Neurectomy Procedures for Vertigo
Herbert Silverstein
When medical management of patients with Meniere’s disease fails, vestibular neurectomy is among the procedures of choice if hearing is to be preserved. The operation is effective in relieving vertigo attacks caused by Meniere’s disease while preserving hearing in 90% of patients. Although the most common inner ear disorder treated by vestibular neurectomy is classic Meniere’s disease, vestibular neurectomy is useful in selected cases of recurrent vestibular neuronitis, traumatic labyrinthitis, and vestibular Meniere’s disease. In deciding when to operate, the patient’s preference is a strong consideration. Some patients may have one or two severe episodes per month that do not affect their lifestyle sufficiently to warrant a major surgical procedure. Other patients, even those with only a few attacks per year, may be so severely affected that they live in constant dread of the next recurrence. There should be objective evidence of unilateral inner ear disease. Unless patients are experiencing an acute Meniere’s attack, they should be able to perform a tandem gait test reasonably well.
Contraindications to vestibular neurectomy include bilateral vestibular disease; poor general health, particularly when associated with physiologic old age; disequilibrium; an only hearing ear; or indications of other central nervous system disease. Vertigo from an ear with very poor hearing (80-dB speech reception threshold [SRT] with less than 20% discrimination) is usually more appropriately treated with transtympanic cochleovestibular neurectomy or labyrinthectomy. Previous transmastoid surgery of the endolymphatic sac is not a contraindication, nor is old age when the patient is healthy and has good balance function. Elderly people usually require more time to regain good balance function than do younger individuals. Vestibular neurectomy has been performed successfully in patients in their 70s, with no additional morbidity.
Although the middle fossa approach for selective vestibular neurectomy provides control of vertigo, the procedure is formidable and anatomic landmarks are difficult to determine. In general, patients more than age 60 years are not candidates for this approach because of the difficulty in elevating thin dura from the floor of the middle fossa and decreased tolerance for retraction of the temporal lobe.
ANATOMY: VESTIBULAR, COCHLEAR, AND FACIAL NERVES
At the fundus of the internal auditory canal, six separate branches of the seventh and eighth cranial nerves enter the internal auditory canal. They are the facial nerve, nervus intermedius, superior vestibular, saccular, posterior ampullary, and cochlear nerve. The transverse (falciform) crest divides the fundus into superior and inferior compartments. The vertical crest separates the superior half of the fundus into an anterosuperior quadrant for the facial nerve and nervus intermedius and a posterosuperior quadrant for the superior vestibular nerve. Anterior and inferior to the falciform crest lies the cochlear nerve, hidden from the surgeon by the inferior vestibular nerve. The posterior ampullary nerve lies in a separate canal (the singular canal) that enters the internal auditory canal in the posteroinferior quadrant, approximately 2 mm medial to the falciform crest. This reliable landmark is the point at which drilling stops when the posterior wall of the internal auditory canal is being surgically removed. A thin section computed tomograph (CT) of the labyrinth is routinely obtained to visualize the location of the singular canal. The inferior vestibular nerve is formed by the junction of the saccular nerve and joins the posterior ampullary nerve at the level of the singular canal in the posteroinferior quadrant.
The superior vestibular nerve innervates the superior and lateral cristae, the utricular macula, and sends a small twig to the anterosuperior part of the saccular macula. The inferior vestibular nerve innervates most of the saccular macula and the posterior crista.
Whereas the superior and inferior vestibular nerves are separated in the lateral part of the internal auditory canal, they fuse as they travel toward the porus acusticus. In the lateral part of the internal auditory canal, the cochlear nerve lies anteroinferior and the vestibular nerves lie posterior, but they fuse into a single trunk, known as the eighth cranial
nerve, near the porus or medial to it. As the combined nerve trunk passes toward the porus, the cochlear and vestibular segments rotate 90 degrees (1). As viewed by the surgeon, the rotation is clockwise on the left and counterclockwise on the right, so that the cochlear nerve shifts from an anteroinferior to a posteroinferior position relative to the vestibular nerve as it travels toward the porus (2). Most of the rotation occurs within the internal auditory canal; only a slight rotation occurs in the cerebellopontine angle (Fig. 30.1). The 90-degree rotation of the cochlear and vestibular nerves is not recognized in modern neurologic publications (3). The cochlear nerve enters the brainstem caudal and slightly dorsal to the vestibular nerve. The flocculus of the cerebellum covers 5 mm of the eighth cranial nerve at the brainstem.
