11
Music and the Acoustic Desensitization Protocol for Tinnitus
The Acoustic Desensitization Protocol1 is a new approach to rehabilitating patients who suffer from tinnitus. It utilizes music that has been spectrally modified according to each individual patient’s hearing characteristics to allow intermittent interaction with, or masking of, the patient’s tinnitus, stimulate auditory pathways across a full frequency range, and facilitate relaxation, all at a comfortable listening level. This customized acoustic therapy is provided together with in-depth counseling and education on the neurological aspects of the auditory system and the emotional responses associated with tinnitus.
The protocol proceeds in two stages. In the first stage, the acoustic stimulus facilitates a high level of interaction with the tinnitus, providing the patient with early benefits in the form of enhanced relaxation and relief from, and control over, tinnitus during periods of use. In the second stage, the protocol is adjusted so as to intermittently interact with (i.e., alternately mask vs expose) the tinnitus, and the level of tinnitus exposure is gradually increased over several months. Intermittent exposure to the patient’s own tinnitus signal within the relaxed setting created by the relaxation music (reinforced by the feeling of relief and control provided by the first phase of treatment) desensitizes the patient, leading to substantial reductions in awareness of, and disturbance by, tinnitus after 4 to 6 months of therapy. Concurrent intensive counseling helps to facilitate this process. A unique portable device has been developed that enables the treating clinician to incorporate the technique into clinical practice. This chapter gives an overview of the treatment’s underlying principles and rationale, as well as the recommended protocol.
1 Acoustic Desensitization Protocol is a trademark of Neuromonics Pty. Ltd.
Underlying Principles of the Acoustic Desensitization Protocol
An Acoustic Approach to Systematic Desensitization
Problematic tinnitus obviously affects both the entire auditory system and the emotional centers of the brain, often resulting in a “vicious cycle” involving the perception of tinnitus and one’s reaction to it (Coles, 1995; Hazell, 1995). Systematic desensitization is a psychological technique traditionally used for the behavioral treatment of phobias. The method usually involves the provision of muscle relaxation training, paired with a progressively graded exposure to the phobic item (Yulis et al, 1975). Desensitization to the phobic stimulus is achieved by gradually increasing exposure levels in the context of a deeply relaxed state, with the support of the therapist.
Tyler (1996) outlined the current range of tinnitus practices that have been referred to as desensitization. He was among the first to note that complete use of systematic desensitization procedures has yet to be incorporated into tinnitus rehabilitation practices. Tyler proposed that graded exposure to noxious external sound stimuli could be used under conditions of deep relaxation to treat tinnitus. This has not been widely applied in clinical practice so far, perhaps because noxious sounds may be too aversive for tinnitus sufferers. A basic tenet of the Acoustic Desensitization Protocol is that the perception of the tinnitus itself becomes the noxious stimulus progressively introduced during a relaxed state against a background of more palatable sounds. Patients are thereby exposed to their own tinnitus in a pleasant (instead of intrusive) context. To successfully apply the Acoustic Desensitization Protocol, both clinicians and patients need to be fully conversant with this critical notion.
The Use of Music in the Acoustic Desensitization Protocol
Music has been successfully applied in several therapeutic applications (Standley, 1995). The powerful affective response to music may be related to its nonverbal nature, which allows it to directly interact with the limbic system, bypassing slower linguistically based processing in the auditory cortex (Critchley and Henson, 1977). Its use to facilitate systematic desensitization to tinnitus by employing the dynamic nature of the music to intermittently mask the perception of tinnitus is a novel application. In this approach, music further provides a relaxation stimulus that tempers the limbic/autonomic reaction as well as an auditory stimulus that activates auditory pathways across a wide frequency range. By enhancing relaxation when the tinnitus would otherwise prevent it, music helps patients to change their attitude to tinnitus.
Stimulation across a Broad Frequency Range via Customized Spectral Modification
The Acoustic Desensitization Protocol provides an audible acoustic stimulus across as wide a frequency range as possible, including over 12 kHz. The intention is to stimulate all auditory pathways so as maximize neuroplastic change.
Most tinnitus sufferers have hearing loss in the high frequency ranges (Davis, 1998), above the normal speech range frequencies that are typically measured. Consequently, the broadband signals used in tinnitus therapy are unlikely to provide optimal stimulation for these patients (Baguley et al, 1997).
