78 A 34-year-old woman involved in a motor vehicle accident struck her upper face to the dashboard with brief loss of consciousness. The steering wheel and windshield were broken with extensive damage to her car. She was transported by ambulance to the emergency department. On physical examination, she was alert and oriented ×4. Her vital signs were stable. Her C-collar was in place, and two intravenous lines were in place. A 3-cm laceration was over her superior nasal dorsum. The nasal dorsum was obviously depressed with the nasal bones visible through the open wound. With gentle manual manipulation, loose crepitance was evident on the nasal pyramid. No septal hematoma and no evidence of cerebrospinal fluid (CSF) leak was evident. Her eye examination showed normal extraocular movements, and her vision was intact to finger counting. Her pupils were equal and reactive to light. Her intercanthal distance was 42 mm. Her facial buttresses other than her central naso-orbital region were intact. Her cervical spine was later cleared, and her chest radiograph was clear. The remaining physical examination was benign (Fig. 78.1). 1. With any facial injury, a complete systemic trauma evaluation is required. The overall status of the patient must be evaluated and take priority (airway, breathing, circulation, cervical status, intracranial status). Only after these are steps are stabilized can obvious facial injuries be addressed. In some instances, the facial fractures may need to be addressed in a later setting, depending on the medical status. 2. The face is examined to evaluate the extent of the fractures while being cognizant of possible injury to surrounding structures, including the orbits and globe, the frontal lobe, the frontal sinus, the medial canthi, and the lacrimal system. Any evidence of CSF leak must be ruled out. 3. Patients with naso-orbito-ethmoid (NOE) fractures may have up to 67% of ocular injuries, with 20 to 25% of these serious and 3% resulting in blindness. 4. Classic clinical findings supporting naso-orbital injury include the following: Fig. 78.1 Patient before repair. 5. The clinical diagnosis of NOE fractures might not be obvious because of significant soft tissue swelling masking the underlying skeletal injury of the central midface. Classic nasal findings include a loss of height of the nasal dorsum with superior rotation of the nasal tip (the pig-nose deformity). At times, NOE fractures will be detected only by imaging studies. 6. Complex NOE fractures can be the most challenging facial fractures to repair. Achieving the same pretrauma nasal appearance and medial canthal position can be difficult to attain, and the patient should be informed of this fact. 7. Bimanual examination by placing a mosquito clamp in the nose and digitally palpating the medical canthal on the same side can help determine whether free mobility is present at the naso-orbital ethmoid area. In the past, the eyelid traction test (pulling the lower eyelid laterally away from the nose) has been described as the classic sign for traumatic telecanthus; however, this finding may be evident only in severe cases. Fine-cut coronal and axial computed tomography (CT) scans (1.5-mm slices) of the face are helpful to delineate the fractures and their displacement when the patient is stabilized (Fig. 78.2). Impacted naso-orbito-ethmoid complex fracture Fig. 78.2 Computed tomography scan (axial view) of the face shows the lacrimal crests bilaterally splayed apart with a traumatic telecanthus.
Naso-Orbito-Ethmoid Fractures
History
Differential Diagnosis—Key Points
 An intercanthal distance greater than one half the interpupillary distance
An intercanthal distance greater than one half the interpupillary distance
 An intercanthal distance greater than 35 mm
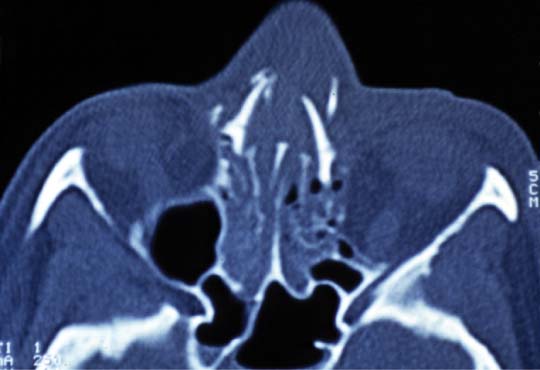
An intercanthal distance greater than 35 mm
 Medial canthus rounding
Medial canthus rounding
 Epiphora resulting from injury to the nasolacrimal duct system or a displaced punctum
Epiphora resulting from injury to the nasolacrimal duct system or a displaced punctum
 Enophthalmos
Enophthalmos
 Dystopia
Dystopia
Test Interpretation
Diagnosis

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


