Neurologic
Alex V. Levin
Thomas W. Wilson
J. Raymond Buncic
During embryogenesis, the brain and many ocular structures are derived from neuroectoderm. Therefore, many structural abnormalities of the brain will be associated with ocular anomalies. Optic nerve hypoplasia is associated with anterior pituitary abnormalities, agenesis of the corpus callosum, absence of the septum pellucidum, and schizencephaly.
Morning glory disc can be associated with basal encephalocele, and tilted disc syndrome can be associated with suprasellar tumors.
Nystagmus and abnormalities of extraocular eye movements are commonly external signs of neurologic abnormalities. Infants with constant exotropia will often have developmental delay. Specific nystagmus patterns can help localize structural pathology (downbeat nystagmus—Arnold Chiari malformation). Myasthenia gravis, multiple sclerosis, mitochondrial diseases, and storage disease will often present with ocular/visual abnormalities prior to systemic symptoms.
Increased intracranial pressure from brain tumors or pseudotumor cerebri can present as vision loss and examination of the optic disc reveals papilledema. Headaches are a common reason for referral to an ophthalmologist. The cause of headache is rarely secondary to strabismus or refractive error. However, careful neuro-ophthalmic examination, including evaluation of the visual acuity, visual fields, color vision, pupils, and extraocular movement as well as visualization of the optic disc, is required to exclude any underlying pathology.
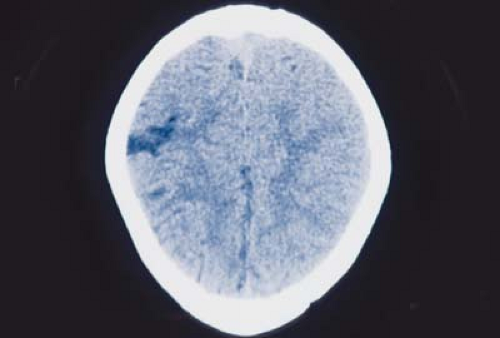 Figure 21.1 Schizencephaly Schizencephaly is an abnormality of brain cell migration during embryogenesis. Normal cell migration is dependent upon a radial glial fiber system that orients the neuronal tissue into its proper anatomic location. Schizencephaly represents abnormal clefting within the cerebral hemispheres. These defect(s) may be unilateral or bilateral, fused or unfused, large or small. Porencephaly refers to enclosed cysts within the cerebral tissue. Associated clinical findings with schizencephaly include severe mental retardation and associated seizures, which are often unresponsive to conventional treatment. |
 Figure 21.2 Holoprosencephaly Holoprosencephaly is an abnormality of development of the midline structures of the brain and face. Clinical features of holoprosencephaly include agenesis of the premaxilla, cleft upper lip (left image), hypotelorism, mental retardation, microcephaly, and oligodontia. A mild form of the disease will present as hypotelorism and mild changes of the midface. A severe form of holoprosencephaly with cyclopia is incompatible with life (right image). Multiple genetic and chromosomal abnormalities have been identified in holoprosencephaly. Surgical reconstruction of the face, including cleft palate repair, are indicated for severe defects. |
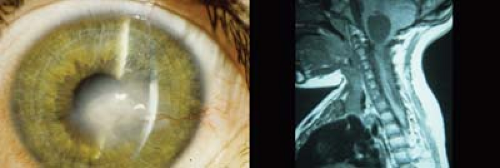 Figure 21.3 Arnold-Chiari Malformation Arnold-Chiari malformation is characterized by extension of the brainstem and cerebellar tissue into the cervical canal (right image). The inferior part of the fourth ventricle may also be displaced downward. It is commonly associated with spina bifida and myelomeningocele (Arnold-Chiari type II). Patients typically present with signs of increased intracranial pressure, including headache and visual loss. Patients may also demonstrate downbeat or seesaw nystagmus, ataxia, multiple cranial neuropathies, and quadriparesis. Stretching of the trigeminal nerve can cause corneal anesthesia with painless scarring of the cornea (left image). Posterior fossa decompression and/or shunting may be required. |
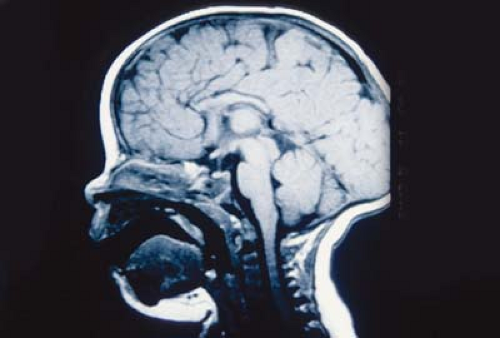 Figure 21.4 Aicardi Syndrome Aicardi syndrome is an X-linked dominantly inherited disorder that is lethal in males and involves the brain and eye. Infant girls present with infantile spasms and seizures and have significant developmental delay and mental retardation. This computed tomography scan of the brain shows a sagittal midline view, demonstrating absence of the corpus callosum. The brain shows a variety of anatomic abnormalities including schizencephaly, cysts, hemispheric asymmetry, and migration abnormalities (pachygyria and microgyria). The corpus callosum is formed from the commissural plate, and insults to this embryologic tissue cause agenesis. |
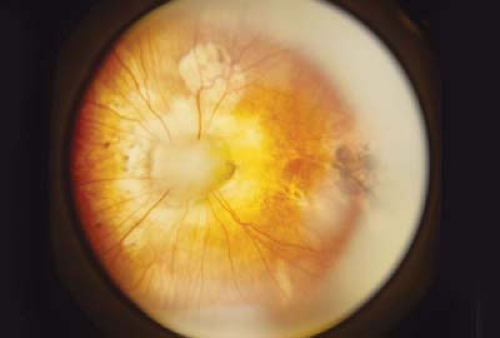 Figure 21.5 Aicardi Syndrome—Ocular Findings Characteristic ocular findings of Aicardi syndrome include well-circumscribed lacunae in the retina. Histopathologically, these lesions represent defects in the chorioretina, including the retinal pigment epithelium, to variable depths. Patients may also have optic disc colobomas or other less specific optic disc anomalies. The retinal lacunae are multiple and are concentrated about the optic disc. These lesions are classic for Aicardi syndrome. Patients may also have abnormalities of the vertebrae. The disease is lethal in males. A careful family history, including a history of multiple miscarriages during pregnancy, should be obtained in cases where Aicardi syndrome is suspected.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|