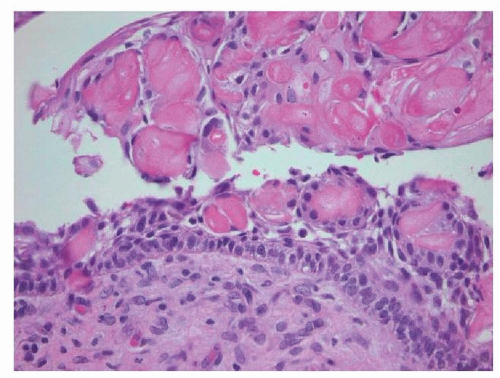 Figure 132.3 Calcifying odontogenic cyst (Gorlin cyst). Cyst lined by odontogenic epithelium. The basal cells are palisaded and columnar. Large, eosinophilic “ghost cells” are seen within and on the surface of the epithelium. |
Treatment and Prognosis
Surgical enucleation usually results in complete resolution. The extraosseous lesions are often associated with other odontogenic tumors and due to their low recurrence potential are managed conservatively with lesion removal only.
Glandular Odontogenic Cyst (Sialo-Odontogenic Cyst)
The glandular odontogenic cyst was first described in 1987 (7). Although only a few cases have been reported, it is worth mentioning due to its locally aggressive behavior and its propensity to recur. This lesion is generally considered odontogenic in origin with numerous mucus-secreting cells within its epithelial lining.
Clinical and Radiographic Features
This lesion occurs most commonly in middle-aged adults. The majority of glandular odontogenic cysts have been reported in the mandible especially in the anterior region. They appear as multilocular radiolucencies and may cross the midline.
Histopathology
This lesion has several unique microscopic features: (a) an epithelial lining of variable thickness and a flat epithelial-connective tissue junction; (b) small microcysts and glandlike structures within the epithelial lining; and (c) a single layer of cuboidal or columnar cells lining the gland-like structures (Fig. 132.4).
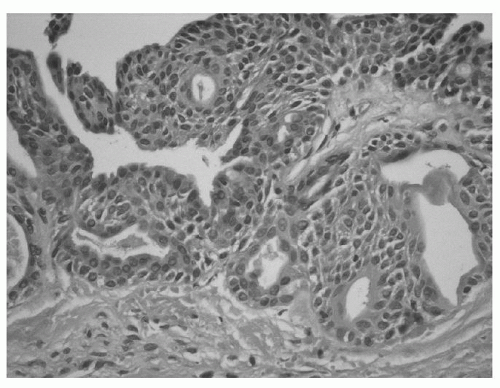 Figure 132.4 Glandular odontogenic cyst. Stratified squamous epithelium forming gland-like structures. |
Treatment and Prognosis
Most glandular odontogenic cysts are amenable to enucleation and curettage. However, due to its recurrence potential, some advocate marginal resection (8). Regardless, long-term follow-up is advisable.
NONODONTOGENIC CYSTS
Nasopalatine Duct Cyst (Incisive Canal Cyst)
The nasopalatine duct cyst originates from the epithelial remnants of the two embryonic nasopalatine ducts (9). The majority of these cysts arise in the anterior maxilla near the incisive foramen.
Clinical and Radiographic Features
Men are affected twice as often as females, and this cyst occurs most frequently in the fourth to sixth decades. The nasopalatine duct cyst is either asymptomatic or presents as a soft tissue swelling in the midline of the anterior hard palate once the lesion has perforated the bone. The lesion is typically a well-circumscribed, oval-pear or heart-shaped, unilocular radiolucency in the midline of the anterior palate. If the cyst reaches large proportions, it can resorb the roots of the adjacent teeth. Some normal incisive canals are radiographically wide, which may make diagnosis of this lesion less precise. It is generally accepted that any radiographic lesion greater than 6 mm should be considered a cyst and not an enlarged incisive foramen. If no soft tissue or bony swellings are present and the patient is asymptomatic, then a diagnosis of nasopalatine duct cyst becomes unlikely.
