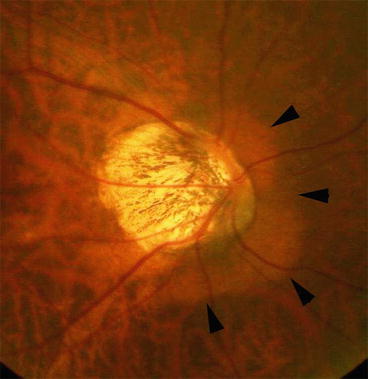
Fig. 6.1
Various appearance of optic disc in eyes with pathologic myopia. (a and b) Optic disc area is enlarged and shows ‘megalodisc’ appearance. (c and d) Optic disc is small and tilted
The recent advance in ocular imaging, especially optical coherence tomography (OCT), has enabled us to visualize the deep structures on and around the optic nerve. By using swept-source OCT and 3D MRI, we identified various findings which are considered to be caused by mechanical stretching around the optic nerve in eyes with pathologic myopia. These results prompted us to consider that at least in some patients, a mechanical damage on and around the papillary region might play an important role in developing the VF damage in highly myopic eyes. Thus, there might be a condition which should be called as “myopic optic neuropathy” [1]. This chapter describes how the papillary and peripapillary regions are mechanically altered in eyes with pathologic myopia and how such abnormalities could possibly relate to the VF defects.
6.2 Optical Coherence Tomography (OCT) Findings of Papillary and Peripapillary Region of Eyes with Pathologic Myopia
6.2.1 Dilation of Perioptic Subarachnoid Space (SAS) and Thinning of Peripapillary Sclera
Recently, due to an advancement of OCT, like enhanced depth imagin (EDI)-OCT and swept-source OCT, it has been possible to visualize the deep structure in the optic nerve.
Park et al. [2] used EDI-OCT and observed the SAS around the optic nerve in 25 of the 139 glaucomatous eyes (18 %). Most of the 25 eyes had high myopia and extensive parapapillary atrophy. We [3] used swept-source OCT and found that SAS was found in 124 of 133 highly myopic eyes (93.2 %) but not in the emmetropic eyes. The SAS appeared to be dilated in highly myopic eyes. In the B-scan images, the SAS was triangular, with the base toward the eye surrounding the optic nerve in the region of the scleral flange (Fig. 6.2). There was a change in the scleral curvature at the attachment of the dura mater of the SAS to the peripapillary sclera. This shows that the distance between the point which the sclera was divided into the dura mater and the optic nerve increased in highly myopic eyes, as suggested by Okisaka [4] based on his histological evaluations. Only the nerve fiber layer and the scleral flange were observed on the SAS, consistent with a histological study by Jonas et al. [5]. The width of the SAS ranged from 263 to 1850 μm in our study. Jonas et al. [5] reported that the mean length of the scleral flange was 1.67 ± 0.74 mm in histological evaluation of 36 human globes with an axial length longer than 26.5 mm. In our study using swept-source OCT, the shortest distance between the inner surface of lamina cribrosa and SAS was 252.4 ± 110.9 μm, and the thinnest region of peripapillary sclera above SAS (scleral flange thickness) was 190.6 ± 51.2 μm [3]. Jonas [6] reported that the shortest distance between inner lamina cribrosa surface and SAS in non-highly myopic eyes without glaucoma was 557.9 ± 172.1 μm in histological evaluation.
