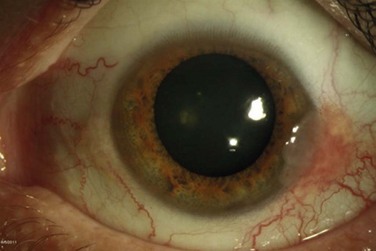
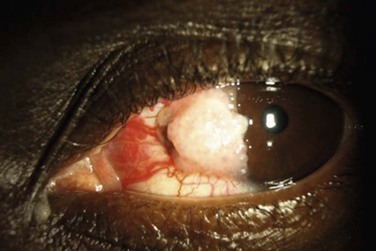
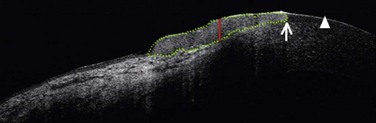
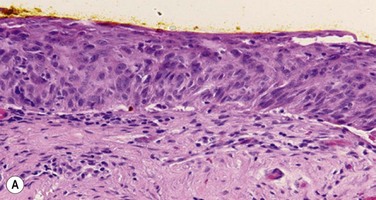
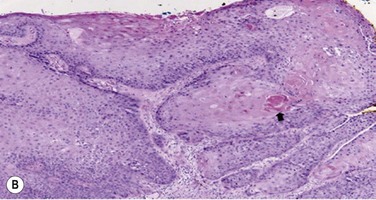
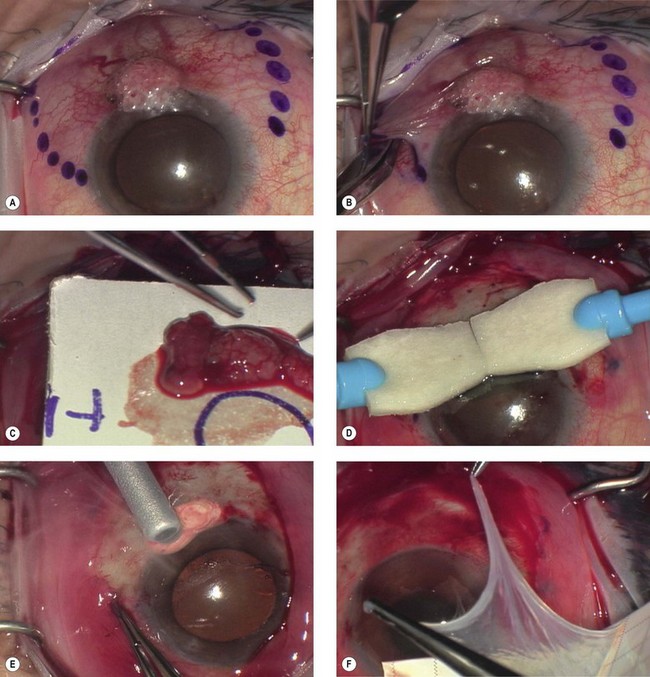
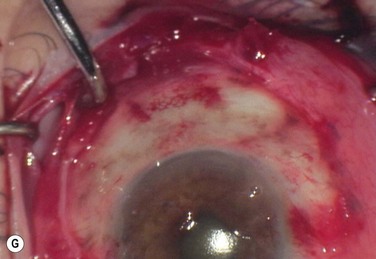
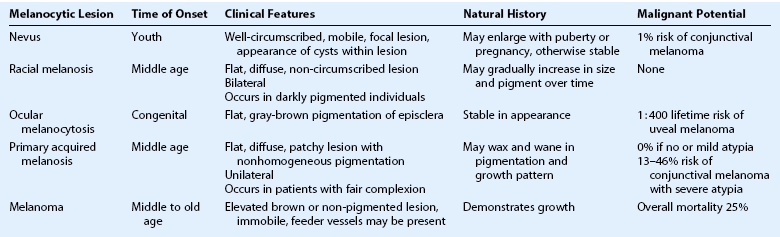
19 Ocular surface squamous neoplasia (OSSN) is an umbrella term used to describe cancerous epithelial lesions of the cornea and conjunctiva, ranging from dysplasia to carcinoma-in-situ to invasive squamous cell carcinoma.1 The term conjunctival and corneal epithelial neoplasia (CIN) describes varying degrees of dysplasia confined to the surface epithelium, and when it is full thickness is called carcinoma-in-situ. When invading the basement membrane, the term squamous cell carcinoma applies. Ocular surface squamous neoplasia (OSSN) has an estimated incidence in the United States of 0.03 per 100 000 persons.2 Higher incidences have been reported in other parts of the world with more sun exposure, with an estimated incidence of 1.9 per 100 000 persons in Australia3 and 3.5 per 100 000 persons in Uganda.4 It is the most common, non-pigmented ocular surface tumor.5 OSSN occurs more commonly in middle-aged or elderly individuals. Lee and Hirst reported an average age of occurrence of 56 years, with a range of 4 to 96 years.3 Patients with xeroderma pigmentosum and human immunodeficiency virus develop OSSN at younger ages.6,7 It is also more common in fair-skinned individuals and males, with a fivefold higher incidence in Caucasian males.2 Numerous epidemiologic studies have identified ultraviolet B (UV-B) light as a major etiologic factor in the pathogenesis of OSSN.1,2,8,9 Newton et al. demonstrated a 49% decline in the rate of OSSN for each 10-degree increase in latitude, due to the decrease in solar ultraviolet radiation with increasing latitude.9 In a case control study, Lee at al. identified fair skin, pale irises, a propensity to sunburn, and prolonged sun exposure in early life as risk factors for OSSN.8 UV-B light is known to cause DNA damage through formation of pyrimidine dimers.10 Patients with xeroderma pigmentosum, who are more susceptible to the effects of sunlight, due to a defect in DNA repair mechanisms, have increased incidences of OSSN.6 It has been proposed the effect of UV-B radiation may be due to the overexpression of the p53 tumor suppressor gene.11 The increased frequency of OSSN since the advent of the acquired immunodeficiency syndrome (AIDS) epidemic, strongly suggests the role of the human immunodeficiency virus (HIV) in increasing the risk of developing OSSN.7,12 In a study in Malawi, 79% of patients diagnosed with OSSN were found to be HIV positive. In HIV patients, OSSN occurs at a younger age and tends to be more aggressive.12 This emphasizes the importance of testing for HIV in younger patients diagnosed with OSSN, as it may be the first presenting sign of the disease.7,12 Whereas, the role of HPV in the pathogenesis of cervical cancer has been well established, the role of HPV as an etiologic factor in OSSN remains unclear. Various studies have demonstrated an association between HPV subtypes and OSSN,13,14 while other studies have failed to show any association.15,16 Further evidence confusing the etiologic role of HPV includes the presence of unilateral OSSN in patients with bilateral conjunctival HPV DNA, the presence of HPV in normal conjunctival tissue, and the persistence of HPV infection many years after eradication of OSSN 13,17,18 It is possible HPV may not act alone but may require a cofactor, such as HIV or UV-B light, in order to cause disease.17,19 Other risk factors reported in the literature include heavy smoking and exposure to petroleum derivatives.20,21 