32 Nonacoustic Cerebellopontine Angle Tumors
The cerebellopontine angle (CPA) is a complex intracranial space that contains cranial nerves and vascular structures, surrounded by the meninges and the arachnoid of the cerebellopontine cistern. CPA tumors are the most common neoplasms in the posterior fossa, accounting for 5 to 10% of intracranial tumors. Most CPA tumors are benign, with over 85% being vestibular schwannomas (acoustic neuromas), lipomas, vascular malformations, and hemangiomas. The most frequent nonacoustic CPA tumors are meningiomas, epidermoids (primary cholesteatomas), and facial or lower cranial nerve schwannomas. Primary malignancies or metastatic lesions account for less than 2% of neoplasms in the CPA.
We shall consider the clinical features and management of epidermoids, lipomas, and posterior fossa meningiomas in this chapter.
Lipomas
Intracranial lipomas are rare tumors, which may occur in the CPA or internal auditory canal (IAC). The earliest observations of intracranial lipomas were made by neuroanatomists and pathologists in 1818, 1856, and 1897,1 but a detailed study has been done in the past 60 years.2 Till date about 100 cases have been reported in the literature.3 Lipomas develop from mesenchymatous cells and presumably are caused by aberrant differentiation of primitive meningeal matter during the ingrowth of vascular connective tissue,4 instead of a neoplastic process.5,6
Intracranial lipomas have been associated with malformations of the skull and brain such as cranium bifidum, spina bifida, microcephaly, meningoencephalocele, and other malformations7 and this supports the concept of the dysgenetic origin of the disease.8 The prevalence of lipomas is approximately 1 or 2 among 1000 autopsies,9 which suggests that symptomatic and extant lesions have substantially different occurrence rates. They are found in approximately 1/1000 computed tomography (CT) scans, but only 1/70 are intracranial tumors.9 The incidence of this lesion is neither age nor gender related and they have been found in both children and adults.10
Localization
Small accumulation of fat cells have been reported in many sites of the primitive meninges,1 in the central area at the base of brain11 and in the pia of the corpus callosum; the most common site involved.12 Most of the lesions (80%) are found in the supratentorial area whereas lesions in the dorsal pericallosal area accounts for nearly 50%. Isolated intraventricular lipomas may occur but rarely, and those of cerebral cortex are extremely uncommon.13 Other typical location in supratentorial sites includes the chiasmatic and sylvian cistern.14 A very small percent of all intracranial lipomas (0.14%) involves the CPA or the IAC.15 Rarely these neoplasms are bilaterally present.
Clinical Manifestations
Most lipomas are asymptomatic and are diagnosed as accidental findings. Symptomatic lipomas present with variable features and one of the more classical presentations is the triad of CPA syndrome: unilateral loss of hearing (62 to 71%), unilateral tinnitus (42 to 71%), and episodic vertigo (associated often with nausea and vomiting [41%] analogous to an acoustic schwannoma).3,16 These symptoms can be progressive and may vary in combination. Other manifestations include facial pain, neuralgias, paresthesias, auricular fullness in the affected ear, headaches, hemifacial spasms (9%), and rarely ataxia or dysdiadochokinesia.
There is a little difference in presentation between CPA and IAC lipomas. When localized in the CPA they may present quite a varied course and nonacoustic symptoms such as hemifacial spasms or pain may dominate.9 Fluctuant sensorineural hearing loss (SNHL) and episodic dizziness can be present.17 IAC lipomas have a slowly progressive course, often similar in symptoms complex to acoustic schwannoma, with mainly SNHL and tinnitus.
Histopathology
CPA and IAC lipomas are yellowish smooth or lobulated masses sometimes with a delicate capsule. More frequently they are not capsulated. Their consistency may be soft or hard. The tumor is often densely adherent to the brainstem as it blends into the entry site of the cranial nerves VII and VIII roots, which it regularly surrounds. It may also incorporate cranial nerve or it may surround the cranial nerves IX, X, and the portion of XI. Sometimes the tumor can be limited to IAC and subsequently may extend into or be restricted to the CPA. Lipomas are made up of mature adipose tissue traversed by strands and sheets of vascular connective tissue and portions of cranial nerves. The adipose tissue tends to splay apart and infiltrate the nerve fibers. The connective and adipose tissue may be closely associated with numerous blood vessels of different caliber.