In the Acoustic Desensitization Protocol, spectral modification of music signals also adjusts for the typically low-frequency emphasis in music’s spectral composition. Fig. 11–1 illustrates the spectral properties of a music recording averaged over 64 seconds, compared with the mean hearing threshold levels of a cohort of 80 tinnitus patients (Davis et al, 1999), matched at 4 kHz. The music waveform illustrates that the greatest energy is centered between 200 Hz and 2 kHz, with little energy (on average) above 3 kHz. Among the typical sample of tinnitus patients, hearing thresholds decline substantially above 3 kHz. With such patients, in the absence of spectral modification, the lower frequency components of the music would need to be quite loud before the higher frequency components could be adequately perceived. Even patients with normal hearing across the entire frequency range benefit from spectral modification as a result of the low-frequency bias of most music.
Use of earphones ensures provision of a calibrated “dose” without attenuation of the very high frequency signals over distance through the free field.
For the Acoustic Desensitization Protocol, the acoustic signal is spectrally modified in a tailored and patented manner according to each patient’s audiogram using customization algorithms developed by the author and fine-tuned over several clinical trials (Davis 1998; Davis et al, 2002b). Signal customization, together with the use of high-fidelity earphones, ensures that, at a comfortable listening volume, even stimulation is provided across a wide frequency range despite any hearing loss.
Tinnitus patients often experience loudness discomfort levels that are lower than what would be expected for their particular level of sensorineural hearing loss (Coles and Sood, 1988; Stouffer and Tyler, 1990; Tyler and Conrad-Armes, 1983). The aforementioned algorithms are calibrated to account for these abnormally steep loudness growth characteristics, particularly in those with minimal to moderate hearing loss.
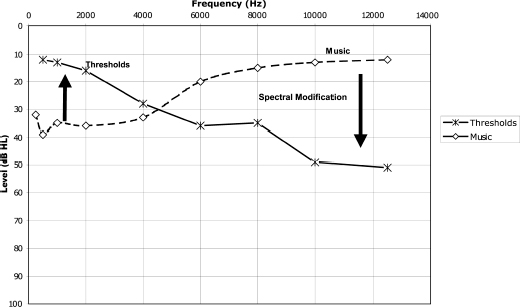
Figure 11–1 Spectral characteristics of typical unmodified music versus hearing thresholds of tinnitus patients.
Adjustment for Asymmetrical Hearing Loss and Importance of the Stereo Effect
With the intention of stimulating the integrative pathways of the auditory system, the spectral modification is undertaken in a manner that accounts for any asymmetry in hearing thresholds across the two ears and provides the acoustic stimulus in full stereo. This contrasts with the uncorrelated signals provided by bilateral tinnitus maskers or hearing aids. This stereo effect may explain why this approach has been found to provide an effective masking stimulus to those patients who report “central tinnitus” and who were unable to achieve masking with other devices (Davis, 1998).
Staged Treatment Delivery
Consistent with the graded increase in exposure that is provided in a systematic desensitization protocol, the treatment is delivered in two stages:
1. Spectrally modified music (with noise) is initially used to achieve a high level of interaction with the tinnitus.
2. Spectrally modified music (without noise) allows intermittence of the inter action (masking vs exposure); the degree of exposure is gradually increased by decreasing the volume over several months.
In the first stage, music has noise added to facilitate a high level of interaction at a comfortable listening level. The sound of this noise is often described by patients as a light “shower sound.” The source recording of this noise band is embedded in the music at a predetermined signal-to-noise ratio, and this mix is then individually customized. The ability to achieve a high level of tinnitus interaction provides patients with a sense of relief and control over the tinnitus, and promotes a reduction in general anxiety levels.
In the second stage, the tinnitus is masked during peaks in the music; during the troughs, the tinnitus is momentarily exposed. Reducing the volume of the music over time gradually increases these exposure times. Through repeated, momentary exposure, in the context of a relaxation stimulus, the patient gradually becomes desensitized to the tinnitus signal. Over time, this results in reduced awareness of, and disturbance by, the tinnitus.
Counseling
The principles underlying the counseling approach used in the Acoustic Desensitization Protocol are outlined later in this chapter.
Implementation of the Acoustic Desensitization Protocol
Overall Treatment Flow
Fig. 11–2 depicts the typical treatment flow.
