Nasal Reconstruction
Stephen S. Park
Nasal reconstruction has evolved significantly from early, rudimentary attempts to provide covering for large nasal defects. In contemporary nasal reconstruction, surgeons combine a mastery of aesthetics and surgical techniques, to create a nose that is visually inconspicuous and functionally stable. This is expected to hold up throughout the life of the patient. Ancient methods focused on using soft tissue to fill the cavity, with little regard for structural framework, internal lining, intranasal airspace, and intrinsic contours. Nasal reconstruction in the 21st century has raised the bar to a level where the new nose may go unnoticed by the casual observer, nasal function returns to the baseline, and the patient integrates back into society without undue self-consciousness.
HISTORY OF NASAL RECONSTRUCTION
The history of nasal reconstruction dates back to antiquity when, during the fourth Egyptian dynasty (2575-2467 bc), prostheses were molded for the deceased, because “only those without physical disfigurement would enter the Kingdom of Osiris” (1). Reconstruction came into greater demand with the rise of nasal mutilation as a common form of humiliation or punishment. Around 1500 bc, when Prince Lakshmana of India deliberately amputated the nose of Lady Surpunakha, King Ravana arranged for the reconstruction of Lady Surpanakha’s nose by his physicians, documenting one of the earliest accounts of nasal restoration in human history (2, 3). Sushruta Samhita, an ancient Indian Sanskrit written during the Vedic period (600-1000 bc), describes nasal reconstruction as performed by a caste of Indian potters, using cheek tissue to cover the nasal defect (4). Early descriptions of using forehead tissue to repair a nasal defect exist in writings by the Kangiara family from 1440 ad (5). Despite the long history with this type of reconstruction, very little international exchange occurred because of the lack of maritime commerce and little communication between Europe and Asia during that period. In the 16th century, Gusparo Tagliacozzi described his success with a two-staged method of nasal reconstruction using a pedicled, cutaneous flap from the upper arm, based on the brachial vessels. This was followed by attempts with pedicled flaps from other individuals, especially slaves. Outcomes were obviously discouraging, and further progression was shortly abandoned.
In 1794, the first description of the Indian forehead flap in the English language was published in the Madras Gazette and later reproduced in Gentleman’s Magazine (6). Joseph Carpue (7), an English general surgeon, is credited with the introduction of this forehead flap to the Western world when he described his experience with two successful “Indian forehead flaps” for nasal reconstruction. Subsequently, the classic forehead flap for nasal reconstruction became widespread throughout the globe and defined the standard method of repair during the early 19th century. This “classic” Indian median forehead flap was based on bilateral supratrochlear arteries with a wide pedicle that could not extend beyond the level of the brows. The wide base limited the rotation and length of the forehead flap. This limitation became more evident when it was recognized that intranasal lining left to heal by second intention resulted in significant distortion, contracture, and nasal obstruction. This restricted design could not be designed to line the intranasal defect.
Pedicled flaps moved slowly to the United States; the first American reports of forehead flaps for nasal reconstructions are from the 1940s (8, 9). These early flaps were traditional “median” forehead flaps with wide pedicle bases capturing both supratrochlear vessels. Kazanjian and Converse believed that the paired arteries were needed to adequately perfuse the forehead flap. Because of the limited length of this early median forehead flap, many variations were described, largely aimed at mobilizing more tissue with greater flap length: “Gillies’ up-and-down flap” (10), “New’s sickle flap” (11), “Converse’s scalping
flap” (12), and the “Washio flap” (13). In spite of the variety of flaps attempted, none have stood the test of time primarily because of the poor quality of scalp skin in contrast to forehead skin and the significant donor site morbidity.
flap” (12), and the “Washio flap” (13). In spite of the variety of flaps attempted, none have stood the test of time primarily because of the poor quality of scalp skin in contrast to forehead skin and the significant donor site morbidity.