Imaging
Radiologically, IAC lipomas can be associated with bone erosion, while it is atypical for CPA lipomas.18 CT scans show a typical low-density mass that has attenuation characteristics similar to adipose tissue (−50 to −100 Hz). On magnetic resonance imaging (MRI), lipomas appear similar to fat, are hyperintense compared with brain on T1-weighted images (Fig. 32.1), and hypointense on standard T2-weighted spin echo frequencies (Fig. 32.2). After gadolinium (Gd) administration there is no enhancement. A differential diagnosis with similar T1 images includes hemorrhage or highly proteinaceous fluid. Fat suppression techniques in T1-weighted scans can be used to confirm the diagnosis as with this technique a lipoma changes from the high signal intensity to an isointense aspect.18–20
Treatment
Surgical treatment of lipomas in CPA and IAC is challenging, because of the frequent involvement of the cranial nerves and vascularity of these tumors which presents more risk of intraoperative bleeding; more than other CPA lesions.3,5 Because of infiltration of cranial nerves, even a simple biopsy or partial resection can cause important postoperative consequences. Christensen et al confirmed the real difficulties envisaged in attempting total removal of these tumors.21 Saunders et al agree that only partial excision can be achieved and preservation of hearing, when attempting removal of these tumors, seems to be an unachievable goal.15 The translabyrinthine approach allows a complete resection of CPA and IAC tumors, as it provides a wide exposure of the surgical field, complete control of the IAC fundus, and good management of the facial nerve from brainstem to IAC. As a consequence hearing, if present, will be sacrificed.22 Middle cranial fossa and posterior fossa approaches allow preservation of hearing in 26% of cases even in partial resection cases.23 Surgical resection should be reserved for those patients who present debilitating symptoms such as vertigo, facial weakness, and trigeminal neuralgia.24 Conservative management is possible because of the slow growth (only one case reported 15% increased tumor size in 8-year period)23 and benign nature of this tumor.
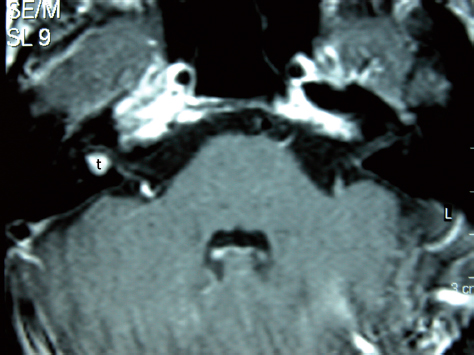
Figure 32.1 T1-weighted magnetic resonance imaging—axial. The tumor (t) is hyperintense compared with brain. L, lipomas.
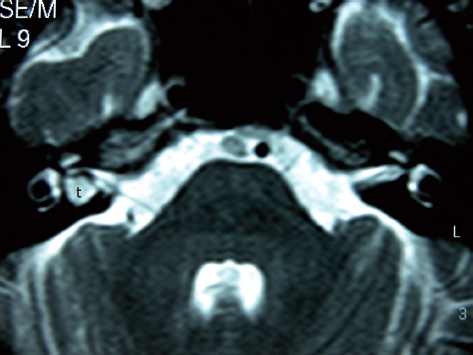
Figure 32.2 T2-weighted magnetic resonance imaging—axial. The tumor (t) appears hypointense compared with brain. L, lipomas.
