Oculoplastic Considerations and Management of Facial Paralysis
Aaron Fay
Peter A.D. Rubin
CAUSES OF FACIAL NERVE DYSFUNCTION
Facial nerve dysfunction may result from infection, inflammation, neoplasm, accidental trauma, or surgery. Each may produce concomitant intraocular disease, which should be excluded in all cases. Ocular surface involvement, however, is closely related to severity and duration of the facial paralysis. Inflammatory conditions, which tend to improve over weeks to months, may be best treated medically and with reversible surgeries. Conversely, permanent facial paralysis resulting from facial nerve transection may require eyelid and lacrimal reconstruction and intensive replacement of aqueous tears. It is therefore imperative to investigate the viability of facial nerve rehabilitation at the time of injury or paralysis. In cases of surgical injury to the facial nerve, it is important to observe intraoperative clues of rehabilitation potential. Intraoperative or postoperative facial nerve stimulation may be of prognostic value in selected cases (Chapters 6, 7, and 35). This chapter will focus primarily on evaluation and treatment alternatives of periocular reconstruction in cases of surgical facial nerve injury.
PERTINENT OPHTHALMIC ANATOMY
Eyelids and Lacrimal Apparatus
An understanding of eyelid and periocular anatomy is essential in evaluating neurologic and myogenic eyelid function and lacrimal secretion (Fig. 39.1). Eyelid anatomy is commonly described in distinct anterior and posterior lamellae. The anterior lamella comprises the skin and pretarsal and preseptal components of the orbicularis oculi; the posterior lamella contains tarsus, the collagenous structural element of the eyelid, and the palpebral conjunctiva. Within the tarsus are meibomian glands, sebaceous glands whose ducts open along the posterior lid margin. Additional sebaceous glands (Zeis) are associated with individual cilia along the anterior lid margin. The anterior and posterior lamellae adjoin along the lid margin to form the visible gray line (Fig. 39.2).
Eyelid elevation and depression are coordinated through a complex neurologic loop that is the critical element in modern surgical approaches to eyelid paralysis (Fig. 39.3). Elevation is produced primarily by stimulation of the levator palpebrae superioris, which is innervated by the superior division of the oculomotor nerve. Eyelid elevation can also be achieved by adjunctive contracture of the ipsilateral frontalis, stimulated by the temporal branch of the facial nerve. Conversely, eyelid closure is produced exclusively by the orbicularis oculi, which is innervated by the temporal and zygomatic branches of the facial nerve. The orbital portion of the orbicularis is under voluntary control and produces forced eyelid closure (wink), whereas the palpebral components (pretarsal and preseptal) produce involuntary reflex closure (blink) (Fig. 39.4). Under physiologic conditions, reflex closure and baseline lacrimation protect the ocular surface from environmental pathogens, debris, and trauma. This spontaneous blinking occurs at a rate of approximately 20 to 30 blinks per minute and increases with age, whereas blink amplitudes range from 25 to 38 degrees and decrease with age. Both are age dependent. Additional reflex closure may be stimulated by bright light (light-blink reflex), exhaustion, photophobia (pain produced by bright light), or the corneal reflex.
Lacrimation is intimately related to eyelid function. The normal tear film comprises three layers: mucinous, aqueous, and lipid. The posterior mucinous layer derives from conjunctival goblet cells, whereas the anterior lipid layer is produced by meibomian glands. Greater than 98% of tear volume, however, is aqueous and derives from both primary and accessory lacrimal glands. Basal secretion is produced by the accessory lacrimal glands of Krause and Wolfring located within the eyelids and conjunctival fornices. The primary lacrimal gland is responsible for reflex tearing and receives autonomic innervation from parasympathetic fibers that travel first with the facial nerve and then with the maxillary division of the trigeminal nerve. Proper lacrimation provides eyelid lubrication and nutrients to the anterior corneal stroma and epithelium. Tears contain antimicrobial properties (IgA) and serve as the primary refracting surface for the visual system. Once tears are produced, proper eyelid tone and function are required for normal lacrimal drainage.
