Ocular Manifestations of HIV/AIDS
Nikolas J.S. London
Emmett T. Cunningham Jr
Acknowledgement
Supported in part by The San Francisco Retina Foundation and The Pacific Vision Foundation.
As of 2007, it was estimated that 33 million people worldwide were infected with the human immunodeficiency virus (HIV), with nearly 2.7 million new infections and 2.0 million AIDS-related deaths recorded that year.1 Although the pandemic persists in regions such as sub-Saharan Africa and globally in high-risk populations, the overall prevalence of infection appears to be stabilizing.1 Ocular manifestations of HIV/AIDS typically occur late in the course of disease, a state referred to clinically as acquired immunodeficiency syndrome (AIDS), and characterized by either profound CD4+ T-lymphocyte depletion (<200 cells/μL) or the development of opportunistic infections or unusual neoplasms (Figs. 36-1 and 36-2; Table 36-1).2,3,4 Since the original description of eye disorders in patients with HIV/AIDS by Holland et al5 in 1982, a number of clinic-based surveys6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31 (Table 36-2) and reviews32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50 have described the spectrum of ocular manifestations in HIV/AIDS. Without treatment, up to 70% of patients infected with HIV ultimately develop ocular complications of their disease, and postmortem findings suggest that the prevalence of ocular involvement can be as high as 95%. Although retinal microvasculopathy and cytomegalovirus (CMV) retinitis are far and away the most common complications, other ocular manifestations of HIV/AIDS also occur (Table 36-2) and can occasionally cause profound and permanent loss of vision.
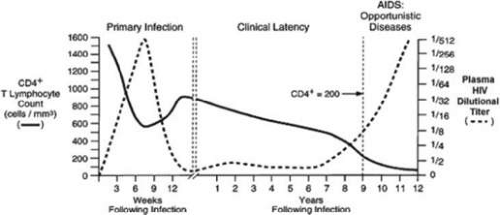 Figure 36-1. The natural history of HIV infection. Clinical phases include primary infection, clinical latency, and acquired immunodeficiency syndrome (AIDS). AIDS is characterized by low CD4+ T-lymphocyte counts (<200 cells/mm3), high viral titers, and increased susceptibility to opportunistic infections and unusual neoplasms. (Modified with permission from Fauci AS, Pantaleo G, Stanley S, Weissman D: Immunopathogenic mechanisms of HIV infection. Ann Intern Med 124:654, 1996.) |
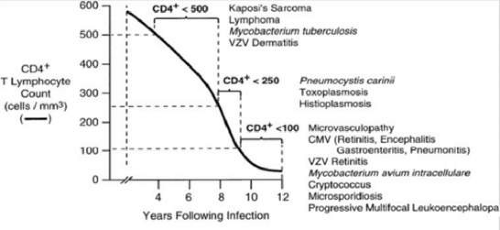 Figure 36-2. Typical CD4+ T-lymphocyte count range for presentation of various ophthalmic manifestations of HIV infection. Although uncommon, presentation at CD4+ T-lymphocyte counts greater than indicated can occur. |
TABLE 36-1. Conditions Included in the Revised 1993 AIDS Surveillance Case Definitions from the Centers for Disease Control | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 36-2. Prevalence of Ocular Disorders in Patients Infected with HIV | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The introduction of combined antiretroviral therapy in 1996 changed the face of HIV/AIDS-related eye disease. Termed highly active antiretroviral therapy (HAART), this drug regimen uses a combination of potent antiretroviral medications to inhibit replication of HIV. Patients on HAART typically experience a robust improvement in helper T-cell (CD4+) populations, which translates into fewer opportunistic infections, reduced morbidity and mortality, and improved overall quality of life. There has been a dramatic decline in eye-related opportunistic infections, with incidence rates of CMV retinitis and other HIV/AIDS-related ocular complications decreasing by 50% or more.51 Despite the dramatic decline in incidence following the introduction of HAART, ocular complications still occur and remain an important cause of disability in patients with HIV/AIDS. In addition, as a result of improved treatments for specific conditions and more effective and available antiretroviral drug combinations, patients are living longer at lower levels of immune capacity, leading to an increase in the prevalence of less severe, chronic conditions such as keratoconjunctivitis sicca and blepharitis.
