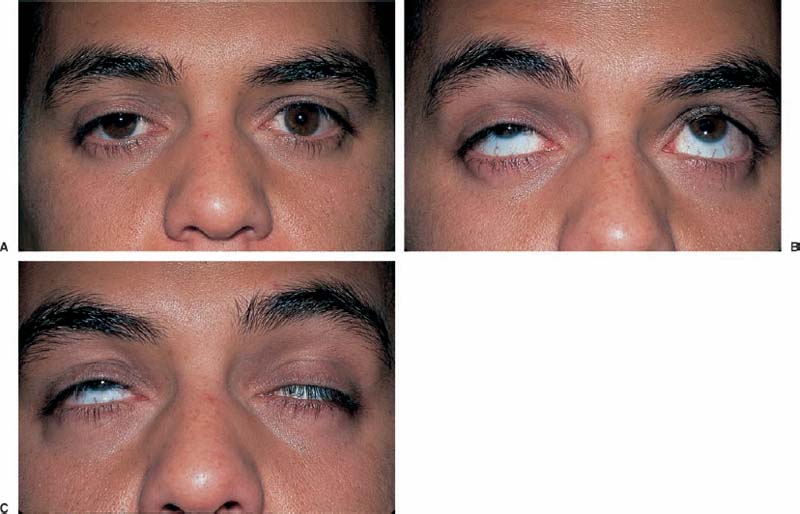
Chapter 34 These disorders may produce various degrees of ophthalmoplegia, with or without ptosis, secondary to involvement of either the neuromuscular junction or the extraocular muscles. Myasthenia gravis is not rare, and yet it frequently may be misdiagnosed early in its clinical presentation. Ocular involvement eventually occurs in 90% of all myasthenic patients, and accounts for the initial complaint in 75%.1 Initial evaluation should be directed at differentiating myasthenia gravis from mimicking ocular myopathies through confirmatory diagnostic testing, followed by systemic evaluation for comorbid conditions, such as thymoma or other autoimmune diseases. The patient with suspected myasthenia gravis should be evaluated within days to weeks, unless systemic symptoms such as shortness of breath or impaired swallowing are present, in which case immediate evaluation is required. Myasthenia may begin at any age in either sex, but there is a predilection for women in the second and third decades, and a peak for men in the sixth and seventh decades.2 Patients frequently complain of the new onset of vertical and/or horizontal diplopia, or sometimes visual blurring with rapid glances to the side. The onset of diplopia may be insidious or abrupt, and initially it is frequently intermittently present with irregular intervals of occurrence. It may be brought on by prolonged eye use, suggesting fatigability, and often rest temporarily restores normal function. Drooping of the eyelids is often asymmetric, and initially may appear unilateral, with worsening as the day progresses (diurnal fatigability). It may first be noticed by the patient, a close family member, or possibly a coworker. Patients may be aware that napping temporarily improves the ptosis. Approximately 85% of myasthenic patients with initially only ocular symptoms develop systemic disease within 2 years of diagnosis.3 Symptoms suggesting generalized myasthenia gravis include slurred speech, impaired swallowing, neck pain and weakness, breathing difficulties, and weakness of grip or proximal leg muscles. The primary ocular signs of myasthenia gravis are variable degrees of ophthalmoplegia with or without ptosis. The ptosis often worsens with prolonged upgaze (Fig. 34–1), and the combination of ptosis and weakness of the orbicularis oculi muscles (tested by having the patient squeeze eyelids closed while the examiner attempts to open them) is highly suggestive of myasthenia gravis.4 The extraocular muscle involvement may be unilateral or bilateral, and can mimic third, fourth, or sixth cranial nerve palsies; internuclear ophthalmoplegia; gaze paresis; or even comitant strabismus.5 Occasionally, in ~5% of patients, there may be coexisting signs of dysthyroid ophthalmopathy. A comprehensive list of the ocular signs of myasthenia gravis can be found in Table 34–1. FIGURE 34–1 Demonstration of fatigable ptosis with prolonged upgaze. Photographs initially show mild ptosis OS (A) that worsens when the patient is asked to sustain his gaze upwards (B), ultimately followed by marked ptosis of both lids (C).
MYASTHENIA GRAVIS AND OCULAR MYOPATHIES
URGENCY OF EVALUATION
DIAGNOSIS
SYMPTOMS
Demographics
Diplopia
Ptosis
Systemic Symptoms
SIGNS
RED FLAGS
 Pupillary responses should be normal in myasthenia gravis. Abnormal pupils should prompt further investigation to rule out other entities such as a third nerve palsy, Horner’s syndrome, botulism, or toxin-induced myopathy.
Pupillary responses should be normal in myasthenia gravis. Abnormal pupils should prompt further investigation to rule out other entities such as a third nerve palsy, Horner’s syndrome, botulism, or toxin-induced myopathy.
Ptosis exacerbated after sustained upgaze Peekaboo sign: prolonged eyelid closure leading to eye opening Lid twitch (after briefly looking down and then back to primary gaze) Orbicularis oculi weakness (tested by the examiner attempting to open the eyelids while the patient squeezes them tightly closed) Diplopia due to single or multiple extraocular muscle weaknesses Saccades: hypometria of large saccades and hypermetria of small saccades, saccadic jitter or quiver Gaze-evoked drift or nystagmus Post-edrophonium: saccadic hypermetria |
 Atypical comorbid symptoms or signs such as persistent headache, nausea or vomiting, visual loss, or unilateral body signs indicate the need for brain neuroimaging to rule out a compressive structural lesion or intracranial hemorrhage (Fig. 34–2).
Atypical comorbid symptoms or signs such as persistent headache, nausea or vomiting, visual loss, or unilateral body signs indicate the need for brain neuroimaging to rule out a compressive structural lesion or intracranial hemorrhage (Fig. 34–2).
 Eye pain is not a presenting symptom of ocular myasthenia gravis and suggests consideration of orbital imaging with either computed tomography or magnetic resonance imaging to rule out an orbital tumor or pseudotumor syndrome.
Eye pain is not a presenting symptom of ocular myasthenia gravis and suggests consideration of orbital imaging with either computed tomography or magnetic resonance imaging to rule out an orbital tumor or pseudotumor syndrome.
DIFFERENTIAL DIAGNOSIS
Chronic Progressive External Ophthalmoplegia (CPEO)
These patients present with insidiously progressive, symmetric ophthalmoplegia with varying degrees of ptosis that lacks diurnal variation (Fig. 34–3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