Histopathology
The lining of this lesion can be either stratified squamous epithelium, ciliated columnar or cuboidal epithelium, or a combination of the two. This variable lining reflects whether the cyst has arrived from epithelium closer to the palate (stratified squamous) or more closely associated with the nasal cavity (ciliated columnar). The fibrous tissue contains elements of nerve and vascular tissue consistent with the surrounding incisive canal contents. Mucus glands are occasionally seen within the wall of the cyst as these glands are native to the adjacent nasal cavity.
Treatment and Prognosis
Surgical enucleation is usually curative, but may result in sacrificing the nasopalatine nerve and vessel, resulting in denervation of the mucosa of the anterior palate and maxillary incisors. Recurrence is rare.
Stafne Bone Cyst (Lingual Salivary Gland Depression, Static Bone Cyst)
The Stafne bone cyst is not a true cyst. Rather, it is a depression on the lingual aspect of the posterior body of the mandible. This condition has a pathognomonic radiographic appearance of a small ovoid, well-circumscribed radiolucency often surrounded by cortical bone, located below the inferior alveolar canal in the second or third molar region. This radiographic appearance is due to the relative thinning of the mandible. Most reported cases have occurred in males. Sialography, biopsy, and autopsy have revealed that the depression is characteristically filled with an accessory lateral lobe of the submandibular salivary gland, although occasionally connective tissue, adipose tissue, and lymphoid tissue have been seen (10). No treatment is required.
Idiopathic Bone Cavity (Traumatic Bone Cyst or Traumatic Bone Cavity)
The traumatic bone cavity is not a true cyst because it does not contain a true epithelial lining. It is usually found in the posterior mandible and presents on radiograph as a less well-defined radiolucency compared to most odontogenic cysts. These lesions are typically empty on surgical exploration or contain some straw-colored fluid. There is no lining or tissue to submit for biopsy, but exploration of the lesion will be curative, since hemorrhage within the cavity will allow for granulation tissue formation and ultimate resolution of this condition.
ODONTOGENIC TUMORS
Odontogenic tumors are collectively a rare but diverse and complicated group of lesions. They arise from epithelial or mesenchymal cells, or both, that are associated with tooth structures. Most odontogenic tumors are true neoplasms, but some behave as hamartomatous growths. Odontogenic tumors commonly present as asymptomatic swellings, which can eventually cause bone loss, tooth displacement, and jaw expansion. They rarely cause sensory nerve dysfunction. Understanding the biologic behavior of this group of lesions will assist in choosing the appropriate
treatment to best attain a cure or to optimize the outcome (11,12). The tumors discussed in this chapter were selected based upon their frequency, locally aggressive behavior, and/or likelihood of recurrence.
treatment to best attain a cure or to optimize the outcome (11,12). The tumors discussed in this chapter were selected based upon their frequency, locally aggressive behavior, and/or likelihood of recurrence.
Odontoma
Odontomas are not true neoplasms, but rather hamartomatous growths because they form during normal tooth development and then reach a fixed size. The lesion contains elements of enamel, dentin, cementum, and pulp tissue. Depending on the degree of morphologic differentiation, an odontoma can be classified as either compound, if the lesion resembles tooth-like structures or complex, if the lesion appears as an amorphous mass.
Clinical and Radiographic Features
The odontoma is the most common odontogenic “tumor.” The lesion is typically asymptomatic and is discovered in the first two decades on radiographic examination, often initiated to evaluate lack of expected eruption of a permanent tooth. Radiographically, both the compound and complex odontomas are radiopaque masses and have a well-demarcated border. The compound odontoma resembles multiple tiny tooth structures, while the complex odontoma appears as a dense irregular mass.
Histopathology
Although reduced enamel epithelium may be present, odontomas are essentially composed of enamel, dentin, cementum, and pulp tissue. Fibrous tissue is sparse.
Treatment and Prognosis
Removal of the lesion may be necessary to rule out other lesions or if the mass is impeding the eruption of a tooth. Enucleation and curettage is considered curative, and the lesion is not known to recur.
Keratocystic Odontogenic Tumor (Odontogenic Keratocyst)
The KCOT is a uni- or multicystic, intrabony lesion of odontogenic origin. It develops from remnants of the dental lamina and can occur in any location of the jaws (13,14). Its previous traditional term, odontogenic keratocyst (OKC), emphasized the benign behavior of this lesion. However, in 2005, the WHO Working Group recommended the newer term KCOT because it more accurately described its neoplastic behavior (15). These lesions mimic the radiographic appearance of any other odontogenic cyst and some odontogenic tumors. The mandibular ramus and posterior body are the most common locations for the KCOT (Fig. 132.5A and B). The KCOT in the maxilla typically favors the posterior or canine regions.