Nearly 90% of patients with HIV/AIDS live in developing countries, regions where HAART is often less readily available.52 Patients in the developing world also tend to have less access to health care in general and are more likely to be exposed to region-specific pathogens. The spectrum of ocular complications associated with HIV/AIDS varies, therefore, from region to region.
ADNEXAL MANIFESTATIONS OF HIV/AIDS
In the pre-HAART era, adnexal manifestations of HIV/AIDS were seen in approximately 25% of patients (Table 36-3),53 and in many patients they were the presenting sign of systemic immunosuppression.36,50,54
TABLE 36-3. Adnexal Manifestations of HIV Infection | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
HERPES ZOSTER OPHTHALMICUS
Herpes zoster ophthalmicus (HZO) refers to a varicella-zoster virus (VZV)-related vesicular dermatitis involving the ophthalmic distribution of the trigeminal nerve.55 Although VZV dermatitis may be observed in otherwise normal elderly patients, its occurrence in someone younger than 50 years of age is uncommon and should raise the suspicion of systemic immunosuppression owing to malignancy, pharmacologic immune suppression, or HIV infection.44,56,57 VZV dermatitis related to HIV infection typically occurs at CD4+ T-lymphocyte counts of <200 cells/μL and is considered disseminated if it involves multiple dermatomes or unrelated organ systems. In the absence of HAART, herpes zoster ophthalmicus (Fig. 36-3) affects approximately 5% of HIV-infected patients (Table 36-2),41 many of whom relate a history of prior zoster infection. The incidence of HZO varies geographically, however, with rates in African countries reported to be more than four times greater than in western countries.13,20
 Figure 36-3. Herpes zoster ophthalmicus in a patient with AIDS. |
In addition to zoster-related skin lesions, other complications of varicella-zoster virus infection include keratitis, scleritis, uveitis, retinitis, and central nervous system involvement, all of which may be more common in patients with HIV/AIDS.56,57,58 A chronic VZV keratitis has been also described in HIV-infected patients,59 and debilitating postherpetic neuralgia may develop following the resolution of cutaneous disease.
The diagnosis of HZO is often made clinically but can be confirmed by viral culture, Tzanck smear, fluorescent antibody testing, antigen detection by direct immunofluorescence, and/or polymerase chain reaction of viral DNA in challenging cases.60 In immunosuppressed patients, VZV DNA can be found on the ocular surface for more than a month following the onset of rash, compared to only 2 days in healthy patients.61 To reduce the duration of skin lesions and occurrence of ocular complications, treatment should consist of a 5-day course of intravenous acyclovir (10 mg/kg, every 8 hours), followed by indefinite oral maintenance therapy (800 mg, three to five times daily).50,62 Both valacyclovir (1,000 mg, three times daily) and famciclovir (500 mg, three times daily) offer more convenient alternatives to acyclovir. For patients initially unresponsive to acyclovir, or for those who show reactivation on oral acyclovir, valacyclovir, or famciclovir, a trial of intravenous foscarnet or oral valganciclovir should be considered.63 Cases with significant anterior chamber inflammation or stromal keratitis should be treated concurrently with topical corticosteroids. Patients with persistent immune compromise should be examined regularly for posterior segment involvement, and all patients should be observed for postherpetic neuralgia.