Millard repopularized the paramedian flap with a “seagull” design for resurfacing the nose (14, 15, 16, 17). The primary advantage of this paramedian flap was the narrow pedicle base, which allowed for an improved arc of rotation. The inferior reach of the flap could be further extended by basing the pedicle below the level of the brow. This design created less narrowing of the brows in contrast to the original “median” forehead flap. Millard also noted that the supratrochlear artery traveled in a plane between the skin and frontalis muscle, and, consequently, the frontalis muscle could be selectively trimmed off the undersurface of the flap without jeopardizing flap vascularity. Gary Burget and Fred Menick (18) have since refined these concepts of the paramedian forehead flap design and have brought nasal reconstruction to its higher standards.
ETIOLOGY OF NASAL DEFECTS
Defects of the nose arise from a large array of causes, and, on many occasions, it is worthwhile to consider the specific etiology as it may impact the method of repair. The nose is the most common site for de novo cutaneous malignancies. Basal cell carcinomas predominate, and there are histologic subtypes with varying degrees of aggressiveness. The nodular subtype is most common, as characterized by a circumscribed growth pattern, and carries the most favorable prognosis. Aggressive histologic subtypes, such as the morpheaform or infiltrating, can develop small nest patterns and are more likely to involve the internal lining or to recur following surgical excision. These latter subtypes are best treated with Mohs surgery. Squamous cell carcinoma is the second most common type and also behaves aggressively, with a greater incidence of regional metastasis. Melanoma is the most serious skin tumor, warranting an aggressive surgical intervention. Recurrent skin tumors or tumors that have been previously irradiated have a less predictable vascular anatomy, which may impact flap design and closure options. Vascular and adnexal tumors of the nose are less common but often require more aggressive treatment plans. Sharp and blunt trauma to the nose, such as from motor vehicle accidents, can lead to nasal defects with associated variables for consideration. Animal or human bites are grossly contaminated, and a delay in repair is often advocated. This dogma arises from experience with extremity injuries; however, the face is characterized by such a robust vascularity that immediate repair will often be successful.
NASAL ANATOMY
A firm understanding of the normal nasal anatomy is a prerequisite for mastery of nasal reconstruction. The biomechanics of covering flaps, the importance of a firm framework, and the anatomic basis for internal lining repair are imperative concepts as one proceeds through the algorithm of reparative options.
The external nasal skin is variable at different areas of the nose, being thick at the nasion and tip and extremely thin along the rhinion. The thin epithelial sleeve along the alar rim and nasal facets makes these areas especially vulnerable to notching and contour irregularities following reconstruction.
There are four layers of soft tissue between the skin and the nasal skeleton—the superficial fatty panniculus, fibromuscular layer, deep fatty layer, and, finally, the periosteum or perichondrium. The superficial fatty panniculus is located immediately below the skin and consists of adipose tissue with interlacing vertical fibrous septi coursing from the deep dermis to the underlying fibromuscular layer. The fibromuscular layer contains the intrinsic nasal musculature and the nasal superficial musculoaponeurotic system (SMAS), which is a continuation of the facial aponeurotic system. The deep fatty layer located between the SMAS and the thin covering of the nasal skeleton contains the major superficial blood vessels and nerves. The periosteum of the nasal bones extends over the upper lateral cartilages and fuses with the periosteum of the piriform process laterally (19). Perichondrium covers the nasal cartilages, and dense fibrous interconnections can be found between the paired tip cartilages. Between the framework and the deep fatty layer is a plane of loose areolar tissue that is free of fibrous septa, making it an ideal plane for dissection and elevation of the soft tissue envelope.
The nasal musculature of the nose is well defined, with greatest activity along the junction of the upper lateral and alar cartilages (20). This allows for muscular dilation and stenting of the functionally critical nasal valve area. All nasal musculature is innervated by the zygomatic division of the facial nerve (21).