It has also been reported in association with pterygium.22 Finally, there have been case reports of OSSN in immunosuppressed patients with neoplasia (lymphoma, leukemia) and following organ transplantation.23 Ocular surface squamous neoplasia, most commonly presents with foreign body sensation, irritation, redness, or a growth on the ocular surface.1 Lesions are typically unilateral and slow growing. More than 95% of these lesions occur in the mitotically active limbal region, within the sun-exposed interpalpebral zone.24,25 More rarely, it can involve the cornea or bulbar conjunctiva alone. It also can occasionally involve the forniceal or palpebral conjunctiva or involve the bulbar conjunctiva or cornea alone. The lesion may be fleshy and markedly elevated, sessile, or minimally elevated. The classic macroscopic appearance of OSSN is a gelatinous limbal mass with feeder vessels. It can be also have a papilliform appearance with a strawberry-like papillary growth at the limbus or demonstrate leukoplakic changes. (Fig. 19.1).1,26 Nodular and diffuse are two other appearances that have been described. The nodular form is well circumscribed and rapidly growing, while the diffuse form may mimic a chronic conjunctivitis and has a tendency for metastasis to regional lymph nodes.1 It may be difficult to distinguish CIN from squamous cell carcinoma (SCC) based on clinical examination. SCC may be larger and more elevated with a feeder vessel, and adherent to the underlying tissues (Fig. 19.2).27,28 CIN lesions tend to be freely mobile over the sclera. Ocular surface squamous neoplasia is most commonly misdiagnosed as pinguecula, pterygium, actinic keratosis and squamous papilloma, or episcleritis.29 Hirst et al. found in a histopathologic review of 533 pterygium specimens, 9.8% were found to have evidence of dysplasia.30 This supports the notion that all excised pterygium specimens should be submitted for pathology at the time of removal. The differential diagnosis includes other benign entities, such as pyogenic granuloma, inflammatory pannus, phlyctenulosis, and pseudoepitheliomatous hyperplasia. Amelanotic melanoma, sebaceous cell carcinoma, and keratoacanthoma can also rarely simulate OSSN.29,31 Keratoacanthoma can be distinguished by its rapid growth over several months. Papanicolaou smear cytology is widely accepted as a valuable diagnostic tool in the detection of cervical cancer and has also been described to be useful in the diagnosis of external ocular tumors.32 A cytobrush or spatula is used to scrape the surface of the suspicious lesion and the cells are sent on a slide to pathology, fixed with 95% alcohol, and stained using a Papanicolaou technique. A major disadvantage is that the superficial nature of the sample may lead to missing the tumor cells. In addition, with this technique, it is not possible to determine the degree of tissue invasion or localize the tumor.26 Impression cytology is another technique that can be used to obtain cells from the surface of the conjunctival lesion, with its use first described in limbal tumors in 1954.33 In this technique, a filter paper composed of cellulose acetate, millipore filter paper, or a biopore membrane device, is placed on the ocular surface using gentle pressure and subsequently fixed and stained with the Papanicolaou stain. Nolan and Hirst reported a sensitivity for the diagnosis of OSSN with impression cytology of only 78%.34 Unlike exfoliative cytology, this method allows for localization of the lesion with preservation of cell-to-cell relationships. Similar to exfoliative cytology, only superficial cells are obtained and thus, the presence of invasion cannot be determined. The advantage of both impression and exfoliative cytology is that they there are