This article discusses the development and anatomy of the nasal septum and structures of the lateral nasal wall. Emphasis is placed on anatomic variations associated with surgically correctable nasal obstruction. Common variations, such as deviated nasal septum, inferior turbinate hypertrophy, paradoxic middle turbinate, and concha bullosa, are discussed. Rare developmental causes of nasal obstruction are briefly outlined.
This article describes the development and anatomy of the nasal septum and structures of the lateral nasal wall. A clear understanding of the development and anatomic variations of the nasal septum and structures of the lateral nasal wall is vital for successful treatment of nasal obstruction. With knowledge of the specific location and anatomic reason for a patient’s nasal obstruction, clinicians can better identify the specific structure responsible for the obstruction and thus implement a more targeted approach to treatment.
Nasoseptal embryology
The tissue that gives rise to the face and nasal structures derives from three different embryonic sources: the ectoderm, the neural crest, and the mesoderm. The ectoderm provides an overlying cover and, through its interactions with mesenchymal layers, a pattern for developing structures. Neural crest cells provide the majority of facial mesenchymal tissue. The paraxial and prechordal mesoderm provides precursors for myoblasts that differentiate into voluntary craniofacial muscles.
At 4 weeks’ gestation, five identifiable primordial structures surround the stomodeum, a depression below the developing brain and the first sign of a future face. These five structures are the frontonasal prominence, the right and left maxillary prominances, and the right and left mandibular prominances. The maxillary and mandibular prominences lie superolaterally and inferolaterally bilaterally respectively. By the end of the fourth week of gestation, paired thickenings of ectoderm appear on the frontonasal prominence superior and lateral to the stomodeum. These oval placodes develop into the nose and nasal cavities ( Fig. 1 ).
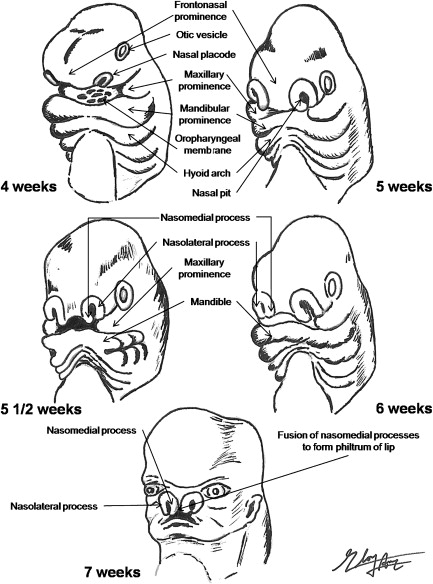
During the fifth week, mesenchymes on the periphery of the nasal placodes proliferate to form horseshoe elevations. The lateral and medial limbs are termed nasolateral and nasomedial processes respectively. Mesenchymal tissue surrounding the nasal placodes continues to proliferate and thicken, resulting in a perceived depression of the placodes. These depressions are subsequently called the nasal pits and are the primordia of anterior nares and nasal cavities (see Fig. 1 ).
From 5 weeks’ gestation, the nasal pits continue to deepen toward the oral cavity. By 6 and one-half weeks, only a thin oronasal membrane separates the oral cavity from the nasal cavaties. This oronasal membrane subsequently disintegrates, leading to a communication to the nasal cavities posterior to the primary palate. These regions of continuity are the primordial choanae. As the palatal shelves fuse and the secondary palate develops, the nasal cavity lengthens, resulting in the junction of the nasal cavity and the pharynx.
Beginning from the fourth to sixth week of gestation, the paired maxillary processes grow medially toward each other and toward the paired nasomedial processes. By the end of the sixth week, the nasolateral processes begin to fuse with the maxillary processes to form the ala nasi and the lateral border of the nostril bilaterally (see Fig. 1 ). Along the junctions of the nasolateral and maxillary processes lie the nasolacrimal grooves. Ectoderm within these grooves thickens to form epithelial cords, which then detach and canalize to form nasolacrimal ducts and lacrimal sacs. By late fetal period, nasolacrimal ducts extend the medial corners of the eyes to the inferior meatuses in the lateral wall of the nasal cavity.