The nasal blood supply is via a predictable and consistent network of named vessels through both the internal and external carotid systems. The angular artery branches from the facial artery and is a discrete landmark along the nasofacial junction. Feeder vessels off the angular artery perforate the levator labii superioris and provide the vascular basis for the design of melolabial flaps. A medial branch off the angular artery, the lateral nasal artery, supplies the lateral surface of the caudal nose. This lateral nasal artery courses in the sulcus between the ala and nasal sidewall and is covered by the levator labii superioris alaeque nasi. It arborizes multiple times to enter the subdermal plexus covering the nostril and cheek and is the anatomic basis for many small local flaps within the lateral nasal wall, for example, bilobe flaps. The dorsal nasal artery, a branch of the ophthalmic artery, pierces the orbital septum above the medial palpebral ligament and travels inferiorly along the side of the nose to anastomose with the lateral nasal artery. The dorsal nasal artery provides a rich axial blood supply to the dorsal nasal skin and serves
as the main arterial contributor to dorsal nasal flaps. The columella and tip are supplied by the paired columellar arteries, branches of the superior labial artery. The external nasal branch of the anterior ethmoidal artery, a branch of the ophthalmic artery, pierces bone on the medial wall of the orbit at the point where the lamina papyracea of the ethmoid bone articulates with the orbital portion of the frontal bone (frontoethmoid suture). The vessel enters the ethmoid sinuses to supply the mucosa and sends branches to the superior aspect of the nasal cavity. The external nasal branch of the anterior ethmoidal artery emerges between the nasal bone and the upper lateral cartilage to supply the skin covering the nasal dorsum and tip.
as the main arterial contributor to dorsal nasal flaps. The columella and tip are supplied by the paired columellar arteries, branches of the superior labial artery. The external nasal branch of the anterior ethmoidal artery, a branch of the ophthalmic artery, pierces bone on the medial wall of the orbit at the point where the lamina papyracea of the ethmoid bone articulates with the orbital portion of the frontal bone (frontoethmoid suture). The vessel enters the ethmoid sinuses to supply the mucosa and sends branches to the superior aspect of the nasal cavity. The external nasal branch of the anterior ethmoidal artery emerges between the nasal bone and the upper lateral cartilage to supply the skin covering the nasal dorsum and tip.
The venous drainage of the external nose is through corresponding vessels, leading into the facial vein, the pterygoid plexus, and the valveless ophthalmic veins. The intranasal mucosa has a similar number of named vessels, and they are critical when designing mucosal flaps for full-thickness nasal defects. The septal branch of the superior labial artery is a dominant feeder to the septal mucosa. In fact, a flap of the entire septal mucosa, back to the sphenoid sinus, can be based on this single vessel. The anterior and posterior ethmoidal vessels supply the superior portion of the septum. Terminal branches of the anterior ethmoidal artery cover the dorsal nasal septum, a critical region for the swinging, composite septal flaps used for internal lining and structure. Terminal branches of the sphenopalatine artery supply the posterior septum and posterior lateral nasal wall. The vasculature of the internal nose is the anatomic basis for complex nasal reconstruction.
The sensory nerve to the nasal skin is via the ophthalmic and maxillary divisions of the fifth cranial nerve. Branches of the supratrochlear and infratrochlear nerves supply the skin covering the radix, rhinion, and cephalic portion of the nasal sidewalls. The external nasal branch of the anterior ethmoidal nerve supplies the skin over the caudal half of the nose. The infraorbital nerve provides sensory branches to the skin of the lateral aspect of the nose.
The structural framework of the nose is composed of the paired nasal bones to the upper third, the nasal septum and upper lateral cartilages to the middle vault, and the paired lower lateral cartilages within the nasal tip. Dorsal support to the middle vault is primarily achieved through the rigidity of the cartilaginous septum and, to a lesser extent, the paired upper lateral cartilages. Their fusion at the midline is important clinically because of the tendency for the upper lateral cartilages to progressively contract intranasally and lead to obstruction. If a disarticulation between the septum and upper lateral cartilages occurs, the middle vault should be diligently reconstructed.