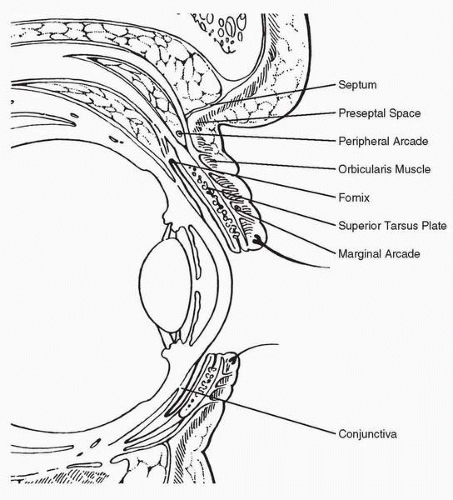 FIG. 39.1 Cross-sectional anatomy of the eyelids. (From Janfaza P, Nadol JB, Galla R, et al, eds. Surgical anatomy of the head and neck. Philadelphia: Lippincott Williams & Wilkins, 2001:169, with permission.) |
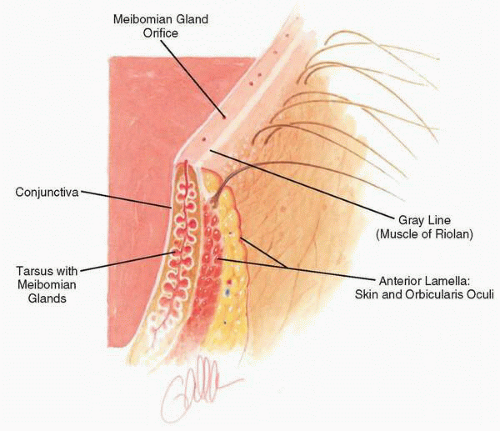 FIG. 39.2 Eyelid margin demonstrating distinct posterior and anterior lamellae with intervening gray line (muscle of Riolan). |
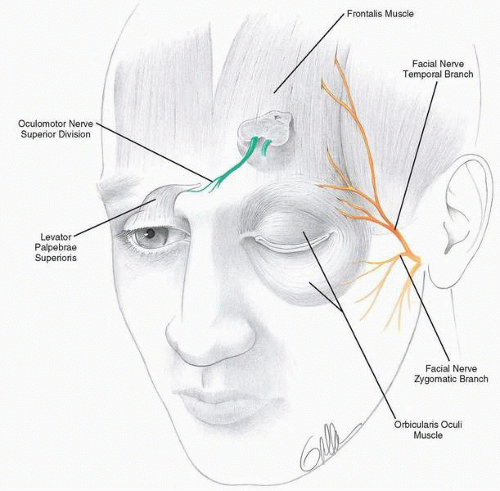 FIG. 39.3 Innervation of the primary eyelid elevators and depressors. The levator palpebrae superioris is innervated by the superior division of the oculomotor nerve, whereas the orbicularis oculi is innervated by the facial nerve. |
The tear pump is a physiologic mechanism that sweeps new tears across the ocular surface in a superotemporal to inferonasal direction and assists in drainage through the canaliculi and lacrimal sac. Although the precise mechanism has been debated, the medial heads of the orbicularis oculi (Horner’s muscle) encircle the lacrimal sac, producing rhythmic contracture of the sac and a pressure phenomenon that draws the tear lake into the lacrimal puncta while forcing tears into the nasolacrimal duct. Insufficient palpebral tone or function is a common cause of epiphora.
Lower eyelid tone and position rely on facial nerve integrity to mitigate gravitational forces. Orbicularis paresis therefore produces lower lid laxity and frank ectropion, as well as epiphora from lacrimal pump dysfunction. Paradoxically, entropion can also occur as the lax lower eyelid is dislodged from its native apposition to the globe and freely everts or inverts. Entropion produces foreign body sensation, superficial corneal injury, and secondary epiphora.