nerve, near the porus or medial to it. As the combined nerve trunk passes toward the porus, the cochlear and vestibular segments rotate 90 degrees (1). As viewed by the surgeon, the rotation is clockwise on the left and counterclockwise on the right, so that the cochlear nerve shifts from an anteroinferior to a posteroinferior position relative to the vestibular nerve as it travels toward the porus (2). Most of the rotation occurs within the internal auditory canal; only a slight rotation occurs in the cerebellopontine angle (Fig. 30.1). The 90-degree rotation of the cochlear and vestibular nerves is not recognized in modern neurologic publications (3). The cochlear nerve enters the brainstem caudal and slightly dorsal to the vestibular nerve. The flocculus of the cerebellum covers 5 mm of the eighth cranial nerve at the brainstem.
The cochleovestibular cleavage plane can usually be identified grossly. The surgical view will show the vestibular fibers to be cephalad or superior and the cochlear fibers to be caudal or inferior. Occasionally, inferior vestibular fibers will course with the cochlear nerve (Fig. 30.2). In the cerebellopontine angle, the cochleovestibular cleavage plane appears grossly as a fine septum along the eighth cranial nerve in 75% of patients.
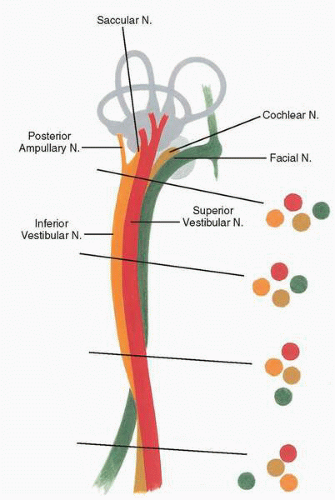 FIG. 30.1 Anatomy of the seventh and eighth cranial nerves as seen from the surgical position during the left retrosigmoid-internal auditory canal approach. Note the 90-degree rotation of the cochlear and vestibular nerves. |
The facial nerve remains ventrally positioned and hidden by the eighth cranial nerve along much of its course and assumes a ventral-caudal position as it enters the brainstem. In the internal auditory canal, the facial nerve is connected to the superior vestibular nerve by the Rasmussen facialvestibular anastomosing fibers, and in the cerebellopontine angle the facial nerve lies adjacent but distinct from the eighth nerve. Although it remains hidden from the surgeon’s view by the eighth cranial nerve in the retrosigmoid approach, the facial nerve can easily be seen by gentle retraction of the superior vestibular nerve in the internal auditory canal or the eighth nerve in the cerebellopontine angle. The facial nerve enters the brainstem 3 mm ventral and usually caudal to the eighth nerve route entry zone. In the internal auditory canal, the facial nerve appears whiter than the eighth nerve, and in the cerebellopontine angle it appears grayer.
The nervus intermedius, which may consist of a single nerve or multiple bundles, travels between the facial and eighth nerves through their entire course. The nervus intermedius enters the brainstem closest to the eighth nerve and usually delineates the cochleovestibular cleavage plane on the anterior surface of the eighth nerve.
OPERATIVE APPROACHES FOR VESTIBULAR NEURECTOMY
Retrolabyrinthine Vestibular Neurectomy
The retrolabyrinthine approach had been previously described for use in patients with trigeminal neuralgia, and it is also a convenient approach for selective vestibular nerve section (4).