The nasomedial prominences continue to expand but remain unfused until the seventh or eighth week of gestation, when they merge with superficial components of the maxillary processes. The fusion lines between these processes are the nasal fins. As mesenchymes penetrate this articulation, a continuous union is formed, completing most of the upper lip and upper jaw bilaterally (see Fig. 1 ). The nasomedial processes then merge with each other, forming the intermaxillary segment and subsequently displacing the frontonasal prominence posteriorly. The intermaxillary segment formed from the nasomedial processes is the precursor to several structures, including the primary palate, the tip and crest of nose, and a portion of the nasal septum.
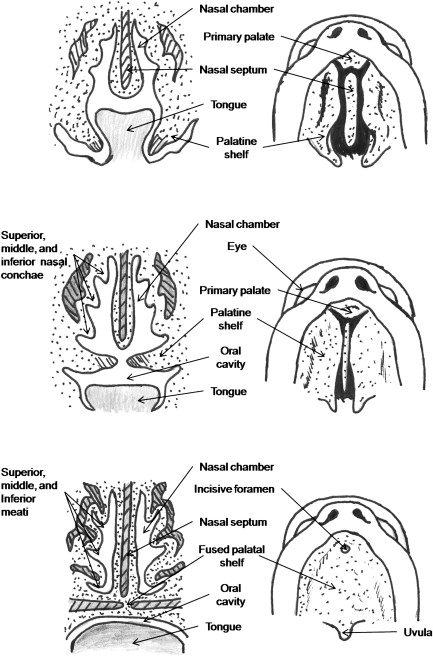
The nasal septum grows inferiorly from the nasofrontal prominence to the level of the palatal shelves following fusion to form the secondary palate ( Fig. 2 ). Anteriorly, the septum is contiguous with the primary palate originating from the nasomedial processes. The initial site of palatal fusion occurs posterior to the incisive foramen and extends both anteriorly and posteriorly. The fusion point between the primary and secondary palate is the incisive foramen (see Fig. 2 ).
At the end of its development, the nasal septum divides the nasal cavity into two separate chambers. The nasal septum’s components are the quadrangular cartilage, the perpendicular plate of the ethmoid, the vomer, the maxillary crest, the palatal crest, and the membranous septum ( Fig. 3 ).

The tubular vomeronasal organ first appears as bilateral epithelial thickening on the nasal septum. By the fortieth day of gestation, this primordial structure has invaginated along the septum. The structure thus end in a blind pouch and subsequently separates from the septal epithelium. In other species, the vomeronasal organ is lined with chemoreceptors similar to those in the olfactory epithelium. This epithelium projects into the accessory olfactory bulb, which connects to the amygdala and other limbic centers.
Lateral nasal wall embryology
At 8 weeks’ gestation, a cartilaginous nasal capsule surrounds the nasal cavity and is continuous with the cartilage of the nasal septum. Three soft tissue elevations or preturbinates can be identified within the nasal cavity. Even at this early stage, the preturbinates are oriented in size and position comparable with the adult inferior, middle, and superior turbinates (see Fig. 2 ).
By 9 to 10 weeks, the cartilage capsule develops into two cartilaginous flanges that penetrate the soft tissue elevations of the inferior and middle turbinate. A small elevation of cartilage located at the entrance to the middle meatus ultimately forms the uncinate process. This cartilage originates from the medial wall of the lateral cartilage capsule. As the uncinate begins to develop, a ridge of bone originating from the hard palate advances posteriorly to replace the lateral cartilaginous capsule and becomes the posterolateral wall of the nose.
Around 11 to 12 weeks’ gestation, the primordial ethmoidal infundubulum develops as a space lateral to the uncinate process in the middle meatus. From this space, a short tract running inferolaterally toward the maxillary bone precursor is the initial development of the maxillary sinus. As the primordial maxillary sinus grows, a vertical plate of bone extending from the primitive maxilla lengthens posteriorly to separate the lower part of the orbit from the lateral cartilaginous capsule. Additionally a second vertical bony plate extends cephalad from the hard palate and forms the posteroinferior lateral wall of the nasal cavity.
By 15 to 16 weeks’ gestation, the inferior, middle, and superior turbinates are well formed. Additionally the primordial maxillary sinus is surrounded by a sleeve of cartilage and has grown from the space lateral to the uncinate, the ethmoid infundibulum, toward the apex of maxilla inferiorly. Posterior protrusions from the ethmoid infundibulum continue to enlarge and will become the posterior ethmoid cells.