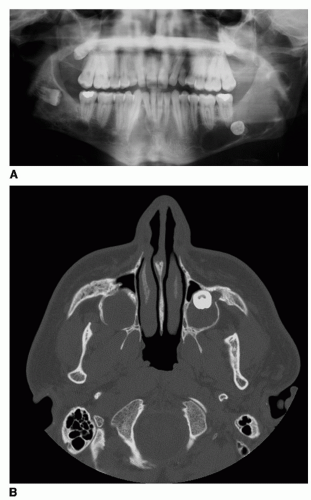 Figure 132.5 A: Keratocystic odontogenic tumor. Panoramic radiograph of a 18-year-old man with bilateral mandibular and maxillary KCOT. Patient also had NBCCS. B: Axial computed tomography (CT) scan of same patient, revealing bilateral maxillary lesions. Lesions were noted to extend to the orbital floors intraoperatively. |
Clinical and Radiographic Features
The KCOT differs from other odontogenic lesions with regard to its growth potential and recurrence rate. It can display aggressive growth, causing bony expansion and destruction, and reports have shown recurrence rates from 5% to 60% (16,17). The KCOT occurs over a wide age range; however, its peak incidence is within the second and third decades. When multiple KCOTs occur in a patient, the nevoid basal cell carcinoma syndrome (NBCCS) must be considered. The mean age of patients with multiple KCOTs, with or without NBCCS, is lower than those with single, nonrecurrent KCOTs. Radiographically, the KCOT appears as a well-circumscribed radiolucency with a distinct border, and many cause bony expansion or erosion of either cortex. Involved teeth may become displaced, but root resorption rarely occurs.
Histopathology
The KCOT has the following distinct microscopic appearance: its lining is parakeratinized, stratified squamous epithelium, which is six to eight cell layers thick; the luminal surface is covered by a corrugated layer of parakeratin; the basal layer is palisaded and cuboidal, with prominent, intensely stained hyperchromatic nuclei; and a lack of rete pegs. This flat epithelial-connective tissue interface results in a separation of the epithelium on histopathologic processing. Exfoliated parakeratin often fills the cyst lumen and presents during surgery as a creamy, white material. Daughter (satellite) epithelial islands and cysts may be seen in the surrounding connective tissue and may be indicative of the NBCCS.
Treatment and Prognosis
The KCOT requires surgical enucleation and osseous curettage, and every attempt should be made to remove it in one piece (18). Modified Carnoy solution is a tissue fixative that can aid in a more complete lesion removal. Treatment of the residual bony cavity may devitalize microscopic remnants, thus decreasing the chance of recurrence (19,20). Some clinicians have advocated marginal resection to avoid recurrence (21). When large lesions are present, marsupialization may be performed to decompress the KCOT to allow for easier removal of the cyst at a later surgery (22,23). Secondary infection, need for high patient compliance, and variable results limit the use of marsupialization techniques. Most recurrences occur within 5 years, but reports of recurrence as long as 10 years later have been documented. Thus, close follow-up is mandatory. Recurrence of KCOT has been speculated based on several theories: incomplete removal of the cyst due to its thin friable membrane and adherence to adjacent tissues, residual satellite cysts following enucleation, and remnants of dental lamina not associated with the KCOT in question causing de novo cyst formation. The orthokeratinized odontogenic cyst is considered by some to be a unique cyst, and by others to be a variant of the KCOT. It is much less common than the KCOT and has a much lower recurrence rate (24). Unlike the KCOT, the orthokeratinized odontogenic cyst is lined by orthokeratinized stratified squamous epithelium. There is a prominent granular layer below a noncorrugated surface, and the basal layer is less prominent.
Nevoid Basal Cell Carcinoma Syndrome (Basal Cell Nevus Syndrome, Gorlin Syndrome)
The NBCCS is an autosomal dominant inherited condition that exhibits high penetrance and variable expressivity (25,26




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
