Fig. 12.1
Globe dystopia after aggressive anterior orbital floor decompression
Thus we choose to avoid opening the medial wall anterior to the anterior ethmoidal foramen and the floor anterior to the maxillary sinus osteum. This approach involves removal of the posterior-inferomedial strut, which is vital for decompression in dysthyroid optic neuropathy, and serves to create space for axial expansion of the orbit posteriorly. There is also a theoretic benefit to maintaining the major normal maxillary and ethmoid sinus outflow mechanisms, which may reduce the risk of postoperative sinusitis and mucoceles.
The lateral orbit was classically the first to be removed for orbital decompression [52]. Early reports involved removal of the lateral orbital rim and the thin bone overlying the temporalis muscle [53, 54] and this method persists to modern times [55, 56]. However, only limited amounts of proptosis reduction can be achieved in the anterior orbit, where extra-axial globe displacement predominates over axial proptosis reduction. It is advantageous to leave this bone, and rather remove the bone of the deep lateral orbit. The deep bone of the sphenoid diploe lies directly behind globe and allows posterior displacement of the globe in addition to volume expansion.
There is another aesthetic advantage to leaving the anterior lateral wall. The proptosis of TED is associated with some widening of the interpupillary distance, which is part of the disfigurement. Removing the anterior lateral wall can allow the globe to lateralize, widening the interpupillary distance further, which is aesthetically undesirable. Leaving the anterior lateral wall in the area of the equator of the globe minimizes this tendency for expansion of the interpupillary distance. Removing the anterior lateral wall over the temporalis muscle also creates continuity between the orbit and the temporalis fossa, which can induce oscillopsia [55, 57].
Leaving an eggshell of bone over the temporalis muscle and concentrating on the removal of the deep bone of the lateral wall can mitigate these consequences [58]. It is also possible that the deep lateral decompression has a lower incidence of new onset strabismus [59]. These material and theoretic benefits make deep lateral decompression our first choice for decompression requiring moderate amounts of proptosis reduction.
Minimally Invasive Orbital Decompression: Indications and Technique
Patients with even minor amounts of proptosis can have significant congestion that may benefit from orbital decompression (Fig. 12.2). Additionally, holistic cosmetic rejuvenation may warrant 1–3 mm of proptosis reduction in some cases, such that the lid position and periorbital hollows can be optimally managed.

Fig. 12.2
Tense, congested orbit with chemosis and subsequent resolution with symptomatic relief after bilateral decompression
One approach that can be useful involves carving out the basin of the inferior orbital fissure through a transconjunctival incision [60]. This technique entails an inferior transconjunctival approach to the orbital floor. A subperiosteal flap is elevated and the region surrounding the tip of the inferior orbital fissure is exposed. The bone in this region is composed of the thick body of the zygoma and the lateral extent of the maxilla overlying the maxillary sinus (Fig. 12.3). This can be carved with a drill, or if the patient is not sedated, using sharp bone curettes to create a rounding of the lateral orbit (Fig. 12.4). Some opening of the lateral maxillary sinus roof is acceptable in this situation; however opening the central anterior floor can lead to globe dystopia and should be avoided. Fat decompression in the inferior intraconal space can augment proptosis reduction, and both carry low rates of new onset diplopia around 7–8 % [60–64].