HAART appears to have had a significant impact on the prevalence of HZO. In 1989 Jabs and et al20 reported HZO in 4% of 200 patients with HIV/AIDS, whereas it was seen in only 0.1% of 1,632 patients in a 2007 survey.51 Certain manifestations of HZO may be either more common or more severe following initiation of HAART, however. For example, an immune-mediated stromal keratitis has been described and is believed to represent an immune reconstitution inflammatory syndrome (IRIS) directed against retained viral antigen within the corneal stroma.64
KAPOSI’ SARCOMA
Kaposi’ sarcoma is a vascular mesenchymal tumor of the skin, mucous membranes, and gastrointestinal tract that, prior to the widespread availability of HAART, occurred in up to 30% of HIV-infected patients.48,65,66 Kaposi’ sarcoma appears to be more common in patients who acquire HIV through sexual intercourse, perhaps related to the fact that human herpes virus-8 itself is sexually transmitted.67,68,69 Kaposi’ sarcoma lesions involving the ocular adnexa were initially described as affecting approximately 5% of patients with HIV/AIDS.70,71 Involvement of both the eyelids and the conjunctiva (Fig. 36-4) has been described. Lesions on either the upper or lower eyelid may mimic a chalazion. Conjunctival lesions are most commonly found in the inferior fornix but may occur on any aspect of the palpebral or bulbar conjunctiva. Conjunctival lesions are typically red, minimally elevated, and mobile with or without associated hemorrhage. They are often mistaken for benign subconjunctival hemorrhage. Diagnosis of Kaposi’ sarcoma is based on clinical examination. Although not often performed, biopsy of suspicious lesions can provide a histopathologic diagnosis.
 Figure 36-4. Inferior conjunctival Kaposi’ sarcoma in a patient with AIDS. |
The primary treatment for Kaposi’ sarcoma is immune reconstitution with HAART. In cases of HAART failure or in regions where HAART is unavailable, directed treatment may be necessary. Indications include (i) compromised lid function, (ii) discomfort, and (iii) cosmesis. The treatment strategy depends on the size and location of the lesion. Radiation therapy is effective in treating eyelid and conjunctival Kaposi’ sarcoma, but it is expensive and can be associated with loss of lashes, skin irritation, and a mild conjunctivitis.72,73,74 Alternatively, isolated lesions of the eyelid may be treated by cryotherapy or intralesional chemotherapy.71,75 Excision can be performed but is often difficult and complicated by bleeding. Large lesions should be treated with a debulking modality prior to excision. Conjunctival lesions also respond to cryotherapy or intralesional chemotherapy, but unlike eyelid lesions, they can be excised with relative ease. Fluorescein angiography is occasionally helpful for identifying a tumor-free margin of 1 to 2 mm at the time of surgery. Eyelid or conjunctival lesions accompanied by systemic involvement are often best treated with systemic chemotherapy. Interferon a76,77 and vinblastine78,79 have also been used with success. Recurrences are common.75,80
MOLLUSCUM CONTAGIOSUM
Molluscum contagiosum is a highly contagious papulonodular dermatitis caused by the DNA poxvirus called molluscum contagiosum virus (MCV). Prior to the availability of HAART, molluscum was seen in 1% to 5% of patients.19,21,84 Recent estimates vary from 0.6% to nearly 5%, although varying study conditions make a direct comparison of these rates difficult.51,85,86
Although molluscum lesions tend generally to occur in children, immunosuppressed patients may develop molluscum lesions at any age. Both the skin and mucous membranes may be affected, typically with multiple, small, umbilicated cutaneous nodules. Molluscum contagiosum is more common in patients with HIV/AIDS as compared to nonimmunosuppressed patients and, when present, tends to be more severe, producing larger, more numerous, commonly bilateral, and more rapidly growing lesions that are resistant to conservative treatments.48,87,88 Molluscum contagiosum was initially reported to occur on the eyelids (Fig. 36-5) in <5% of patients infected with HIV (Table 36-2).84,89,90,91 Cases of conjunctival molluscum contagiosum are rare but have been described in the literature92,93 An association with follicular conjunctivitis and superficial keratitis has also been described in immunocompetent patients but appears to be uncommon in people with HIV/AIDS.