The process begins with diagnostic tests to determine hearing thresholds, minimum masking levels, tinnitus pitch match, residual inhibition, and loudness discomfort levels. In addition, patients are educated as to the likely pathogenesis of their tinnitus. A purpose-built device2 is then prescribed with embedded acoustic therapy customized for the patient and provided with instructions for use so as to provide a high level of interaction. The patient’s response is checked around 2 weeks later, and any difficulties that the patient may be encountering in using the device are discussed and resolved. After a further 6 weeks (subject to patient readiness), the stage 2 acoustic signal is provided, and patients are instructed in its use to provide intermittent interaction with their tinnitus.
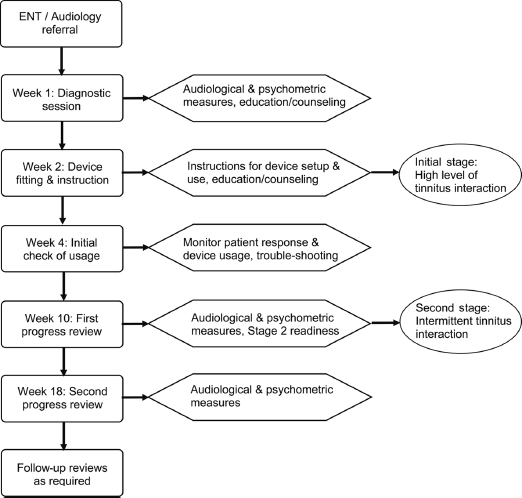
Figure 11–2 Acoustic Desensitization Protocol treatment flow. ENT, ear, nose, and throat specialist.
Progress review appointments should include the measurement of audiological and psychometric parameters to monitor progress and provide positive feedback to the patient. The clinician may sometimes find the need to supplement the minimum number of visits, particularly during the early weeks of therapy, to ensure appropriate compliance to the protocol.
2 Neuromonics Pty. Ltd. (www.neuromonics.com) provides a purpose-built processor for use with the Acoustic Desensitization Protocol.
Patient Candidacy and Selection
The Acoustic Desensitization Protocol is suitable for patients with a wide range of hearing characteristics. Those occasional patients with hearing within the normal range at all frequencies bilaterally still tend to benefit from this approach because spectral modification overcomes the low-frequency emphasis of music. Those with a severe or profound bilateral hearing loss are not clear candidates because they might benefit more from hearing aids or cochlear implants. Patients with a severe or profound unilateral hearing loss can be helped using contralateral stimulation, although the presentation level tends to be somewhat higher than binaural cases. Their candidacy should be verified by contralaterally performing the minimum masking level tests to determine up front if a masking-type interaction is possible at a comfortable listening level.
Those patients with clinically significant depression may find it difficult to adhere to the treatment regime without additional psychological or psychiatric intervention and support. With such patients, tinnitus-specific counseling may continue concurrently, and the use of this acoustic therapy (with a high level of interaction) can be promoted as a crisis management tool that helps them sleep and feel more in control of their tinnitus.
Some professionally trained musicians do not respond as well to music-mediated therapy, perhaps as a result of an intellectual response to the music, which interferes with their relaxation response. With such patients, the treating clinician needs to emphasize the need to strive to place the music into the background of their consciousness. As an alternative to music, spectrally modified environmental noise recordings, particularly those incorporating beachside wave sounds, may be considered.
Tests and Measures
A pure-tone audiogram, including thresholds at 10 and 12 kHz, needs to be recorded for all patients. For counseling reasons, the author routinely measures tinnitus pitch match, loudness balance, residual inhibition, minimum masking levels, and loudness discomfort levels. The latter two measures are also repeated as objective mid- and post-therapy indices, along with psychometric indices such as the Tinnitus Reaction Questionnaire. Loudness discomfort level measurement has been adapted to avoid any exacerbation of tinnitus through exposure to loud noise; the adapted approach defines “uncomfortably loud” as the level that would be uncomfortably loud if it had to be listened to for more than a minute (but it is presented for only a few seconds).
Device Setup
The acoustic signal in the Acoustic Desensitization Protocol is administered via a portable device that has been designed to promote optimal treatment. Prior to fitting of the device, the customization and programming of the device are conducted by the manufacturer. This device is displayed in Fig. 11–3.