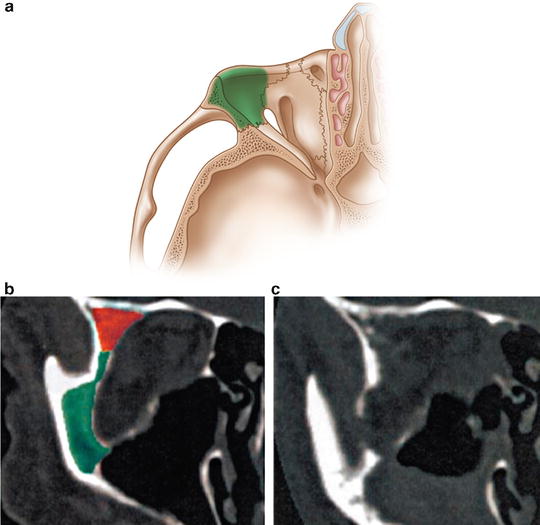
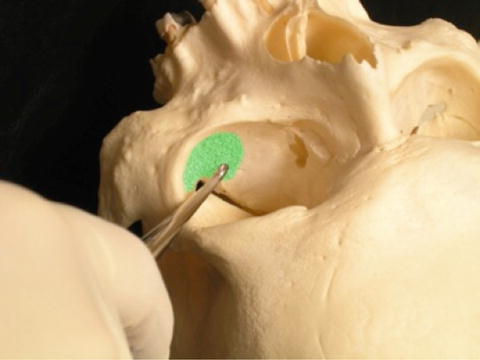
Fig. 12.3
(a) The green area outlines the thick bone of the inferolateral orbit. The middle frame (b) outlines the same bone on coronal computed tomography, and the right pane (c) demonstrates the change in volume with decompression of this bone
Fig. 12.4
Bone of the lateral orbit that can be accessed with a boney curette
In patients with congestion but only mild proptosis, orbital fat removal alone may allow adequate decongestion and proptosis reduction; through conjunctival approaches, both the inferolateral and inferomedial intraconal pockets can be accessed. A suction cutting technique allows the fat to be gently teased out of the orbit and removed. The fullness of the anterior pads will often improve after removal of intraconal fat, and aggressive removal of the anterior “blepharoplasty” fat can create a hollow appearance (Fig. 12.5). However, if a patient has profound fullness of the anterior fat pads, conservative debulking of these pads can be considered in conjunction with removal of the deeper intraconal fat.

Fig. 12.5
Late overcorrection after aggressive decompression of anterior orbital fat
Strabismus
Strabismus surgery has important aesthetic implications. It is well established that manifest strabismus can negatively impact self-perception, social functioning [65], and overall QoL [66]. Studies specifically related to TED have confirmed this relationship, as patients with diplopia are more likely to have symptoms of depression [18], occupational disability [7], and impaired perceptions of their own functional, social, and psychological well-being [3, 5, 12, 67].
Classically staged surgical rehabilitation in TED [19] leaves the patient to suffer the consequences of strabismus often for more than 2 years. However, it is possible to offer minimally and noninvasive measures during this period, as outlined in earlier sections.
When the appropriate time comes for strabismus surgery, TED patients are nearing the end of their facial transformation/rehabilitation cycle. They have often gone through the most significant surgery of the process in decompression. This “home stretch” can be agonizing for patients who have already been through a difficult experience. The implication of this understanding is that any opportunity to combine surgeries and shorten the overall length of rehabilitation will be welcomed.
One strategy that has been employed in this regard is to combine inferior rectus recession surgery with lower lid retractor release [68–70]. This procedure can reduce the amount of retraction caused by inferior rectus recession [71]. We generally prefer to perform it in a minimally invasive en glove fashion [72, 73]. This can be combined with volume augmentation in the form of a dermis fat graft or fat pearl transfer (Fig. 12.6) if necessary. It is also useful to place the lower eyelid on stretch with a Frost suture, which can be loosened in the postoperative area for adjustment of strabismus sutures, and then re-tightened.
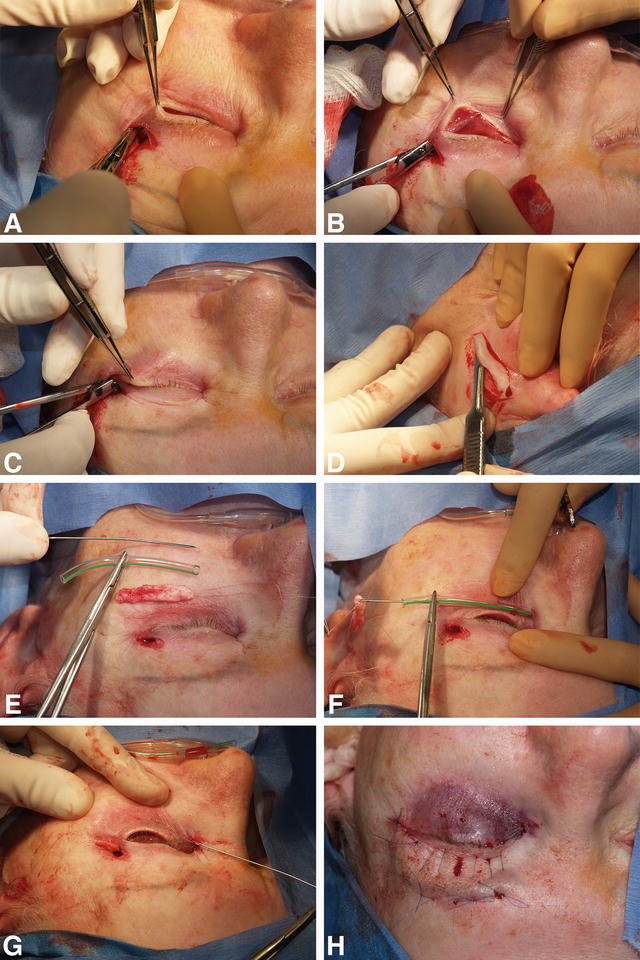
Fig. 12.6
Surgical series of en glove lysis for lower eyelid retractors with dermis graft placement. (a) A small lateral crows feet or lid crease incision is made. (b) The lower eyelid retractors are released from the conjunctiva, creating a window pane thin posterior lamella. (c) The orbicularis retaining ligament is released with blunt stretching between the tarsus and the orbital rim. (d) A de-epithelialized dermis strip graft is harvested, in this case from the retroauricular area. (e) A protective sheath is fashioned from intravenous tubing to match the length of a Keith needle. (f) The distance is estimated and the guarded needle is passed through the dissection pocket created earlier. (g) The guard is removed and the dermis graft on a suture is passed through the pocket from lateral to medial. (h) The eye is placed on stretch with a Frost suture