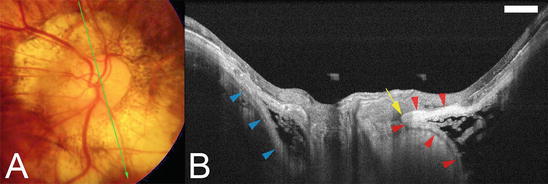
Fig. 6.2
Swept-source OCT images of subarachnoid space (SAS) around the retrobulbar optic nerve. (a) Large conus is found around the myopic optic disc. (b). Swept-source OCT slice scanned along the green line in (a) shows the SAS as a hyporeflective space along both the upper and lower borders of the ON. The SAS is triangular, with the base toward the eye. The peripapillary sclera is continuous with the pia mater along the inner boundary of the SAS (red arrowheads). The SAS protrudes toward the ON at the transition point of the peripapillary sclera and the pia mater (arrow). The peripapillary sclera is also continuous with the dura mater along the outer boundary of the SAS (blue arrowheads). The arachnoid trabeculae are seen as wide, linear streaks within the SAS (Reproduced from reference number [3] with permission)
The expanded area of exposure to CSF pressure along with thinning of the posterior eye wall may influence staphyloma formation and the way in which certain diseases, such as glaucoma, are manifested. In one of our myopic patients, there appeared to be a direct communication between the intraocular cavity and SAS through pit-like pores (Fig. 6.3). The clinical significance of a direct communication between intraocular space and SAS is not clear. This communication could cause a disrupted integrity of peripapillary sclera and changes of concentrations of materials in intraocular space and SAS. However, the translaminar pressure becomes theoretically zero, which might act favorably for the progression of VF defects.
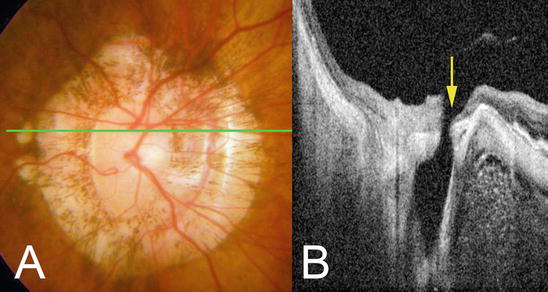
Fig. 6.3
Fundus photograph and swept-source OCT images showing direct communication between the intraocular space and the SAS. (a) Color fundus photograph of the optic disc showing a large annular conus. (b).On OCT section across green line in (a) shows that vitreous cavity is continuous with SAS through pitlike pores (arrow) (Reproduced from reference number [3] with permission)
These OCT findings are compatible with earlier histological observations. Curtin [7] described that a dilation of perioptic subarachnoid space (SAS), eversion of the inner aspect of the scleral canal, anterior displacement of the lamina cribrosa, and marked degrees of supertraction are especially specific to the highly myopic globe. Compared with the normal disc anatomy, staphyloma development has produced a marked thinning of the posterior sclera. The involvement of the innermost scleral fibers of the posterior foramen in the distention process causes the lamina cribrosa to advance toward the retinal surface. Okisaka [8] reported that in emmetropic eyes the perioptic SAS was narrow and the SAS blindly ended at the level of lamina cribrosa. The dura of the SAS was attached to the peripapillary sclera just around the lamina cribrosa. In contrary, in highly myopic eyes, the perioptic SAS was enlarged together with an increase of the axial length. In a cross section of the optic nerve, the SAS showed an inversely triangular shape whose base was toward the eye. In parallel to the dilation of SAS, the dura attachment site was markedly away from the optic nerve margin.
6.2.2 Formation of Acquired Pits in the Optic Disc Area and in the Conus Area
By using swept-source OCT, Ohno-Matsui et al. found that the optic nerve pits were not uncommon in highly myopic eyes [9]. Pit-like clefts were found at the outer border of the optic nerve or within the adjacent scleral crescent in 32 of 198 highly myopic eyes (16.2 %) but in none of the emmetropic eyes. The pits were located in the optic disc area (optic disc pits) in 11 of 32 eyes and in the area of the conus outside the optic disc (conus pits) in 22 of 32 eyes. The optic disc pits existed at the inferior or superior edge of the optic disc (Fig. 6.4). Conus pits were observed in eyes with type IX staphyloma and were present nasal to the scleral ridge or outside the ridge temporal to the nerve (Fig. 6.5). The optic disc pits were associated with discontinuities of the lamina cribrosa, whereas the conus pits appeared to develop from a scleral stretch-associated schisis or to emissary openings for the short posterior ciliary arteries in the sclera. The nerve fiber tissue overlying the pits was discontinuous at the site of the pits, and this discontinuity might be related to VF loss of highly myopic patients.