The tip is supported by the overall size and strength of the lower lateral cartilages, their ligamentous attachments to the caudal septum, the scroll with the upper lateral cartilages, and the adherence to the overlying soft tissue. Each lower lateral cartilage is subdivided into the medial, intermediate, and lateral crura. The shape, length, and angulation of the intermediate crura determine the external morphology of the tip lobule and the position of the tip-defining point. Disruption or weakening of the lateral crus predisposes to alar retraction and notching, an important consideration in nasal reconstruction when these structures may have been compromised. Laterally, small sesamoid cartilages are interconnected by a dense, fibrous connective tissue.
The alar lobule and nasal sidewall is a functionally pivotal area of the nose that is not often highlighted during rhinoplasty discussions but has a critical role during reconstructive surgery. This keystone region is located between the lateral border of the lower lateral cartilage and the bony piriform aperture. Externally, it corresponds to the supra-alar crease and is the most common location for a clinically significant, dynamic valve collapse. Beneath the skin, the area consists of a firm, fibrous-fatty aponeurosis, an occasional sesamoid cartilage, and a portion of the transverse nasalis muscle. Typically, this histologic architecture provides sufficient rigidity to prevent collapse during inspiration. If compromised, nasal function will be impaired unless it is aggressively restored with liberal grafting in a nonanatomic fashion. The internal nasal valve is a distinct area defined by the dorsal septum medially, upper lateral cartilage superolaterally, and the head of the inferior turbinate inferomedially. The external nasal valve is the cross-sectional area under the alar lobule proper. It does not entirely correlate with the lateral crus of the lower lateral cartilages. The alar rim does not have cartilage within it, and collapse or notching can readily occur. To avoid this, structural grafts to the alar rim are often needed. The junction between the ala and cheek forms an acute angle and is difficult to reconstruct; most repairs heal with gradual effacement of that alar-facial angle and may become increasingly conspicuous. If at all possible, one should try to preserve the alar-facial junction and keep incisions slightly onto the nose. The limen vestibuli is the junction between the internal nasal lining and the stratified squamous epithelium of the nose. It does not lie at the caudalmost border of the alar lobule but rather slightly intranasally, within the vestibule. Reconstruction of full-thickness defects of the alar rim should keep this in mind and allow the resurfacing flap to roll inward before suturing to the internal lining flap.
There is a bony piriform platform that surrounds the nose, and its role in tissue support is often poorly appreciated. The nasal sill, anterior nasal spine, and medial maxilla (including the frontal process of the maxilla) provide an essential platform for the nose, and resection of these structures will require a separate repair, such as with a split calvarial bone graft. Failure to rebuild this platform will often result in a soft tissue collapse and facial asymmetry.
DEFECT ANALYSIS
Analyzing a given defect and arriving at the ideal method of repair is a challenging and rewarding exercise. On occasion, the “correct” flap will be intuitive, as it appears to
define itself. At other times, it can be a creative dilemma as one struggles to visualize the incisions, flap transfer, surrounding vectors of tension, and final scars. This mental challenge requires a dynamic, three-dimensional image of the nasal repair. At times, it is worthwhile to have a structured algorithm for defect analysis. Although it does not necessarily define the ideal flap, it can be very useful in avoiding errors in design. In particular, the line of questioning can guide one away from creating disfiguring mistakes such as eyelid retraction or an unnatural hairline. Once flaps are elevated and transposition is attempted, the reconstruction is committed; this is clearly not the time to discover a gross design flaw.
define itself. At other times, it can be a creative dilemma as one struggles to visualize the incisions, flap transfer, surrounding vectors of tension, and final scars. This mental challenge requires a dynamic, three-dimensional image of the nasal repair. At times, it is worthwhile to have a structured algorithm for defect analysis. Although it does not necessarily define the ideal flap, it can be very useful in avoiding errors in design. In particular, the line of questioning can guide one away from creating disfiguring mistakes such as eyelid retraction or an unnatural hairline. Once flaps are elevated and transposition is attempted, the reconstruction is committed; this is clearly not the time to discover a gross design flaw.