Eyelid Retraction
Lid retraction is one of the most common and earliest signs of TED. It is cosmetically unappealing to patients and can contribute to ocular irritation in the form of exposure keratopathy. Classically and definitively, the treatment for retraction is surgical, and a wide range of techniques for both the upper and lower eyelids have been described. Surgery is typically deferred until the post-inflammatory stage of disease, after decompression and strabismus correction have been performed. This time period can be condensed with temporizing measures and by combining retraction surgery with other stages of rehabilitation.
There are a few minimally invasive techniques for the management of upper eyelid retraction in active TED. Injecting triamcinolone into the space between Müller’s muscle and the conjunctiva has been shown to lower the eyelid and reduce swelling [74, 75]. It is not well established if these injections act like orbital depot injections [76–79] or by some other site-specific mechanism. Their use is limited as the long-term effect is unknown, dosing is not well established, and they carry a small risk of embolic complications.
Similarly, botulinum toxin has been injected into Muller’s plane to achieve temporary eyelid lowering [80–84]. This approach has not been widely adopted as the dosing can be variable and rates of temporary ptosis and induced diplopia approach 20 %. Additionally, neither botulinum toxin nor triamcinolone can be used for lower eyelid retraction.
Hyaluronic acid (HA) gels have gained wide popularity for cosmetic applications in filling volume deficit areas [85]. These fillers can be effective in correcting both upper [86] and lower eyelid retraction secondary to TED [87, 88]. This strategy is advantageous in that it is titratable, repeatable, and reversible. These features make their use in TED ideal for active stage disease, when the eyelid position may be changing, and for inactive disease when small amounts of residual asymmetry are evident (existing or postoperative). Some cases may completely avoid surgery altogether. This is considered an off-label use of the medication.
The procedure is performed by first anesthetizing the conjunctiva topically. The upper eyelid is then everted and the conjunctiva just superior to the upper tarsal edge is exposed. Using a 30-gauge needle, a single bolus of HA is placed centrally in the subconjunctival levator-Muller plane. Small volumes (0.1–0.2 mL) of material are injected iteratively with the end point being adequate lid lowering and improved symmetry (Fig. 12.7).
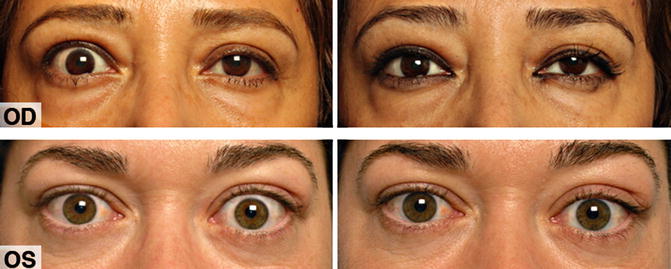
Fig. 12.7
Hyaluronic acid gel injection for upper lid retraction. On the left is pre-injection and on the right is at 3-month follow-up. The upper series represents active, inflammatory stage disease, while the lower series shows quiescent disease
In patients who do require eyelid retraction surgery, it may be advantageous to combine this procedure with decompression. The philosophy here is to usher patients along their course of rehabilitation in a more expedient manner, accepting that small touch up stages of surgery may be required later.