relatively simple, painless, and minimally invasive methods, which can be performed in the office after the application of topical anesthesia. They may also be a simple method for the detection of recurrences.32 There have been several reports of in vivo confocal microscopy as a useful tool in the diagnosis of OSSN.35,36 Confocal microscopy allows for real-time, noninvasive imaging at the cellular level by optical microscopic sectioning of the ocular surface. Malandrini and colleagues described a case of CIN, with a clear distinction between the healthy and pathological epithelium on confocal microscopy. The epithelial cells near the lesion were larger in size, more irregularly shaped, and demonstrated brighter nuclei.35 More recently, ultra-high resolution optical coherence tomography (UHR- OCT) has been described as a noninvasive diagnostic tool to evaluate ocular surface lesions. This technology allows for morphologic visualization of the corneal architecture, with an axial resolution of 2–3 µm. Kieval et al. found that UHR-OCT of pterygia and OSSN lesions demonstrated a high degree of correlation to histopathological specimens.37 The UHR-OCT of OSSN showed thickened epithelium with an abrupt transition from normal to neoplastic tissue (Fig. 19.3). UHR-OCT of pterygia demonstrated a normal thin epithelium, with thickening of the underlying subepithelial mucosal layers. The sensitivity and specificity for differentiating between OSSN and pterygia using UHR-OCT with an epithelial thickness cutoff of 142 µm was 94% and 100%, respectively.37 Pre-invasive OSSN lesions are classified as mild, moderate, or severe, based on the extent of replacement of the epithelium by dysplastic cells that lack normal maturation (Fig. 19.4A). The cells are usually long and elongated. Mild dysplasia (CIN grade I) is when the dysplasia is confined to the lower one-third of the epithelium. In moderate dysplasia (CIN grade II), the abnormal cells extend to the middle third of the epithelium. Severe dysplasia (CIN grade III) involves the full-thickness epithelium with total loss of the normal cellular polarity and is also known as CIS. The epithelial basement membrane is intact. Most conjunctival SCCA’s are well differentiated, demonstrating individually keratinzed cells (dyskeratosis) and concentric collections of keratinized cells (horn cells). Well-differentiated tumors demonstrate varying degrees of cellular pleomorphism with hyperchromatic nuclei, prominent nucleoli and the presence of mitotic figures. Hyperparakeratosis and parakeratoses are also present (Fig. 19.4B).26,27 Histopathologic variants with more aggressive behavior are spindle cell carcinoma, mucoepidermoid carcinoma, and adenoid squamous cell carcinoma.26 Surgical Excision with Cryotherapy Surgical excision, alone or in combination with medical therapy, is the most established treatment for OSSN. With surgical excision alone, the rate of recurrence is high, ranging from 5% to 33% with negative margins and up to 56% with positive surgical margins.26 A ‘no touch’ technique, in which touching the tumor with any instruments is avoided, reduces the risk of tumor seeding.38 Wide margins of 4–6 mm should be obtained. If the lesion extends into the sclera or cornea, a superficial keratectomy or partial-thickness sclerectomy may be needed. Absolute alcohol epitheliectomy of the involved cornea is also recommended. To delineate the margins of the lesion, rose bengal staining or UHR-OCT can be used. However, there is evidence that the microscopic signs of OSSN may extend beyond the macroscopic border the tumor,17 and many surgeons prefer adjuvant cryotherapy to the limbus and conjunctival margins at the time of excision. Cryotherapy is thought to work initially by its thermal effect and