At 17 to 18 weeks’ gestation, the thick cartilage cap of the primitive maxillary sinus leads the continuing extension of the sinus anteriorly, laterally, and inferiorly. This channel runs medial to the nasolacrimal duct near its origin at the orbit. Initial ossification of the cartilaginous precursor of the inferior turbinate also occurs at the angle where the inferior turbinate budded from the lateral cartilaginous capsule. Protrusions posteriorly into the sphenoid bone are visualized. Over the next 3 to 4 weeks, ossification progresses to involve the superior aspect of nasolacrimal duct near the orbit and the middle turbinate. As with its inferior counterpart, ossification of the middle turbinate commences at its site of origin from the lateral cartilaginous capsule.
By 24 weeks’ gestation, the primordial maxillary sinus has invaginated into the woven bone of the maxilla. Laterally, a bony plate separates the channel from the orbit and medially a plate of bone separates the inferior turbinate from the lateral cartilaginous capsule. In addition, the nasolacrimal duct is firmly encased in a tube of bone superiorly near the eye.
The development of the lateral nasal wall is close to complete by 24 weeks’ gestation. By this time, the superior and middle turbinates have developed and ossified from the ethmoid bone, while the inferior turbinate has emerged from two origins, the maxilla and the lateral cartilaginous capsule. Based on the initial mucosal thickening, turbinate development appears to be a primary process, and meatal ingrowth occurs secondarily.
Lateral nasal wall embryology
At 8 weeks’ gestation, a cartilaginous nasal capsule surrounds the nasal cavity and is continuous with the cartilage of the nasal septum. Three soft tissue elevations or preturbinates can be identified within the nasal cavity. Even at this early stage, the preturbinates are oriented in size and position comparable with the adult inferior, middle, and superior turbinates (see Fig. 2 ).
By 9 to 10 weeks, the cartilage capsule develops into two cartilaginous flanges that penetrate the soft tissue elevations of the inferior and middle turbinate. A small elevation of cartilage located at the entrance to the middle meatus ultimately forms the uncinate process. This cartilage originates from the medial wall of the lateral cartilage capsule. As the uncinate begins to develop, a ridge of bone originating from the hard palate advances posteriorly to replace the lateral cartilaginous capsule and becomes the posterolateral wall of the nose.
Around 11 to 12 weeks’ gestation, the primordial ethmoidal infundubulum develops as a space lateral to the uncinate process in the middle meatus. From this space, a short tract running inferolaterally toward the maxillary bone precursor is the initial development of the maxillary sinus. As the primordial maxillary sinus grows, a vertical plate of bone extending from the primitive maxilla lengthens posteriorly to separate the lower part of the orbit from the lateral cartilaginous capsule. Additionally a second vertical bony plate extends cephalad from the hard palate and forms the posteroinferior lateral wall of the nasal cavity.
By 15 to 16 weeks’ gestation, the inferior, middle, and superior turbinates are well formed. Additionally the primordial maxillary sinus is surrounded by a sleeve of cartilage and has grown from the space lateral to the uncinate, the ethmoid infundibulum, toward the apex of maxilla inferiorly. Posterior protrusions from the ethmoid infundibulum continue to enlarge and will become the posterior ethmoid cells.
At 17 to 18 weeks’ gestation, the thick cartilage cap of the primitive maxillary sinus leads the continuing extension of the sinus anteriorly, laterally, and inferiorly. This channel runs medial to the nasolacrimal duct near its origin at the orbit. Initial ossification of the cartilaginous precursor of the inferior turbinate also occurs at the angle where the inferior turbinate budded from the lateral cartilaginous capsule. Protrusions posteriorly into the sphenoid bone are visualized. Over the next 3 to 4 weeks, ossification progresses to involve the superior aspect of nasolacrimal duct near the orbit and the middle turbinate. As with its inferior counterpart, ossification of the middle turbinate commences at its site of origin from the lateral cartilaginous capsule.
By 24 weeks’ gestation, the primordial maxillary sinus has invaginated into the woven bone of the maxilla. Laterally, a bony plate separates the channel from the orbit and medially a plate of bone separates the inferior turbinate from the lateral cartilaginous capsule. In addition, the nasolacrimal duct is firmly encased in a tube of bone superiorly near the eye.
The development of the lateral nasal wall is close to complete by 24 weeks’ gestation. By this time, the superior and middle turbinates have developed and ossified from the ethmoid bone, while the inferior turbinate has emerged from two origins, the maxilla and the lateral cartilaginous capsule. Based on the initial mucosal thickening, turbinate development appears to be a primary process, and meatal ingrowth occurs secondarily.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