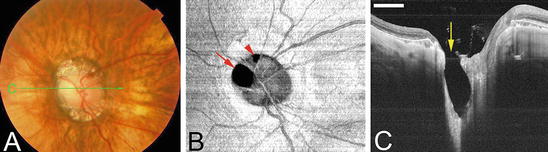
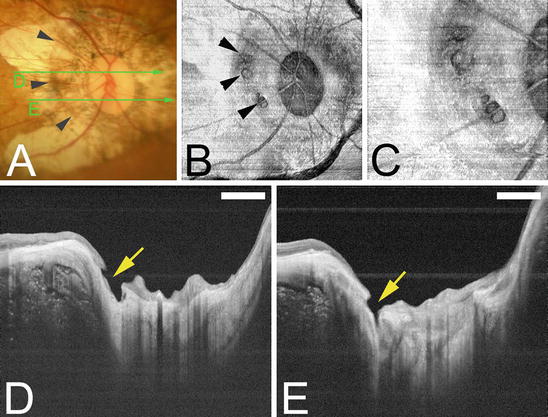
Fig. 6.4
Deeply excavated pit-like structures in the optic disc area. Bar; 1 mm. (a) Photograph of the left fundus shows horizontally oval optic disc and surrounding conus. The green line shows the area scanned by swept source OCT for the images shown in c. (b) En face view of the optic disc reconstructed from three-dimensional swept source OCT images shows one large pit at the superonasal edge of the optic disc (arrow) and one small pit at the superior edge of the optic disc (arrowhead). (c) B-scan image of OCT across the scanned line in Fig.6.4a shows an oval-shaped, deeply excavated pit (arrow) at the superonasal part of the optic disc with a wide opening. The depth of the pit from its opening was 1,071 μm. The nerve fibers overlying the pit are discontinuous and the lamina is torn off from the peripapillary sclera at the site of the pit (Reproduced from reference number [9] with permission)
Fig. 6.5
Conus pits present on the temporal side of the scleral ridge in an eye with type IX staphyloma (Curtin’s classification). Bar, 1 mm. (a) Photograph of right fundus of 64-year-old woman shows an oval disc with a large annular conus. A scleral ridge is shown by arrowheads. The green lines show the area scanned by swept-source optical coherence tomography (swept-source OCT) for the images shown in Figures d and e. (b) En face image of the optic disc area reconstructed from three-dimensional swept-source OCT images shows multiple pits on the slope inside the ridge at approximately same distance from the optic disc margin (arrowheads). (c) Magnified view of Figure b shows a collection of pits just temporal to the scleral ridge. (d) B-scan swept-source OCT image shows that the pit is present on the inner slope of the ridge (arrow). The peripapillary sclera and overlying nerve fiber tissue is discontinuous at the pit site. (e) Another pit can be seen inferotemporal to the optic disc (Reproduced with permission from reference number [9])
6.2.3 ICC (Intrachoroidal Cavitation)
Peripapillary ICC is observed as yellowish-orange lesion inferior to the optic disc along the inferior margin of the myopic conus funduscopically (Fig. 6.6). By using OCT, Freund et al. reported that this lesion was a localized detachment of the retinal pigment epithelium, however, the observation using more recent OCT showed that this lesion was located within the choroid and called as ‘ICC’. Shimada et al. reported that ICC was found in 4.9 % of highly myopic eyes, and interestingly, 70 % of the patients with ICC had glaucomatous visual field defects. By using EDI-OCT and swept-source OCT, Spaide et al. showed that ICC developed following the disrupted integrity of border tissue of Jacoby around the optic nerve, and the scleral curvature was bowed posteriorly at the area of ICC. Spaide also reported that the inner retina was herniated into the ICC space and in some cases, the defect of full-thickness of neural retina was observed along the border of ICC. Subsequent to the full thickness retinal defect, it is expected that the visual field defects develop in the area of the entire course of retinal nerve fiber layer which traverse the site of retinal defect. Spade also showed that the tissue separation was seen in the suprachoroid at least in some cases. The development of ICC (or suprachoroidal separation?) and subsequent defect of herniated inner retina is considered an important cause of visual field defects in eyes with pathologic myopia.