Cornea
The cornea is approximately 500 microns thick and comprises five distinct layers. The corneal epithelium is a single cell layer that derives its nutrition from the tear film. The epithelium
serves as a primary barrier to microbial infection. Deep to the epithelial basement membrane, Bowman’s layer is the anterior condensation of the corneal stroma. Bowman’s layer provides a barrier to neoplastic invasion. The corneal stroma consists of highly organized collagen lamellae and keratocytes with intervening terminal trigeminal nerve fibers. Descemet’s membrane is the basement membrane of the corneal endothelium, the posterior layer responsible for the continual dehydration that preserves corneal transparency. Corneal perforation produced by severe corneal drying or infection may lead to endophthalmitis and intraocular abscess formation (Fig. 39.5).
serves as a primary barrier to microbial infection. Deep to the epithelial basement membrane, Bowman’s layer is the anterior condensation of the corneal stroma. Bowman’s layer provides a barrier to neoplastic invasion. The corneal stroma consists of highly organized collagen lamellae and keratocytes with intervening terminal trigeminal nerve fibers. Descemet’s membrane is the basement membrane of the corneal endothelium, the posterior layer responsible for the continual dehydration that preserves corneal transparency. Corneal perforation produced by severe corneal drying or infection may lead to endophthalmitis and intraocular abscess formation (Fig. 39.5).
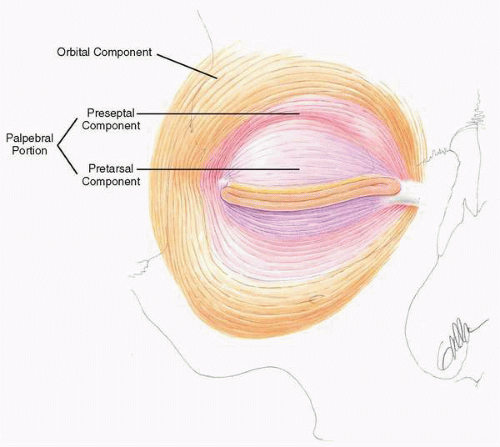 FIG. 39.4 The three segments of the orbicularis oculi. The involuntary blink is produced by the palpebral portions of the muscle, whereas the voluntary wink is produced by the orbital component. |
Corneal sensation is an important indicator of corneal epithelial vitality and may be critical in maintaining a suitable environment for ocular survival. Corneal sensation is carried by the nasociliary branch of the maxillary division of the trigeminal nerve. In addition to corneal sensation, these trigeminal fibers provide neurotrophic influence to the corneal epithelium. Denervated corneas with epithelial defects heal poorly and may develop neurotrophic ulcers, placing the eye at risk for bacterial infection, perforation, endophthalmitis, and blindness. Furthermore, denervated corneas are at increased risk of trauma due to loss of the corneal blink reflex. When compounded by incomplete eyelid closure, the cornea is extremely vulnerable. In the setting of corneal denervation, therefore, appropriate eyelid reconstruction is critical, usually requiring tarsorrhaphy.
Corneal exposure may be produced by limited upper eyelid excursion or by lower eyelid retraction. In either situation, pain, foreign body sensation, or tearing may be the initial symptom. Risk of infection is increased by mechanical and chemical deficiencies; perforation, endophthalmitis, and loss of the eye are possible.
OPHTHALMIC EXAMINATION
A full ophthalmic examination is desirable in cases of compromised eyelid or lacrimal function. Many patients, however, may not be ambulatory following head and neck surgery or head trauma. In these cases an abbreviated bedside consultation may suffice as a preliminary screening.
Visual acuity may be recorded as a Snellen equivalent using a near card. It is important to have the patient use his or her reading glasses or to provide an estimated reading spectacle correction in patients nearing presbyopia (+3.00 lenses usually suffice). Visual acuity in the range of 20/40 may be acceptable during bedside examination given the lack of proper lighting, rudimentary testing material, estimated spectacle correction, and likelihood of corneal surface abnormality. Lubricating or antibiotic ointments often
limit visual acuity testing in this setting. The pupils should be examined for relative afferent defects. Extraocular motility should be examined to exclude oculomotor, trochlear, and abducens nerve involvement. A cursory examination of cranial nerves V, VII, and VIII should be performed.
limit visual acuity testing in this setting. The pupils should be examined for relative afferent defects. Extraocular motility should be examined to exclude oculomotor, trochlear, and abducens nerve involvement. A cursory examination of cranial nerves V, VII, and VIII should be performed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