For every cutaneous defect, there are six questions that are reviewed prior to the first incision (Table 177.1):
1. Immobile structures. What surrounding landmarks must not come under any tension during flap transposition, such as the eyelid, alar margin, or upper lip? It does not necessarily mean that tissue cannot be recruited from that region but rather, adequate structure must be available in the area to fully support the adjacent flap. A common example is a cheek flap that risks lower-eyelid retraction and is vertically supported with anchors to the infraorbital rim. For the nose, there are three “immobile structures”: the alar rim, nasal base symmetry, and lateral nasal wall. The immobility of the lateral nasal wall is a unique concept. Most flaps are thought of in two dimensions. The nose, as a threedimensional structure, has an important lumen. The additional vector of tension is in this third dimension, perpendicular to the cutaneous plane. Local flaps tend to create a force perpendicular to the plane of rotation, leading to sidewall collapse and functional compromise. Recognition of this concept allows one to plan the reconstruction with prophylactic support grafts.
2. Area of recruitment. Given which surrounding areas are “immobile,” from where can tissue be recruited without distorting those areas? Also, in what direction do the lines of maximal extensibility exist and how can the flap be designed to slide parallel with them?
3. Facial lines. There are numerous descriptions of facial lines that can assist with flap selection and design. Langer lines were first described by Langer (19) in 1861 as a recommendation for orienting elliptical skin excisions. Circular defects in postmortem patients became elliptical as rigor mortis ensued, and these lines were mapped throughout the body. Clinical practice has shown that these lines do not always orient along lines for optimal healing. Relaxed skin tension lines (RSTLs) more accurately reflect the intrinsic tension within the dermis while at rest. Wounds heal under less tension when oriented along them, and they can usually assist with flap design. Lines of minimal tension (also known as skin creases) are defined by the repeated contraction of the underlying muscle as they permanently orient elastin and collagen fibers within the dermis. These lines usually run parallel with the RSTLs, but the supratip, glabella, and lateral canthal regions are in conflict. It is usually recommended to incise along lines of minimal tension rather than RSTLs.
TABLE 177.1 DEFECT ANALYSIS | |
|---|---|
|
The other “facial lines” that exist in the face are those created by the borders of aesthetic units and the subunits of the nose. The principle of aesthetic units is based on the fact that the human eye can only perceive things as a series of block images, thus our inability to scan a horizon without a saccadic motion. The face, or nose, is visualized as a discrete set of block images that are put together subconsciously and interpreted as a single image. These images are defined by predictable reflections of light, natural creases, and undulations in cutaneous topography. The nose has subunits defined as the nasal tip, dorsum, columella,
paired ala, sidewalls, and soft tissue facets (Fig. 177.1). Scars that are strategically placed at the border of two units will be less conspicuous than those resting within one. In order to achieve this, one usually has to modify the size/shape of the original cutaneous defect. The aesthetic subunits may require modifications with some patient groups who have other unique nasal characteristics. At times, a patient may have a significant transition from one skin type to another within the nose, such as individuals with rosacea or a rhinophyma (20).
paired ala, sidewalls, and soft tissue facets (Fig. 177.1). Scars that are strategically placed at the border of two units will be less conspicuous than those resting within one. In order to achieve this, one usually has to modify the size/shape of the original cutaneous defect. The aesthetic subunits may require modifications with some patient groups who have other unique nasal characteristics. At times, a patient may have a significant transition from one skin type to another within the nose, such as individuals with rosacea or a rhinophyma (20).