 Figure 36-5. Periocular molluscum contagiosum in a patient with AIDS. |
Immune reconstitution is important in treating the molluscum94; however, even with HAART, lesions can take up to 6 months to resolve. Moreover, new molluscum infections have been described in patients with IRIS, despite no prior history of the disease.95 Direct treatment options include application of liquid nitrogen, treatment with topical chemotherapy agents such as trichloroacetic acid and Cantharidin, incision with curettage, cryotherapy, and excision. Topical imiquimod has shown promise in recent clinical studies.96 Recurrence of eyelid lesions within 6 to 8 weeks of treatment is common in patients with AIDS.84 Recurrences following immune reconstitution appear to be more mild.53
SQUAMOUS CELL CARCINOMA/CONJUNCTIVAL INTRAEPITHELIAL NEOPLASIA
Patients infected with HIV appear to be at increased risk for the development of conjunctival and eyelid squamous cell carcinoma (SCC), possibly associated with an increased prevalence of human papillomavirus (HPV) infection.97,98,99,100,101,102 Moreover, lesions in patients with HIV/AIDS often follow a more malignant course.98,102,103 A higher prevalence of SCC cases associated with HIV infection have been reported out of sub-Saharan Africa, suggesting either an increased risk for or prevalence of infection in this region.104,105,106 In fact, in African cohorts SCC is the presenting sign of HIV/AIDS in up to 50% of patients.105,107 Diagnosis of SCC is based on biopsy with histopathologic examination. When the limbus is involved, gonioscopy should be performed to rule out intraocular extension.43 Treatment consists of wide excision with frozen section monitoring of the margins. Alternative treatment modalities include topical mitomycin-C,108 5-fluorouracil,109,110 and interferon-alpha.111 Immune reconstitution alone can lead to complete regression.112
CUTANEOUS LYMPHOMA
Non-Hodgkin’ lymphoma (NHL) is more common and tends to be of greater malignancy in patients with HIV/AIDS.113 Second to Kaposi’ sarcoma, NHL is the second most common opportunistic neoplasm in patients with HIV/AIDS,50 and is more common in patient with CD4+ cell counts <50 cells/μL. HAART has had a significant impact on the incidence of HIV-related NHL, reducing the incidence by nearly 50%. NHL of the eyelid can be either a manifestation of systemic disease or an isolated local neoplasm.29 Workup for systemic disease should be considered in all cases of ocular or periorbital lymphoma. Diagnosis is based on histopathologic examination of biopsied tissue. Treatment includes chemotherapy and local radiation therapy.45,117
TRICHOMEGALY
Acquired trichomegaly, or hypertrichosis of the eyelashes (Fig. 36-6), typically occurs in the late stages of HIV infection.118,119,120,121,122 The cause is unknown, although elevated viral titers, drug toxicity, and poor nutrition have been implicated as contributing factors. Lashes rarely grow beyond 12 mm,123 and cessation of growth may correlate with immune reconstitution.124 Excessively long lashes may be trimmed, as needed, if they interfere with the use of eyeglasses or if the patient finds them cosmetically unacceptable. The impact of HAART on trichomegaly is not known.
 Figure 36-6. Trichomegaly, or hypertrichosis of the eyelashes, in a patient with AIDS. |
CONJUNCTIVAL MICROVASCULOPATHY
In the absence of HAART, most HIV-infected patients will eventually develop conjunctival microvascular changes, including segmental vascular dilatation and narrowing, microaneurysm formation, the appearance of comma-shaped vascular fragments, and a visible granularity to the flowing blood column, termed “sludging.”114,115 These changes are typically asymptomatic and are usually most evident near the limbus inferiorly (Fig. 36-7). Conjunctival microvascular changes are highly correlated with the occurrence of retinal microvasculopathy. The reason for the occurrence of conjunctival microvascular changes in the setting of HIV infection is unknown and likely multifactorial. Theories have included an HIV-induced increase in plasma viscosity,115 HIV-related immune complex deposition,25 and direct infection of the conjunctival vascular endothelium by HIV. No treatment is indicated.36,54
 Figure 36-7. Conjunctival microvasculopathy at the inferior limbus in a patient with AIDS. |
CONJUNCTIVITIS
In one of the first clinic-based cohort studies, Holland et al29 reported a nonspecific, culture-negative conjunctivitis in 10% of patients with AIDS. More recent clinic-based studies have, however, reported a prevalence of <1%, similar to that of the general population (Table 36-2). Uncommon infectious forms of conjunctivitis have been reported in HIV-infected patients, including cytomegalovirus125 and Cryptococcus.126 These reports are from the pre-HAART era, however. Empiric treatment should be guided by clinical examination and tailored according to the results of the Gram stain and cultures.
