Chapter 31 Minimally Invasive Video-Assisted Thyroidectomy
Introduction
 Please go to expertconsult.com to view related video Minimally Invasive Video-Assisted Thyroidectomy.
Please go to expertconsult.com to view related video Minimally Invasive Video-Assisted Thyroidectomy.
The first endoscopic procedures proposed to reduce the invasiveness in the neck were endoscopic and video-assisted parathyroidectomies,1,2 because it was evident that patients with parathyroid adenomas were ideal candidates for a minimal access surgery being that these tumors were mostly benign and characterized by small size (see Chapter 61, Minimally Invasive Video-Assisted Parathyroidectomy). Later on, the same approach proved to be suitable also for removing small thyroid nodules, with some modifications.3–5 At present, some controversies still exist about what should be considered a true minimally invasive operation for thyroid. Although the concern raised by some about the possible adverse effect of CO2 insufflation in the neck was probably overstated,6 the procedure we initially developed in 1998, minimally invasive video-assisted thyroidectomy (MIVAT), was characterized by the use of external retraction avoiding any gas inflation, which is not necessary to create an adequate operative space in the neck (see Chapter 36, Robotic and Extracervical Approaches to the Thyroid and Parathyroid Glands: A Modern Classification Scheme).
Preoperative Evaluation and Anesthesia
The inclusion criteria and the main contraindications are summarized in Table 31-1. The most relevant limit is represented by the size of both the nodule and the gland as measured by means of an accurate ultrasonographic study to be performed preoperatively. In endemic goiter countries indeed the gland volume can be relevant (independently from the nodule volume), as larger gland volume may be responsible for the necessity of converting to an open procedure. Ultrasonography can also be useful to exclude the presence of a thyroiditis, which might make dissection troublesome. In case ultrasonography only gives the suspicion of thyroiditis, of course, autoantibodies should be measured in the serum. Known preoperative thyroiditis is considered a contraindication.
Table 31-1 Indications and Contraindications for MIVAT
| Indication* | Contraindication |
|---|---|
| Benign disease | Recurrent disease |
| Low-risk papillary carcinoma | Locally advanced or metastatic carcinoma |
| Graves’ | Short neck in obese patient |
* Thyroid volume less than 25 mL and nodule diameter less than 3 cm.
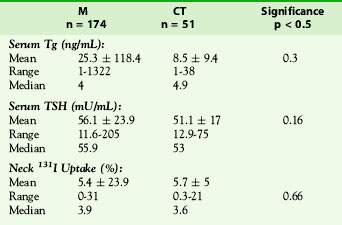
One of the most controversial aspects in terms of indications is in treatment of malignancies. When dealing with papillary carcinoma, MIVAT provides the same clearance at the thyroid bed level as conventional technique, as clearly demonstrated in two different studies performed at the Department of Surgery in Pisa. The first one is a prospective randomized study7: 35 patients with low-risk papillary carcinoma were allotted; 16 were operated on with MIVAT (group A) and 19 with conventional technique (group B). One month after surgery, thyroglobulin (Tg) serum level was measured and a whole-body scintigraphy (WBS) with 131I was performed in all patients, and no statistically significant difference in the results between the two groups was found (the Tg serum level was 5.3 +/− 5.8 ng/L and 7.6 +/− 21.7 ng/L and the mean radioiodine uptake was 3.9 +/− 4.4% and 4.6 + 6.7%, respectively, in groups A and B). The second prospective study involved 221 patients with a papillary carcinoma smaller than 30 mm, with an ultrasound-estimated thyroid volume of less than 30 mL and no ultrasound evidence of lymph node metastasis or thyroiditis.8 One hundred seventy-one patients were operated on with MIVAT (group A) and 50 with conventional technique (group B). After a mean follow-up of 3.6 ± 1.5 years (with a range of 1 to 8 years and a mean 5 years), there were no statistically significant differences between the two groups in terms of age, sex, and mean follow-up. No differences in serum Tg and TSH levels and 131I neck uptake were observed between the two groups of patients (Table 31-2), and no statistical difference in cure rate was found between papillary cancer of the thyroid (PTC) patients treated with MIVAT versus open conventional surgery at the end of the follow-up period. Rates of hypoparathyroidism or recurrent laryngeal nerve palsy were also equivalent. These results with up to 5 years of follow-up clearly suggest that MIVAT is a safe and effective technique in the treatment of low- and intermediate-risk papillary carcinomas.
Table 31-2 Postsurgical Features Related to the Degree of Surgical Completeness in PTC Patients Treated with MIVAT (M) and Conventional Thyroidectomy (CT) at the Time of 131I Remnant Ablation (no differences in serum Tg and TSH levels and 131I neck uptake were observed between the two groups of patients)
Surgical Technique
Operating Room Setup
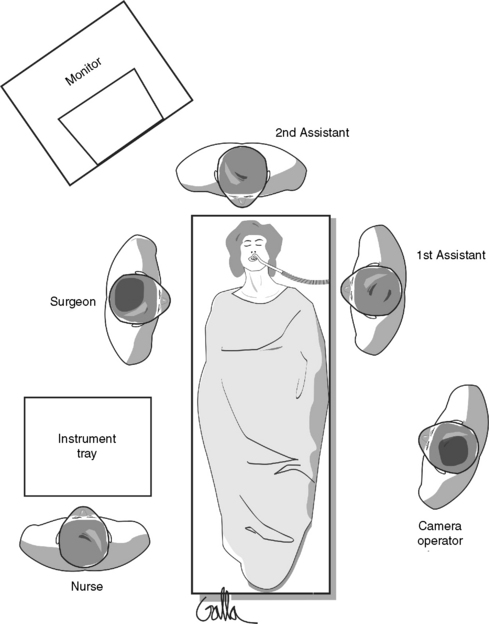
Team (Figure 31-1)
• The surgeon is on the right side of the table.
• The first assistant is on the left side of the table (opposite the surgeon).
• The second assistant is at the head of the table.
• The third assistant is on the left side of the table
• The scrub nurse is behind the surgeon on the right side of the table.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