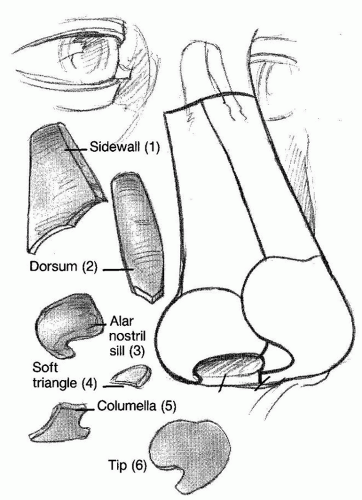 Figure 177.1 Nasal aesthetic subunits. |
4. Resultant scars. One should anticipate the final scars for each proposed flap and how they relate to preexisting facial lines. At times, this exercise is not intuitive, such as the resultant scars of a rhombic flap. This question forces the surgeon to try different orientations of flap design that might yield more favorable scars while still abiding by the previous tenets of immobile structures and area of recruitment.
5. Function. During the defect analysis, one of the essential considerations is the location in terms of function and potential lateral wall collapse. A cutaneous defect involving the critical area along the supra-alar crease will place the nasal airway at jeopardy even if the original defect does not violate native cartilage. This critical “red zone” must alert the reconstructive surgeon of the need for structural reinforcement in the form of cartilage grafting. Anatomically, it corresponds to the fibroareolar tissue immediately lateral to the lateral crus of the lower lateral cartilage and is distinct from the precise internal and external nasal valves. Similarly sized defects along the dorsum or upper third do not have the associated functional concerns.
6. Depth. Assessing the depth of the nasal defect is important to determine if any structural cartilage or bone is missing and to explore the internal nasal lining. Any violation of the intranasal mucosa must be recognized preoperatively, as it will alter the reconstructive plan significantly; all missing lining must be meticulously repaired prior to grafting and resurfacing. Failure to do so will risk contracture, lumen stenosis, graft exposure and resorption, and alar notching.
SMALL CUTANEOUS DEFECTS
Cutaneous defects of the nose can be found in a variety of sizes, depths, and shapes. Intuitively, the smaller ones should be more straightforward in terms of repair, but that is often not the case. Whereas large defects have a limited number of options, those less than 1.5 cm can be repaired with an array of flaps and grafts, often creating a greater intellectual challenge. Furthermore, patient expectations are generally higher with small lesions, and even small irregularities that often plague these repairs can be problematic, such as alar base asymmetry, notching, conspicuous scars, pincushioning, or valve collapse.
Pertinent Anatomy
Nasal topography during reconstruction is often discussed in terms of aesthetic subunits, but since smaller defects frequently involve only small portions of an individual site, it is more practical to discuss the defect in terms of the upper, middle, and lower thirds of the nose. The upper third has relatively thin skin except for the nasion region, where the subcutaneous tissue is much more prominent. The lateral borders are adjacent to the medial canthus and represent immobile regions that cannot be distorted, especially from contracture during second-intention healing. The area of recruitment is primarily from the glabella and, to a lesser extent, from the nasal dorsum. There is little functional concern with defects in this zone.
The middle third of the nose has skin that is thin medially but thicker laterally. Whereas the upper lateral cartilages support the medial portion of this zone, the lateral aspect has support only from fibroareolar tissue without native cartilage. Tissue can be recruited from multiple directions, but any vertical vector must be minimal, as ala or tip elevation can quickly occur. Functional implications are important along the lateral aspect of the middle vault, even if no native cartilage has been violated. The lateral nasal artery is found immediately cephalad to the supra-alar crease and is the basis for many local flaps of the nose.
The lower third of the nose consists of the nasal tip, alar lobule, columella, and soft tissue triangle. The skin is typically thicker and more sebaceous, leading to less favorable wound healing. Most defects of this region are repaired with tissue recruited from the middle vault, but great care must go into flap design and the subsequent vectors of tension. This zone is significant for its free alar margin and the fact that small degrees of wound contracture may lead to retraction and gross alar base asymmetries. The supra-alar crease and alar-facial junction are important natural landmarks that should be preserved or recreated. The alar lobule proper does not contain native cartilage, and disruption to this area predisposes to a dynamic external nasal valve collapse. Consequently, nonanatomic cartilage grafting is essential to prevent alar rim retraction and collapse.