Orbital decompression can lead to small alterations in upper eyelid position [89, 90], and in many cases decompression surgery should be performed prior to eyelid retraction repair. However, patients without any pre-existing motility restriction and mild to moderate eyelid retraction can benefit from combined upper eyelid retraction and decompression surgery [91–93]. Although it is possible that secondary surgeries may be required, such patients tend to have similar final outcomes to staged surgery [91]. The same can be said for combined lower eyelid-decompression surgery [94]. In both cases, small position and contour abnormalities can be managed postoperatively in an office setting with HA fillers.
In terms of surgical technique, a wide range of procedures have been described and most produce acceptable, although periodically unpredictable, results. En glove approaches for both upper and lower eyelid retraction are favored in the case of combined orbital surgery, as this tends to avoid making supplementary incisions. For the upper lid, after lateral decompression, the upper eyelid crease incision can be utilized, or the eyelid can be everted for a posterior approach. A small button hole is made through the lateral horn of the levator aponeurosis and a pocket is dissected between the conjunctiva and levator planes. A blunt dissection stretching maneuver can lengthen the central aponeurosis and sharp dissection of the lateral and medial horns can be graded for contour. Small side cuts into the central pedicle of aponeurosis can increase lid-lengthening effect (Fig. 12.8).
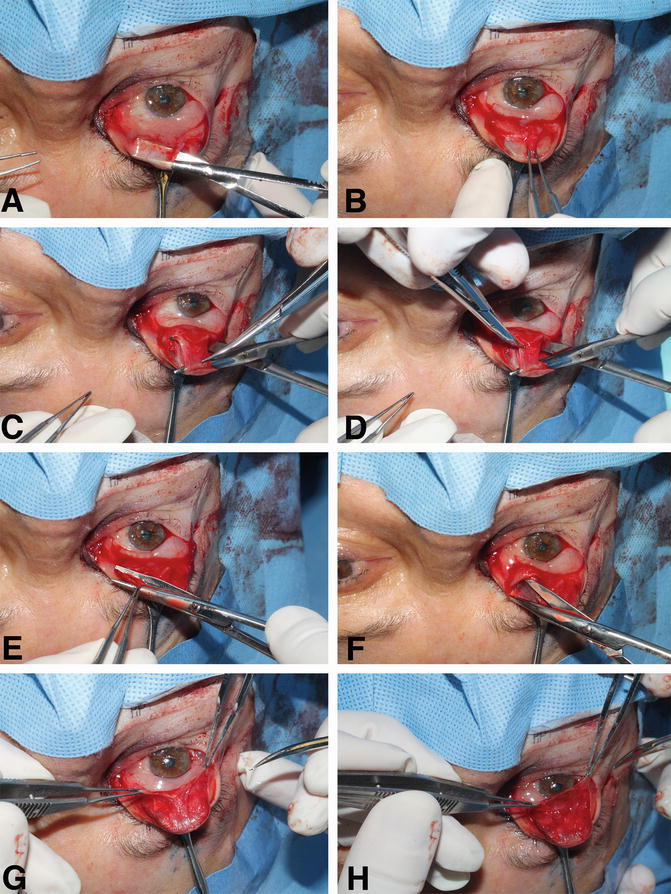
Fig. 12.8
Upper lid retraction stretching sequence. (a) The lid is everted and the conjunctiva is incised. (b) The levator aponeurosis is grasped. (c) A plane between the levator aponeurosis and Muller’s muscle is dissected, the levator is stretched and a small myotomy is made laterally adjacent to the tarsus. (d) A similar incision medially is made more superiorly. (e) The lateral and medial horns of the levator are opened. (f) Stretching is performed in these spaces and contour adjusted. (g) The conjunctiva is elevated and the Muller’s muscle is dissected cleanly off its posterior surface. (h) Window pane thin conjunctiva is demonstrated. The iris should be visible through the tissue
In any upper eyelid retraction surgery, it is important to consider the aesthetic consequences of the brow fat span (BFS)—tarsal platform show (TPS) relationship. Lengthening of the eyelid, without addressing the BFS–TPS ratio can lead to less appealing results with a long TPS, further accentuating the proptotic TED appearance. Further, this can also create the perception of a ptotic and tired eyelid. In cases where there is a short TPS preoperatively (or relatively short compared to the contralateral side), a posterior eyelid lengthening approach may be ideal [91]. However, if there is current or a high risk of late TPS elongation, an anterior approach is preferred, as it allows access to the anterior orbital fat pads and the retro-orbicularis oculus fat in order to contour and manage the BFS. The purpose of this redraping would be to elongate the BFS and the TPS simultaneously in order to maintain the BFS–TPS ratio [95].