also by obliteration of the microcirculation, resulting in ischemic infarction and a double freeze–slow thaw technique is recommended.1 The rates of recurrence with excision and cryotherapy have been reported to be lower than with excision alone, at about 12%.19,39 Excess cryotherapy should be avoided, since side effects include iritis, abnormal intraocular pressure, sector iris atrophy, hyphema, ablation of the peripheral retina, corneal neovascularization, and limbal stem cell deficiency.1,19 Since wide excisions are recommended, surgical excision often results in large defects, necessitating the use of a conjunctival autograft, an oral mucosal graft, or an amniotic membrane transplant. A number of studies have described successful reconstruction of the ocular surface with preserved amniotic membrane after excision of CIN, SCC, primary acquired melanosis, and melanoma.40,41 Amniotic membrane is a helpful technique, since defects of any size can be closed, and the membrane has additional properties of promoting epithelialization, and reducing neovascularization, scarring and fibrosis.40 In addition, the use of fibrin glue, instead of sutures to secure the membrane reduces inflammation.42 The use of a conjunctival autograft of adequate size from either the same or opposite eye is an option. Care needs to be taken to avoid large areas of stem cell removal, which may lead to scarring, symblepharon, and limbal stem cell deficiency. Thick buccal or labial grafts are generally reserved for cases with extensive symblephara and might potentially interfere with the ability to observe for recurrence of the underlying tumor.40 In summary, the preferred technique for OSSN removal involves excision of the tumor with wide margins, absolute alcohol epitheliectomy of the involved cornea, cryotherapy using a double freeze–slow thaw cycle to the limbus and conjunctival margins, and amniotic membrane transplantation (Fig. 19.5). MMC is an alkylating agent that inhibits DNA synthesis by the production of free radicals. It is used as a topical drop at concentration of 0.02% or 0.04% four times daily for 7 to 14 days in cycles. One week is allowed between cycles to minimize ocular toxicity. Excellent responses raging from 87.5% to 100% have been reported.43,44 Side effects include conjunctival hyperemia, blepharospasm, corneal punctate erosions, punctal stenosis, and limbal stem cell deficiency.44 Punctal plugs should be used to prevent punctal stenosis. Refrigeration is required and at our institution (Bascom Palmer Eye Institute) the cost is about US$225 per bottle. 5-FU is a pyrimidine analogue that inhibits the incorporation of thymidine into DNA, during the S-phase of the cell cycle. It is prescribed as a 1% topical solution applied four times daily for 4 to 7 days, with 30–35 days off for a total of two to five cycles.45 It has also been used for 4 weeks continuously.46 5-FU may lead to ocular surface irritation and thus, 4 to 7 days a month dosing is preferred by the authors. Unlike MMC, it does not require refrigeration and is less costly (about US$75 per bottle). Interferon α is a family of proteins, secreted by leukocytes, with antiviral and antineoplastic properties. It has been used in the treatment of many cancers, including cervical intraepithelial neoplasia,47 cutaneous squamous cell carcinoma,48 and renal cell carcinoma.49 It has also been used to treat viral lesions, including hepatitis B and C, and condyloma acuminata.50 INF α-2b is a recombinant protein that has been used in the treatment of OSSN with success rates of above 80%.51,52 It can be given as topical eye drops or a subconjunctival injection, and a combination of both may be used. Topical INF α-2b is much better tolerated than MMC and 5-FU. Interferon drops are