SELECTION OF GRAFTS AND FLAPS
At times, the simplest method of repair is also the preferred one in terms of optimal aesthetic results. Second-intention healing, skin and composite grafts, and local flaps all enter the algorithm for repair of such defects, and proper selection becomes the cornerstone for a successful outcome (Table 177.2) (21). Individuals with a large nose, prominent hump, or broad nasal tip can have their nose reduced slightly, and it will not only create more tissue for recruitment but also reduce the relative size of the defect. The use of common aesthetic rhinoplasty maneuvers in the setting of nasal reconstruction can be a powerful tool. Hump reduction, cephalic trim, tip sutures, etc., all can have great
utility with medium size nasal defects. For many defects, this maneuver can allow the transition from a more complex repair to a simpler one with local flaps or grafts.
utility with medium size nasal defects. For many defects, this maneuver can allow the transition from a more complex repair to a simpler one with local flaps or grafts.
TABLE 177.2 COMMON RECONSTRUCTIVE OPTIONS FOR SMALL CUTANEOUS DEFECTS | ||||||
|---|---|---|---|---|---|---|
|
Upper Third
Smaller defects in this zone are readily repaired with either a full-thickness skin graft or by second-intention healing. Those larger than 1.5 cm can be resurfaced with a sliding glabellar or Rieger flap (22). Other transposition flaps recruited from the forehead and middle third of the nose are less common alternatives.
Middle Third
Small midline defects are often amenable to primary closure with wide undermining and recruitment from lateral nasal tissue; this often represents the first option for optimal repair. It will leave a vertically oriented central scar with tension evenly distributed, thus maintaining nasal symmetry. Many times, a medium-sized defect in the midline can be converted to a small defect with partial closure through bilateral advancement flaps, leaving a residual defect in the midline. The remainder can be resurfaced with a full-thickness skin graft, harvested from the standing cutaneous deformities of the primary closure. This skin is ideally suited for this because of the excellent color/texture match and lack of donor site morbidity. Small transposition flaps (rhombic, bilobe, rotation) are frequently utilized and represent another workhorse repair for this region. Skin grafts can blend in well with the thin skin of this zone, but even small contour depressions are difficult to disguise, as their shadows often remain conspicuous. If a cartilage graft is needed along the lateral wall, a vascularized resurfacing flap is needed. Those larger than 1.5 cm often require a more elaborate flap.
Lower Third
Precise midline defects are ideally suited for primary closure, particularly when the premorbid nasal tip is somewhat bulbous and can afford to be narrowed. Like the middle vault, partial closure with skin grafting from the standing cutaneous deformity is a useful technique. A bilobe flap is often utilized for defects of the nasal tip, allowing the tension to be distributed more widely and at an adequate distance from the free alar margin. The alar lobule is often repaired with composite grafts, restoring structure and covering simultaneously. Smaller defects limited to the supraalar crease can do well through second-intention healing, but moderately sized defects will jeopardize nasal patency. The single-stage melolabial flap can also be used; however, the supra-alar crease is often obliterated and asymmetry can result if the contralateral supra-alar crease is deep and prominent. A two-stage, interpolated melolabial flap is preferable for larger defects of the alar lobule, especially when cartilage grafts have been placed and the aesthetic unit completed. Small, full-thickness defects involving the alar margin are best repaired with a three-layered composite graft from the ear, whereas larger ones require a multilayered reconstruction involving the internal lining, structural framework, and resurfacing. The columella is characterized by a very narrow column of thin skin and lends itself well to small composite and skin grafts. For larger columellar defects, structural grafting along with a pedicled melolabial flap is most often used. The soft tissue triangle defect is ideally restored by allowing second-intention healing to occur with a natural-appearing web.