PRESEPTAL CELLULITIS
Preseptal cellulitis caused by Staphylococcus aureus has been reported in two HIV-infected patients.19,104 Staphylococcus aureus is the most common cause of cutaneous and systemic bacterial infections in HIV-infected patients, and these patients infected with Staphylococcus aureus have a nasal carriage that is nearly twice that of normal controls.48 Treatment is the same as that used for preseptal cellulitis in immunocompetent patients.
ANTERIOR SEGMENT MANIFESTATION OF
HIV/AIDS
Prior to HAART, anterior segment findings accounted for up to 20% of the ocular complications associated with untreated HIV infection (Table 36-4).36,54,127
TABLE 36-4. Anterior Segment Manifestations of HIV Infection | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
KERATOCONJUNCTIVITIS SICCA
Keratoconjunctivitis sicca (KCS), or dry eye, was initially reported to occur in 20% to 39% of HIV-infected patients, more often in men, and typically at late stages of their illness.128,129,130,131,132 Abnormal Schirmer’ testing and interpalpebral rose bengal staining (Fig. 36-8) are invariably present. The cause is complex but is most probably related to combined effects of HIV-mediated inflammation and destruction of the lacrimal and salivary glands (Sjögren’ syndrome) and direct HIV infection of the conjunctiva.130,133,134 Concurrent exposure owing to lagophthalmos and decreased blink rate in the setting of encephalopathy can worsen the keratopathy. Treatment consists of artificial tears and long-acting lubricating ointments, which are applied at bedtime. Punctal occlusion may be of benefit in resistant cases. The introduction of HAART appears to have had little impact on the prevalence of KCS.53
 Figure 36-8. Interpalpebral rose bengal staining of the conjunctival and corneal epithelium in an AIDS patient with dry eyes. |
INFECTIOUS KERATITIS
Infectious keratitis occurs at about the same rate in HIV-infected and HIV-uninfected persons, with most cohorts reporting keratitis in <1% of patients (Table 36-2). However, when HIV-positive patients do acquire infectious keratitis, the organisms are more likely to be opportunistic, and the course more severe or protracted.36,54,127 Most of the etiologies described in subsequent sections occur at various CD4+ T-cell counts, with the exception of microsporidial keratitis, which is uncommon at counts >100 cells/µL. The impact of HAART on the incidence and causes of infectious keratitis has not been described.
VIRAL KERATITIS
Herpes zoster ophthalmicus is often associated with either a dendritic epithelial (Fig. 36-9) or disciform stromal keratitis in HIV-infected patients.135 VZV keratitis can, however, also occur with transient or no skin lesions, a condition termed herpes zoster sine herpete, that has been reported to occur rarely in HIV-positive persons.59,136 Decreased corneal sensation and elevated intraocular pressure are clues to the diagnosis. Diagnosis is based on clinical examination and can be confirmed with viral culture, direct fluorescent antibody studies, and polymerase chain reaction of viral DNA, if necessary. Treatment is similar to that for herpes zoster ophthalmicus, as discussed in prior sections.
 Figure 36-9. Conjunctival injection and rose bengal staining of multiple corneal epithelial pseudodendrites in an AIDS patient with herpes zoster keratitis. |
Herpes simplex keratitis, in contrast, does not seem to be more common in HIV-positive patients.127,137,138,139 HIV-associated herpes simplex keratitis may, however, recur more frequently and in some cases be more resistant to treatment than similarly severe cases occurring in immune-competent patients.138 At least one case series has suggested that herpes simplex epithelial keratitis may occur more commonly near the limbus and with more and larger dendrites in HIV-infected patients.139
Diagnosis is similar to that for VZV. Treatment of simplex-related keratitis may involve administration of oral acyclovir (400 mg, five times daily), valacyclovir (1,000 mg, three times daily), or famciclovir (500 mg, three times daily),140,141,142 or treatment with topical antivirals such as trifluridine 1% (nine times daily) and vidarabine ointment 3% (five times daily). Long-term suppression should be achieved with 400 mg of oral acyclovir twice daily.139 Debridement of the diseased epithelium, which is removed relatively easily with a topical anesthetic and a cotton swab, may increase the healing time. Patients should be followed very closely until resolution is complete.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