Use of Earphones
The use of high-fidelity earphones is essential for the Acoustic Desensitization Protocol to be effective. The “open-air” types of earphones are more suitable than the “sound-insulating” types, which tend to increase perception of the tinnitus and cause straining to hear important outside sounds. To enable the patient to easily identify the correct transducer for each ear while in the dark, the earpieces need to be a different shape for each side. Importantly, patients need to be warned against changing earphones during treatment. This is because different models of earphones display differing frequency response characteristics, and the spectral modification algorithms are calibrated for the specific model of earphones recommended for the patient.

Figure 11–3 The Acoustic Desensitization Protocol device (courtesy Neuromonics Pty. Ltd.).
General Guidelines for Use of the Device
A critical aspect is to provide clear instructions to patients about the use of the device and the rationale for the protocol. This motivates them to use the device sufficiently often and without impediments, and sets realistic outcome expectations.
The patient is advised to use the device when the tinnitus is most disturbing, which is typically in the quieter times like sleep onset, premature waking, reading, contemplating, or relaxing. After they have been heard several times, the customized stimuli can be used while reading or writing. The presentation level is usually low enough that patients can still hold a conversation with the stimulus playing, so the earphones do not need to be removed for short communication exchanges.
Recommended use is at least 2 hours daily. However, for the first 2 to 4 months, usage of 3 hours per day is better, and patients should be encouraged to try for somewhat longer if possible. The device is lightweight and compact (similar in size to many mobile phones), allowing it to be carried around for use during daily activities.
As the tinnitus becomes progressively less disturbing, the device can be used correspondingly less, until the patient feels it is no longer necessary. It is likely that patients will want to keep the device “just in case.” Sometimes the tinnitus disturbance can reappear due to conductive pathology, periods of significant stress, or noise exposure, so additional stimulation may be desired to further treat the tinnitus under such circumstances.
Clinicians should check usage carefully at review appointments because one of the most common causes of substandard progress is insufficient use of the device. Impediments to obtaining sufficient stimulation may need to be determined, and creative strategies for circumventing them devised.
VOLUME SETTING DURING STAGE 1 THERAPY
The specific volume-setting instructions depend on the stage of therapy. During stage 1, a high level of interaction is prescribed. The volume control should be set at the beginning of the session so that the combined music/noise signal just “covers up” the tinnitus, provided that at all times the volume is set at a comfortable level.
Most people find that the more they listen, the less likely they are to be consciously aware of the music. Constant monitoring of either the volume level or the tinnitus can be counterproductive to the ultimate goal of reducing distress and awareness. To help prevent this, patients should be instructed to engage in another quiet activity while the music is playing in the background, such as reading, computer work, walking, gardening, and quiet household activities.
After around 2 months of use, patients typically report feeling that they are now in control of their tinnitus, or at least in control of those aspects that were interfering with their lifestyle, thus signaling successful completion of phase 1.
TRANSITION TO STAGE 2 THERAPY
To facilitate the desensitization process, some exposure to the tinnitus signal is required, so in phase 2, the protocol is adjusted to provide intermittent interaction with the tinnitus. At the beginning of each listening session during this phase of treatment, the volume should be set so that the tinnitus is covered up during the medium to louder passages, and is momentarily apparent during the softer passages, as depicted in Fig. 11–4.
Clinicians should instruct patients to always set the volume at the beginning of each therapy session to ensure that their tinnitus is covered up only around half of the time. It is critical that patients understand that after the first minute or so, they should not monitor the level of interaction or reset the volume until the beginning of the next therapy session. Patients typically find they have been progressively lowering the volume from month to month, and this tends to be reflected in repeat audiometric measures of minimum masking levels using broadband noise. Toward the end of stage 2, the music volume setting can be quite low.
Counseling
Following is a brief outline of the elements underlying the counseling approach that has been used as part of the Acoustic Desensitization Protocol. Some of the elements have been inspired by existing counseling models, such as systematic desensitization of phobias, cognitive therapy, psychosocial counseling, common rehabilitation strategies from cochlear implantation/hearing aids, and sound therapies for tinnitus, including tinnitus total masking and tinnitus partial masking therapy (e.g., Hazell, 1995; Tyler and Babin, 1986; Vernon and Schleuning, 1978) and tinnitus retraining therapy (Jastreboff et al, 1994), as well as music therapies. Other aspects have been derived from clinical experience with the protocol.