TECHNIQUES FOR GRAFTS AND FLAPS
Second-Intention Healing
Local wound care is the most important aspect when selecting this method of repair. Keeping the wound bed moist and preventing the development of a dry eschar will encourage the most prompt and favorable healing. Cytotoxic agents, especially hydrogen peroxide, should be avoided. A guiding suture can be employed in a similar fashion to the purse-string closures used for large defects on the scalp and face. This guiding suture partially closes a small defect and allows the remainder to heal secondarily. The greatest utility of this suture is for small defects along the alar rim. The suture can be placed horizontally, thus converting the circular defect into a vertical elliptical shape, which resists the vertical contracture that will ensue. The suture itself will often notch the alar rim inferiorly slightly, but it contracts to a normal position during healing. The suture is removed after 2 to 3 weeks. This technique will allow more defects to be managed in a conservative fashion.
Skin and Composite Grafts
Superficial defects can be immediately repaired with full-thickness skin grafts and perform well (Table 177.3). For deeper defects, or those exposing bare cartilage, it may be prudent to delay the repair for 10 days allowing a layer of granulation tissue to accumulate within the recipient bed. This enhances vascularity and fills in the depression, thereby improving surface contour. The defect shape is modified, in order to create straight lines with square corners, rather than leaving a circular defect. The entire aesthetic subunit is not necessarily completed. Wound margins are beveled toward the center of the defect in order to smooth the transition between graft and the native nasal skin. Skin grafts can be harvested from the supraclavicular fossa, periauricular skin, and melolabial area. Graft thickness is modified following harvest to best match the surrounding skin texture, especially along the nasal tip, where thicker skin is found. Small “pie crusts” can be cut into the graft to allow the egress of serous fluid, recognizing that these perforations often become discolored and remain noticeable. A bolster dressing is rarely needed on the nose as long as small tacking sutures are placed to maintain close apposition between the graft and recipient bed.
A two- or three-layered composite graft is usually taken from the ear—either the root of the helix, the conchal bowl, or the triangular fossa. Anterior auricular skin is tightly adhered to auricular cartilage and has a good success rate. The shape of the cartilage is usually concave toward the skin, and although this shape can be unfavorable for external resurfacing, it is ideal for internal lining. The auricular donor site is closed primarily with little distortion. Excising cartilage from the apices of the donor site can avoid the “cookie bite” deformity to the ear. The composite graft must be securely attached to the nose, often with through-and-through sutures or a small bolster. These grafts are ideally suited for defects along the alar rim and columella (Fig. 177.2). Many composite grafts will appear moderately dusky for a week but will usually recover during the ensuing days. Larger grafts may undergo a degree of epidermolysis, which will lead to a less favorable color and texture match. Three-layered composite grafts are kept less than 1.5 cm because the sole blood supply is from the peripheral margin. Two-layered composite grafts, on the other hand, can be designed larger because the nourishing bed is the entire surface area of the graft. When utilizing these larger, two-layered composite grafts, one can excise several small, 2-mm punch holes through the cartilage only, taking care not to puncture the overlying skin. These small perforations will allow granulation tissue to penetrate the cartilage and nourish the epithelial covering.
TABLE 177.3 PEARLS FOR SKIN AND COMPOSITE GRAFTS | |
|---|---|
|
Primary Closure
Primary closure with wide undermining is an excellent option for many small cutaneous nasal defects, especially those located in the precise midline of the lower two-thirds of the nose and when the tip is modestly wide or bulbous to begin with. Lateral undermining over the perichondrium, and deep to the nasal SMAS layer, is essential. The elliptical design requires that the vertical apices extend further superiorly and inferiorly than the traditional 30-degree angles, in order to avoid an asymmetric narrowing of the nose. Failure to do so will narrow the nose at the site of the original defect while leaving the supratip or infratip segments disproportionately wide. Common rhinoplasty maneuvers, such as an interdomal suture and cephalic trim, are frequently utilized concomitantly in order to narrow the tip, reduce wound tension, and facilitate primary closure. These bilateral advancement flaps are very useful for medium-sized defects that are partially closed and convert the defect to a smaller one. The remainder is resurfaced with a full-thickness skin graft from the standing cutaneous deformities of the local flaps (Fig. 177.3A-H).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