Epidermoids of the Cerebellopontine Angle
Epidermoid tumors arise from sequestration of remnant epidermal cells at the time of closure of the medullary groove; they are considered dysontogenetic tumors rather than true neoplasms.25 Epidermoid cysts are also called pearly tumors or cholesteatomas. Epidermoids were described historically in 1745 by Verattus, but the first “modern” description of the epithelial origin was by Bostroem.1
Epidermoids are classically classified in two main groups: intradural and extradural. Epidermoids represent 0.2 to 1.5% of all intracranial tumors.26,27 Intradural tumors are more frequent and are principally located in the subarachnoid cisterns. Within this region they seem to occur more frequently in the CPA (30 to 40% of cases), parapontine region, chiasmal area, parapituitary region, and sometimes can be trantentorial.26 In the CPA epidermoids account for 6 to 7% of all lesions.28 Extradural epidermoids may be located anywhere in the skull, frequently being found in the calvaria of the frontal and parietal bones, usually not penetrating the frontal sinus. Epidermoids may also rarely involve the temporal bone and sphenoid. Within the temporal bone they are called petrous bone cholesteatomas with a different management.29 They originate within diploe subperiosteally and therefore epidurally.
Lepoire and Pertuiset classified intradural epidermoids based on vessel involvement.30 Samii et al published a classification of posterior fossa epidermoids that introduced the concept of extension to better define the size of the tumor and the surgical implications.31 This classification divides the posterior fossa into four compartments: (1) between the undersurface of the tentorium and the trigeminal nerve; (2) from the trigeminal nerve to the lower border of the cranial nerves VII and VIII; (3) down to the lower cranial nerves; and (4) from the lower cranial nerves to the foramen magnum.
Histopathology
On macroscopic examination, epidermoids present as bluish white lesions with a capsule that has a mother-of-pearl appearance (Fig. 32.3). It is subtle and elastic and may contain foci of calcification. The surface is often lobulated or nodular. After section, they display a homogeneous appearance with soft waxy, white, or creamy material arranged in an onion-skin like fashion. This results from constant exfoliation of keratin and cholesterol from the epithelial lining of the cyst. Some cysts tend to spread with finger-like extensions along preformed clefts, surrounding blood vessels, cranial nerves, and cerebral or cerebellar hemispheres.
Histological analysis of the capsule usually shows three normal layers of the epidermis. The continuous desquamation of keratinous material is the main cause of the gradual expansion of the cyst.
Clinical Behavior
The age of occurrence ranges from 0 to 80 years with a small prevalence of males to females, although the majority of intracranial epidermoids are diagnosed between the third and fourth decades, during peak clinical manifestations. Occasionally epidermoids can be bilateral.32
Epidermoids are slow growing tumors and are often asymptomatic for years.33 They may irritate adjacent structures causing symptoms such as trigeminal neuralgia, facial paresis or paralysis, hemifacial spasm, optic neuritis, and diplopia (Fig. 32.4). The rupture of the capsule with subdural diffusion of the keratin results in a severe inflammatory reaction (arachnoiditis and meningitis). Although they are usually benign lesions, malignant transformation has been reported.34 Generally recurrences are because of incomplete removal of the capsule.
The intradural epidermoids of CPA develop in the subarachnoid space of the lateral pontine cistern (Fig. 32.5). The symptoms may present in two main forms. In 25 to 50% of cases the presenting symptom is an atypical trigeminal neuralgia with a longer duration of pain and possible involvement of other cranial nerves (depending on the size). The remaining 50 to 75% of CPA epidermoids present themselves with signs of a slowly expanding mass, such as progressive facial palsy, hemifacial spasm, tinnitus, and progressive SNHL, sometimes associated with dysequilibrium and nystagmus. The facial nerve is involved earlier than in a vestibular schwannoma, because epidermoids tend to strangulate the nerve affecting its blood supply. Occasionally the cranial nerves IV, VI, and XI may be involved but the absence of cranial nerve dysfunction in many patients reflects the slow growth and benign nature of these cysts. In cases of large tumors pyramidal signs can sometimes be observed. Hydrocephalus is said to be infrequent because of the long-standing character of the lesion and also because cerebrospinal fluid (CSF) can filter through the crevices of the lesion. Often the capsule of epidermoids in CPA can be adherent to the brainstem and dura.