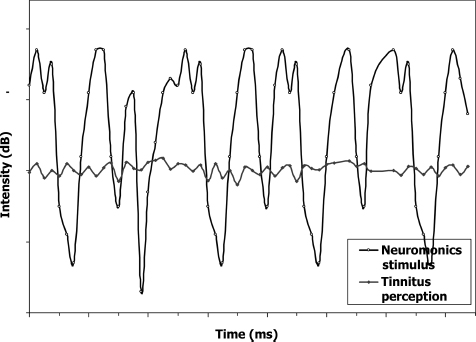
Figure 11–4 Schematic representation of intermittent interaction instructions.
CORE COUNSELING STYLE
Counseling is considered to be an interactive dialogue with the patient that needs to acknowledge the person’s particular circumstances and immediate responses to material being presented. Counseling needs to be tailored to the individual, taking into account his or her particular educational level, personal style, cognitive functioning, level of preconditioning, and so on. The overall intention is to provide a nurturing environment in which patients can describe their experience of tinnitus and their emotional reaction to it. The clinician needs to provide an unconditional positive regard, actively listening, and making skillful use of questioning to elicit more information when it appears relevant.
The collaborative dialogue can begin with questioning on several topics, such as how the patient feels about the tinnitus and how he or she got it, how the patient has been diagnosed and treated so far, the patient’s expectations for the future, and so on. Many patients report that they feel relieved in being able to share their experience with someone else who is sympathetic, and they can take great comfort in hearing that they have not been alone in having these experiences and feelings. This process can be therapeutic in that the patient needs to reconsider his or her experience from the perspective of someone new, ordering the component parts of that experience in a new way that gives the “big picture” for both clinician and patient. It also is a useful period in which rapport can be developed before cognitive restructuring begins, and written notes should be made with regard to any apparent unproductive cognitive distortions that may need addressing later on.
DIAGNOSIS
The case history helps to determine the likely cause(s) of tinnitus and the major exacerbating factors, and also helps to orient the patient to the more important aspects of his or her history and current lifestyle that are influencing the tinnitus experience. The patient is asked to complete the comprehensive case history questionnaire by mail a week or so prior to the initial appointment. This gives sufficient time to check medications and talk with the patient’s family and medical practitioners about such items as noise history and previous diagnoses. These written responses are then reviewed by the clinician in the presence of the patient, clarifying and elaborating each answer.
The audiometric measurement of the tinnitus also gives the patient an opportunity to describe his or her tinnitus in a supportive and understanding atmosphere. By sharing this with others, it helps acknowledge that the patient’s experience is phenomenologically real. The clinician’s explanation of the tinnitus and hearing loss measurements sets the scene for a dialogue aimed at understanding the specific effects of the patient’s condition, such as the ramifications of having a hearing loss only for the higher frequencies. The patient’s minimum masking levels, loudness discomfort levels, and loudness balance results are also a useful starting point for the description of the central auditory amplification hypothesis. Without a reliable reference to benchmark their tinnitus to, many sufferers find it difficult to gauge their progress in response to therapy. For this reason, a repeat administration of the psychometric and audiometric indices at progress reviews can be very heartening.
EDUCATION
The clinician needs to explain all the pertinent aspects of the patient’s particular case history in terms of a model of tinnitus pathogenesis that is credible to the patient. The process should thus provide a detailed explanation of normal auditory system functioning and emphasize the role of the cochlear nerves, brainstem, auditory cortex, and limbic system. The inherent plasticity of the auditory pathways needs to be emphasized because this is the basis of the reasoning given for how neurological changes might ultimately be effected.
The details of the patient’s specific dysfunction should then be explained in similar terms, and this description should be constantly referred back to the particular case history features. For example, if the participant has an extensive history of noise exposure and a corresponding hearing loss configuration, then it needs to be explained why he or she may only have become aware of it after a bout of influenza (the neurological noise floor being uncovered by additional hearing loss, then increased adaptive efferent activity, etc.). A box diagram (e.g., Jastreboff et al, 1996) can be a convenient way to “compartmentalize” the various aspects of tinnitus pathogenesis and their interrelationships.
IDENTIFICATION AND CHALLENGING OF COGNITIVE DISTORTIONS
Direct questioning should be used to identify the presence of cognitive distortions, such as “My tinnitus will get worse” or “go on for ever,” “Tinnitus is a physical disease,” “There is no treatment,” “I will be deprived of sleep because of my tinnitus,” “Tinnitus will make me go deaf,” “Tinnitus will make me go mad,” and “Tinnitus is caused by a tumor.” Alternative perspectives can then be offered and a rationale given, but care should be taken to remain collaborative rather than directive.