very gentle and well tolerated. Reported side effects include mild conjunctival hyperemia and follicular conjunctivitis.53 Topical INF α-2b (1 million IU/mL) is dosed four times daily and given continuously until the tumor resolves. It is not cycled like MMC and 5-FU and the cost is about US$225 per month for the eye drops. On average, the time on the medication is 3 months. Figure 19.6 demonstrates the case of a 54-year-old male with OSSN, which resolved after 12 weeks of treatment with topical INF α-2b. Interferon can also be given as subconjunctival injections. These may be given once to thrice weekly. Side effects of subconjunctival delivery include fever, chills, headache, myalgias, and arthralgias, which may last a few hours after the injection. Acetaminophen at a dose of 1000 milligrams every 6 hours is helpful. The time to tumor resolution is generally faster with subconjunctival injections (average 1.4 months), as compared to resolution topical INF α-2b drops (average 2.8 months).51,52 The subconjunctival dose is 0.5 mL (3 million IU/0.5 mL solution) repeated one to three times a week until clinical resolution occurs. A comparison of MMC, 5-FU, and INF-α-2b are summarized in Table 19.1. Ocular surface squamous neoplasia is considered a low-grade malignancy with a good prognosis, as the tumor is generally slow growing. Local recurrences are common, with most occurring within the first 2 years.1 Intraocular invasion and metastasis are extremely rare. Intraocular invasion is thought to occur by tumor cells entering the eye at the limbus and invading the trabecular meshwork, anterior chamber, ciliary body, iris and choroid.54 Sites of metastasis include the parotid gland, submandibular and submaxillary glands, preauricular, cervical lymph nodes, lungs, and bone and are related to a delay in management.55 Conjunctival melanoma is a tumor that arises from the melanocytes in the basal layer of the conjunctival epithelium. Other melanocytic lesions of the ocular surface include conjunctival nevi, racial melanosis, ocular melanocytosis, and primary acquired melanosis. Clinical features of each are summarized in Table 19.2. A conjunctival nevus is a pigmented or nonpigmented mass, which is mobile, circumscribed, and elevated. It is the most common conjunctival tumor, accounting for 28% of all conjunctival tumors and 52% of those classified as melanocytic tumors.5 Nevi usually present in childhood or early adolescence, most commonly located in the bulbar conjunctiva, caruncle, or plica semiluminaris. Intralesional cysts are commonly visible at the slit lamp (Fig. 19.7). Growth may occur with hormonal changes, such as during puberty or pregnancy, but otherwise the lesion size remains stable. In a study of 410 patients with conjunctival nevi, 1% showed evolution into melanoma over an interval of 7 years.56 Conjunctival primary acquired melanosis (PAM) accounts for 11% of all conjunctival tumors and 21% of melanocytic lesions.5 It presents as a unilateral, patchy area of conjunctival pigmentation in middle-aged or elderly adults with fair skin (Fig. 19.8). The pigmentation can wax or wane over time.28
Ocular Surface Neoplasias
Ocular Surface Squamous Neoplasia
Epidemiology
Etiology
Solar Ultraviolet Radiation
Human Immunodeficiency Virus (HIV) Infection
Human Papillomavirus (HPV) Infection
Other Etiologic Factors
Clinical Features
Differential Diagnosis
Diagnostic Evaluation
Exfoliative Cytology
Impression Cytology
Confocal Microscopy
Ultra-High Resolution Optical Coherence Tomography
Pathology
Treatment
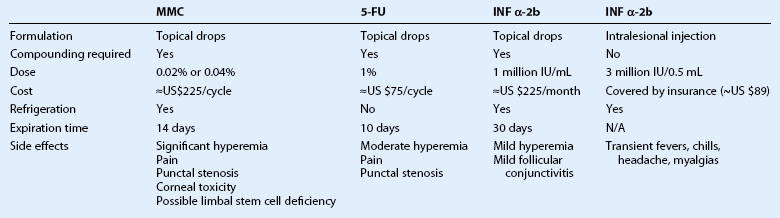
Antimetabolites
Interferon α-2b
Prognosis
Melanoctyic Tumors
Conjunctival Nevus
Primary Acquired Melanosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ocular Surface Neoplasias