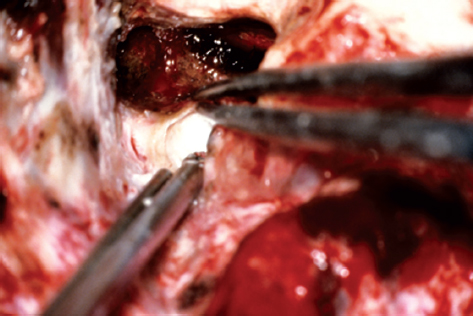
Figure 32.3 The tumor appears as a soft whitish mass. Debulking starts with preservation of neurovascular structures.
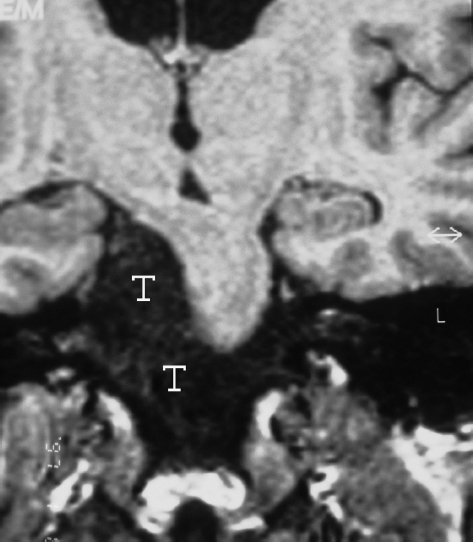
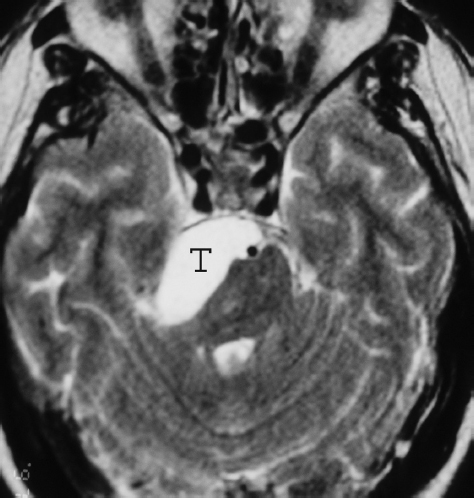
Figure 32.4 Magnetic resonance imaging—coronal. The patient, a 30-year-old man, complained of right diplopia of 3-month duration with palsy of the right abducent nerve. A hypointense neoformation (epidermoid) (T) is present at the level of the cerebellopontine angle. L, lipomas.
Imaging
Advances in neuroradiological imaging have drastically altered the methodology for diagnosis and management of these tumors allowing a more detailed examination and facilitating surgical planning.35 On CT scans, the lesions appear as nonenhancing, low density, and homogeneous mass, often lobulated, with low attenuation and foci of calcifications that may be present along the capsule. The high fat content of these lesions causes a low density appearance allowing differentiation from a dermoid cyst. Massive contrast intake may be a sign of malignant transformation.36 A small lesion can often be confused with an enlarged CPA cistern.37 The IAC is usually not enlarged, but the porus may be eroded.
Angiography may show displacement of the vessels in the posterior fossa without signs of hypervascularity. MRI is now the standard technique for diagnosis of an epidermoid cyst. The signal is low on T1-weighted images, because of proteinaceous content of cysts, without contrast enhancement. On T2-weighted images the signal become hyperintense and nonhomogeneous, generally differing from CSF, especially in proton-density sequence. The main radiological challenge is in distinguishing epidermoids from arachnoid cysts as their surgical management varies radically. Fluid attenuated inversion recovery (FLAIR) and echo-planar diffusion imaging are two kind of sequences that can discriminate between epidermoids and arachnoid cysts.38 On FLAIR sequences epidermoids appear hyperintense (protein content), while arachnoid cysts are hypointense (black—CSF content) while on echo-planar diffusion scans a high signal is indicative of epidermoids and a low signal of an arachnoid cyst.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