DEVICE-SPECIFIC INSTRUCTION
A careful description of the aforementioned principles of systematic desensitization is required, as this is the basis of the progressive changes in volume control setting. The device usage instructions need to be first covered verbally, then provided to the patient for at-home reference.
GOAL SETTING AND EXPECTATION MANAGEMENT
The incremental nature of likely benefits needs to be clearly understood, and the fact that this is not a “magic overnight cure” may require constant reiteration. Patients should be counseled to expect distinct benefits over the duration of treatment. Early on, they can expect an enhanced ability to relax and sleep, plus a sense of relief, as they can now use the device at those times when otherwise they would be disturbed by their tinnitus. This is followed by the development of a sense of control over the tinnitus, with a corresponding reduction in the fear of the tinnitus because the lifestyle impediments previously faced are reduced. Then, over a period of several months, they can expect to experience gradual desensitization, whereby there is a gradual reduction in the percentage of the time that they are generally aware of the tinnitus until over time it ceases to be disturbing. The expectation should be that this will be an incremental process over some months, mediated by the degree of effort that they contribute to the process.
Patients can benefit from collaboratively devising a written plan of specific goals and actions. These provide a useful way to set realistic expectations and tangible milestones and can be referred to at periods of crisis or indecision, or otherwise as inspiration (Davis, 1999).
NURTURING EXPECTATIONS
The deliberate nurturing of patient expectations has the potential to greatly improve the treatment process (Tyler et al, 2001). Accordingly, with the Acoustic Desensitization Protocol, the patient’s expectation of a positive prognosis is nurtured with reference to the results of previous clinical trials of the approach, which reveal a high rate of success. This is typically reinforced by the patient’s experience of benefits early on in treatment. Patients benefit greatly from an explanation of the typical physiological response to relaxation music, with respiration rate slowing and heartbeat slowing to match the meter of the music; by recognizing these effects, the efficiency of their relaxation response can be increased, consistent with biofeedback techniques.
GENERAL TINNITUS MANAGEMENT STRATEGIES
In addition to the use of the customized acoustic therapy, which, among other things, promotes relaxation, more general sleep hygiene practices should be recommended, including avoiding naps, increasing exercise levels, preventing clock watching, adopting a lunchtime “worry time,” and reducing excess caffeine consumption (Davis and Wilde, 1995). Other generally accepted tinnitus management strategies, such as management of general stress levels, should also be outlined.
Consistent with tinnitus retraining therapy (Jastreboff et al, 1996), the avoidance of total silence is strongly promoted, with the customized device advocated as the most frequently used tool to enable this. The Acoustic Desensitization Protocol diverges from tinnitus retraining therapy in that it promotes the use of the device (with a high level of interaction) as a coping aid initially, although only on an interim basis. The rationale for this is that using tools to reduce the lifestyle-disturbing manifestations can reduce fear of the tinnitus and thereby facilitate progress with treatment. Furthermore, the ability of music to engage the limbic system in a positive way appears to facilitate relaxation and attitudinal change in a more effective manner than the use of emotionally neutral noise.
IMPORTANCE OF WRITTEN MATERIAL
Tinnitus patients cannot be expected to recall all that is covered in counseling. The concurrent presence of hearing loss makes reliance on verbal counseling particularly challenging. As a result, provision of written summaries of the main points of therapy is advised.
THERAPY TROUBLESHOOTING
If patients do not appear to be progressing reasonably in terms of measurable changes in repeated psychometric and audiometric measures, several questions can be asked to determine if there are specific factors limiting treatment effectiveness, as follows:
1. Is the device being used for long enough each day?
2. Is the patient using it at those times of the day when the tinnitus is most disturbing, which would typically be in the quieter times?
3. Is the patient setting the volume in a manner that is consistent with the protocol?
4. Is the patient “listening in” to the music too much (i.e., not placing music in the background of consciousness)?
5. Has the patient recently had a cold, flu, allergy, or eustachian tube dysfunction?
6. Has the patient begun any new medication or changed the dose of existing medication?
7. Has the patient had excessive noise exposure lately?
8. Has the patient had extended periods of straining to hear clearly?
9. Has the patient had a period of acute stress?
10. Is there anything else that the patient thinks may have inhibited his or her progress?
11. Has an improvement occurred so gradually as to not be immediately apparent?
12. Are the patient’s expectations for a speedy improvement reasonable?
Expected Outcomes: A Case Study
The effectiveness of the Acoustic Desensitization Protocol has been demonstrated in several clinical trials (e.g., Davis et al, 2002a). A typical case study from a recent trial is described below.