In the lower lid, entry through the upper eyelid incision laterally and dissection of the retractors off of the conjunctiva and tarsus can be performed in en glove fashion [72, 73]. If a fat decompression is performed, some small 0.5 mm fat cobblestones can be fashioned from the excised tissue and used as volume augmentation if required.
Periocular Rejuvenation
The stigmata of TED are contextualized within the natural processes of facial aging. Loss of skin elasticity, deepening of glabellar and other furrows, facial volume loss and tissue descent each have aesthetic implications for TED patients as they do for patients without TED. Additional considerations including the coarsening of facial features, expansion of the lateral brow fat and tendency to form fluid pockets in the periorbital region further complicate facial rejuvenation in TED.
Accordingly, treatments to improve facial skin quality including chemical peels, laser treatments, and other skin care regimes can benefit patients with TED. Botulinum toxin can be extremely effective in effacing dynamic and static rhytids over time. Volume augmentation, whether by synthetic fillers [96], fat grafting [97] or transposition and lifting procedures [98] can also benefit appropriately selected patients with periorbital volume collapse (from natural processes or anterior fat decompression) (Fig. 12.9).

Fig. 12.9
Advanced periocular rejuvenation. The top panel shows preoperative appearance. The second panel is after bilateral decompression. The bottom two panels are after the first and second layer of hyaluronic acid gel filler to the periorbital hollows, respectively
The expansion of the lateral brow fat pad [39–41] can be particularly concerning to patients with TED (Fig. 12.10). This is a difficult problem, as no reliable and reproducible techniques for the management of this problem are currently described. In general, during blepharoplasty or eyelid lengthening, this fat pad can be accessed through an eyelid crease incision. Debulking with sharp dissection and/or contouring with electrocautery can be performed.

Fig. 12.10
Lateral expansion of the brow fat relative to the pre-thyroid eye disease state
Concluding Remarks
Smoking cessation, comfort measures and environmental modification can improve the TED experience for patients. Additionally, minimally invasive procedures such as hyaluronic acid gel fillers and botulinum toxin for lid retraction and strabismus can reduce the cosmetic and functional implications of disease while awaiting stabilization for definitive therapy. Surgical rehabilitation that follows can be graded and individualized for the aesthetic and functional needs of each patient. In each phase, the patient and surgeon must consider the aesthetic implications of each surgical approach and weigh them carefully. Surgical approaches to the orbit were discussed that avoid a skin incision or that conceal the incision within the lid crease. The advantages of the lid crease approach to the lateral wall include the excellent access to the deep lateral orbit, avoiding damage to the lateral canthal angle and orbicularis, and minimizing the risk of postoperative diplopia.
The facial metamorphosis in TED can be extensive, and should be contextualized within the natural processes of aging. Taking a holistic view of periorbital rejuvenation during each stage of disease and reconstruction will allow orbital specialists to approach the goal of restoring TED patients to their pre-morbid state.
References
1.
2.
3.
Kahaly GJ, Petrak F, Hardt J, Pitz S, Egle UT. Psychosocial morbidity of Graves’ orbitopathy. Clin Endocrinol (Oxf). 2005;63:395–402.CrossRef
4.
Park JJ, Sullivan TJ, Mortimer RH, Wagenaar M, Perry-Keene DA. Assessing quality of life in Australian patients with Graves’ ophthalmopathy. Br J Ophthalmol. 2004;88:75–8.PubMedCentralPubMedCrossRef
5.
6.
7.
Ponto KA, Pitz S, Pfeiffer N, Hommel G, Weber MM, Kahaly GJ. Quality of life and occupational disability in endocrine orbitopathy. Dtsch Arztebl Int. 2009;106:283–9.PubMedCentralPubMed
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