In this procedure, a simple mastoidectomy is performed. Both the lateral venous sinus and posterior fossa dura anterior and posterior to it are exposed. The endolymphatic sac is widely exposed, and the bony contour of the posterior semicircular canal is identified. The lateral venous sinus is retracted posteriorly, and the dura is incised anterior to the sinus to create an anteriorly based dural flap. Intravenous mannitol (1.5 g/kg) is administered when the drilling begins. This causes contraction of the cerebellum and allows a wider exposure of the cerebellopontine angle (Fig. 30.3). Cochlear nerve action potentials may be monitored during the course of surgery if desired.
In 75% of cases an identifiable cleavage plane exists between the cochlear and vestibular fibers of the eighth cranial nerve in the cerebellopontine angle. From the surgeon’s view, the cochlear fibers compose the inferior portion of the nerve and the vestibular fibers compose the superior portion. The fifth cranial nerve is identified superiorly and the ninth, tenth, and eleventh nerves inferiorly. After the cleavage plane is visualized under high magnification, an incision is made in the cleavage plane, the cochlear and vestibular fibers are separated, and the vestibular nerve is transected with microscissors. Helpful landmarks to find the cochleovestibular cleavage plane are as follows: (i) The cochlear nerve appears whiter because its fibers are more numerous and closely packed. (ii) A fine blood vessel may be seen passing on the surface between the cochlear and vestibular fibers. (iii) The cochleovestibular cleavage plane is sometimes more visible from the anterior surface of the eighth cranial nerve (a mirror can be used to view this). (iv) The nervus intermedius, if identified, usually lies in the cleavage plane. When a cleavage plane cannot be readily identified, the superior half of the eighth cranial nerve is transected. When this technique is used, most vestibular fibers will be cut and most cochlear fibers will be spared.
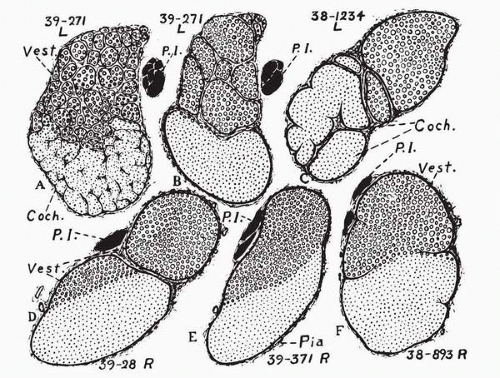 FIG. 30.2 Diagrams showing the funicular pattern of the eighth nerve from human adults. The cochlear and vestibular regions are distinguished from each other by different types of stippling. The solid black areas (P.I.) represent pars intermedia (nerve of Wrisburg) of the seventh cranial nerve. A: Cross-section slightly central to the vestibular ganglia. Both cochlear and vestibular portions consist of many small bundles, the cochlear having commenced to fuse. B: A section of the same nerve as A taken 2 mm farther centrally, showing not only complete fusion of the cochlear but several vestibular fasciculi. The vestibular bundles ultimately fuse with each other and with the cochlear component until a single trunk is formed (similar to E). C: A case where neither cochlear nor vestibular nerves are completely fused through most of their course in the internal auditory meatus and subarachnoid space. D: Example of the condition where the eighth nerve is represented by two distinct trunks, one of which was apparently purely vestibular, whereas the other was mostly cochlear, but with a prominent vestibular region amounting to about one-fifth of the cross-sectional area of the cochlear trunk. E: Example of a common condition where there is a single trunk, a little more than half of which (upon microscopic examination) is found to be vestibular and the rest cochlear. F: A case where incomplete glial septa roughly indicate the division between cochlear and vestibular trunks. There are generally at least a few vestibular fibers on the cochlear side of such septa. (From Rasmussen GL. Studies of the VIIIth cranial nerve of man. Laryngoscope 1940;50:67-83.) |
 FIG. 30.3 The retrolabyrinthine exposure of the seventh and eighth cranial nerves. The vestibular nerve has been transected. |
In reviewing 67 patients, 82% were free of vertigo, 10% were improved, and 8% noted no change postoperatively. Sensorineural hearing has been maintained within 20 dB of the preoperative level in 71% (5). Some patients experienced a mild conductive loss in the low frequencies, presumably from bone dust entering the middle ear causing fixation of ossicles.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