Mr. X was a 62-year-old teacher who presented with a left-sided hissing tinnitus, which had a sudden onset a year prior to his referral to the university tinnitus clinic. It was significantly interfering with his reading, lesson planning, and sleep onset/maintenance. There were also pronounced bilateral sound tolerance problems, with even some telephone conversations being uncomfortably loud.
A mild to moderate mid- to very high frequency sensorineural hearing loss was found, and was 15 dB worse on the left for the midfrequencies (Fig. 11–5). The tinnitus was matched to a narrowband noise centered around 6 kHz, an octave below the maximal hearing loss frequency. The broadband noise minimum masking level was quite high at 20 dB SL, and loudness discomfort levels were found to be markedly low (normally ∼95 dB). These measures suggested a high-magnitude tinnitus and hyperacusis.
During treatment, as is the case with many patients, Mr. X had to be reminded at progress reviews to reset his volume settings at the commencement of each listening session to ensure the appropriate level of interaction was attained. He also then needed reminding not to constantly monitor the volume level once it was initially set at the beginning of each therapy session.
After 2 months of stage 1 therapy, working, sleeping, and tolerance of external sounds had markedly improved, and these were reflected in the audiometric and psychometric data obtained, as summarized in Fig. 11–5 and Table 11–1. After 2 months of stage 2 treatment, further improvements were reported. Mr. X reported that he was now only rarely aware of his tinnitus while the device was not in use, and not at all while using it. He was not often very conscious of the music while it was playing, but it still seemed to evoke a strong relaxation response.
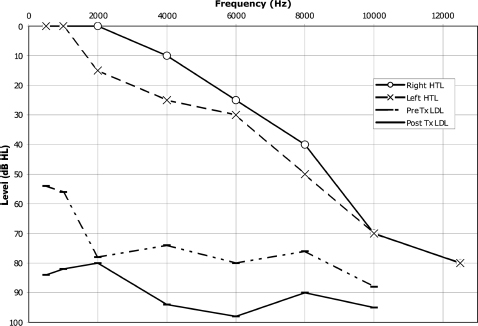
Figure 11–5 Case study: audiogram and loudness discomfort levels. HTL, hearing threshold level (dBHL); pre TX, pre-therapy; Post Tx, post-therapy; LDL, loudness discomfort level (dBHL).
| Prior to Treatment | After 2 Months of Treatment | After 4 Months of Treatment | |
|---|---|---|---|
| Minimum masking level (dB SL) | 20 | 10 | 2 |
| TRQ | 30 | 8 | 0 |
| VAS3-tinnitus severity | 5 | 4 | 1 |
| VAS-relaxation levels | 5 | 4 | 1 |
| VAS-decreased sound tolerance | 5 | 4 | 1 |
| Awareness of tinnitus (% of time) | 100 | 40 | 10 |
dB SL, decibel sensation level (i.e., loudness relative to hearing threshold); TRQ, tinnitus reaction questionnaire composite score (Wilson et al, 1991); VAS3, Visual Analogue Scale.
Conclusion
The Acoustic Desensitization Protocol constitutes a new technique that incorporates principles of systematic desensitization, habituation therapy, music therapy, and clinical psychology. Pivotal to its application is the use of an individually customized, spectrally modified acoustic stimulus that provides an intermittent interaction with the tinnitus while simultaneously facilitating a relaxation response. Comprehensive counseling is also an essential aspect. If applied according to the protocol described herein, clinicians can expect to produce large improvements in most clinical measures over a period of several months with a relatively modest amount of contact time.
3 VAS, Visual Analogue Scale, a 10-point scale, pretreatment anchored at 5, with deterioration being reflected in scores toward 10, improvement in scores toward 0. It was adapted from Coles (1991) to encompass the separate domains of tinnitus severity, general relaxation levels, and decreased sound tolerance.
References
Baguley DM, Beynon GJ, Thornton F. A consideration of the effect of ear canal resonance and hearing loss upon white noise generators for tinnitus retraining therapy. J Laryngol Otol 1997;111:810–813
Coles RRA, Sood SK. Hyperacusis and phonophobia in tinnitus patients. Br J Audiol 1988;22:228
Coles RRA. Some aspects of evaluation of treatment effects. In: Aran J-M, Dauman R, eds. Proceedings of the Fourth International Tinnitus Seminar. Amsterdam and New York: Kugler Publications; 1991:563–568
Coles RRA. Models of tinnitus: generation, perception, clinical implications. In: Vernon J, Møller A, eds. Mechanisms of Tinnitus. Boston: Allyn & Bacon; 1995:57–72
Critchley M, Henson RA, ed. Music and the Brain: Studies in the Neurology of Music. Springfield, IL: CC Thomas; 1977
Davis PB. Music as therapy in the rehabilitation of tinnitus sufferers: effects of spectral modification and counseling [Ph.D. dissertation]. Perth, Australia: School of Speech and Hearing Science, Curtin University of Technology; 1998
Davis PB. A neurophysiologically-based weekend workshop for tinnitus sufferers. In: Hazell J, ed. Proceedings of the Sixth International Tinnitus Seminar. London: Tinnitus and Hyperacusis Centre; 1999:365–467
Davis PB, Wilde RA. Clinical trial of a new tinnitus masking technique. In: Reich GE, Vernon JA, eds. Proceedings of the Fifth International Tinnitus Seminar. Amsterdam and New York: Kugler Publications; 1995:305–309
Davis PB, Wilde RA, Steed L. Changes in tinnitus distress over a four month no-treatment period: effects of audiological variables and litigation status. In: Hazell J, ed. Proceedings of the Sixth International Tinnitus Seminar. London: Tinnitus and Hyperacusis Centre; 1999:384–390
Davis PB, Wilde RA, Steed L. Clinical trial findings of a neurophysiologically-based tinnitus rehabilitation technique using tinnitus desensitization music. In: Patuzzi R, ed. Seventh International Tinnitus Seminar. Fremantle: University of Western Australia; 2002a:74–77
Davis PB, Wilde RA, Steed L. Neurophysiologically-based tinnitus rehabilitation using tinnitus desensitization music. In: Patuzzi R, ed. Seventh International Tinnitus Seminar. Fremantle: University of Western Australia; 2002b:188–190
Hazell JWP. Tinnitus as a manifestation of a survival style reflex. In: Reich GE, Vernon JA, eds. Proceedings of the Fifth International Tinnitus Seminar. Portland, OR: American Tinnitus Association; 1995:579–582
Jastreboff PJ, Gray WC, Gold SL. Neurophysiological approach to tinnitus patients. Am J Otol 1996;17:236–240
Jastreboff PJ, Hazell JWP, Graham RL. Neurophysiological model of tinnitus: dependence of the minimal masking level on treatment outcome. Hear Res 1994;80:216–232
Standley J. Music as a therapeutic intervention in medical/dental treatment: research and clinical applications. In: Wigram T, Saperston B, West R, eds. The Art and Science of Music Therapy: A Handbook. Chur, Switzerland: Harwood Academic Publishers; 1995:3–22
Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord 1990;55:439–453
Tyler RS. Tinnitus treatments modify behaviour. Hearing Instruments 1996;March:20–24
Tyler RS, Babin RW. Tinnitus. In: Cummings CW, Fredrickson JM, Harker L, Krause CJ, Schuller DE, eds. Otolaryngology-Head and Neck Surgery. Vol 4. St. Louis: CV Mosby; 1986:3201–3217
Tyler RS, Conrad-Armes D. The determination of tinnitus loudness considering the effects of recruitment. J Speech Hear Res 1983;26:59–72
Tyler RS, Haskell G, Preece J, Bergan C. Nurturing patient expectations to enhance the treatment of tinnitus. Semin Hear 2001;22:15–21
Vernon J, Schleuning A. Tinnitus: a new management. Laryngoscope 1978;88:413–419
Wilson PH, Henry J, Bowen M, Haralambous G. Tinnitus reaction questionnaire: psychometric properties of a measure of distress associated with tinnitus. J Speech Hear Res 1991;34:197–201
Yulis S, Brahm G, Charnes G, Jacard LM, Picota E, Rutman F. The extinction of phobic behavior as a function of attention shifts. Behav Res Ther 1975;13:173–176
< div class='tao-gold-member'>



