This article discusses the indications, surgical technique, results, and complications of middle fossa craniotomy (MFC) for vestibular schwannoma surgery, focusing on issues such as serviceable hearing, tumor characteristics, and patient-specific factors that help determine options for therapy. MFC is suitable for intracanalicular vestibular schwannomas that extend less than 1 cm into the cerebellopontine angle in patients with good hearing. With the expanding use of modern imaging, many small tumors are being identified in patients with no or minimal symptoms. Patients with these tumors have three therapy options: (1) stereotactic radiotherapy, (2) microsurgery, and (3) observation (ie, wait-and-scan approach).
| ABR | Auditory brainstem response |
| CNAP | cochlear nerve action potentials |
| CSF | Cerebral spinal fluid |
| GSPN | Greater superficial petrosal nerve |
| IAC | Internal auditory canal |
| MFC | Middle fossa craniotomy |
| PTA | Pure tone threshold average |
| VEMP | Vestibular evoked myogenic potentials |
| WRS | Word recognition score |
Middle fossa craniotomy
The middle fossa craniotomy (MFC) approach for removal of vestibular schwannomas, also known as the transtemporal-supralabyrinthine approach , was popularized by House and consists of the supralabyrinthine dissection of the internal auditory canal (IAC). House introduced revolutionary concepts, including many of the principles of skull base surgery that are now taken for granted, such as the use of the operating microscope, continuous suction irrigation, diamond stone burs, and a multidisciplinary team approach.
The MFC had been used for other indications, and Hartley has been credited with the first description of this approach for the surgical treatment of trigeminal neuralgia. Over the years this approach has been used for the treatment of other neurotologic conditions, such as debridement of inflammatory lesions of the petrous apex, facial nerve decompression and grafting, repair of meningoceles, repair of semicircular canal dehiscence, and vestibular nerve sectioning. Kawase and colleagues described an extended middle fossa approach that included dissection of the petrous apex for the exposure of aneurysms of the basilar artery, and this modification has helped expand the indications of this technique for the treatment of selected petroclival tumors.
Indications for surgery
With the current increase in the use of MRI, the identification of small (<1.5 cm) tumors in patients with normal or near-normal hearing also has been on the rise. Today’s skull base surgeons face the dilemma of selecting among three different therapy options for small and minimally symptomatic tumors: microsurgical removal, stereotactic radiation, and observation. During the initial evaluation of patients, surgeons must consider several audiometric, tumor, and patient factors to determine the risk of intracranial surgery, chances of function preservation, and long-term quality-of-life issues. MFC should be offered only for patients who have the best chance of serviceable hearing preservation, and when the risk/benefit analysis is favorable and accepted by the informed patient.
Audiometric Factors
Preservation of serviceable hearing
The goal of MFC is to achieve tumor removal and preserve auditory function that will be useful to the patient long-term. Useful, or “serviceable,” hearing can only be preserved if it is present preoperatively. The definition of serviceable hearing must be individualized, because it depends on several factors, such as audiometric values of the ipsilateral and contralateral ears, progression of hearing loss, patient preference, and available strategies of hearing loss habilitation. Preservation of binaural hearing is important for sound localization and speech understanding in noise; for a patient to benefit from binaural hearing, the interaural average four-frequency (0.5, 1.0, 2.0, and 3.0 kHz) hearing threshold should be less than 20 dB, and the interaural word discrimination score should be less than 20%. The determination of serviceable hearing in a patient with a tumor in the only hearing ear or in patients with bilateral tumors is obviously very different; some patients would choose to keep their hearing at any level even if it only provides sound awareness. The surgeon’s must ensure that the patient has appropriate expectations, habilitation options are available, and the overall quality of life is not placed at risk in exchange for the promise of some measurable auditory function.
From the audiometric standpoint, hearing is characterized by the combination of the four-frequency pure-tone threshold average (PTA) and the word recognition score test (WRS). What is considered serviceable hearing and a definition of success in hearing preservation in some centers is PTA and WRS values of at least 30 dB and 70%, respectively, and in other centers at least 50 dB and 50%, respectively. Hearing aid benefit is limited below the 50/50 level. Because some hearing may be lost immediately or gradually after surgery, and better preoperative hearing has been associated with better chances of early and long-term hearing preservation, it seems intuitive that hearing preservation surgery should be offered only to patients with hearing well above the 50/50 level. The 50/50 level of hearing represents the minimum serviceable hearing and, if preserved at or above this level, allows patients the use of amplification if needed.
Audiologic prognostic parameters beyond preoperative hearing function
Several prognostic signs for hearing preservation have been studied but, except for good preoperative hearing, most of these lack sufficient sensitivity and specificity to be reliable.
Auditory brainstem response test
The morphology and latency of the waveforms of the auditory brainstem response (ABR) test have been used for prognosis of hearing preservation. The absence of a response is associated with a low chance of hearing preservation, whereas a measurable response has no prognostic significance. Shelton and colleagues reported that hearing was preserved in 78% of patients with an interaural wave V latency difference of less than 0.4 ms, and in only 50% of those with no measurable ABR response. More recently, Brackmann and colleagues also showed a significant difference between the mean latency of the interaural wave V latency for patients with preserved hearing compared with those who lost their hearing. The prognostic significance of ABR has been confirmed by other studies, whereas a few have found no relationship.
Tumor location
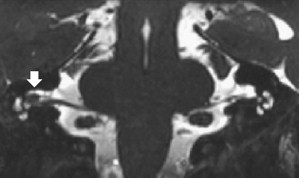
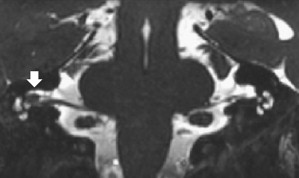
It is generally accepted that the chances of hearing preservation are better in tumors arising from the superior vestibular nerve as opposed to those of the inferior vestibular nerve. The inferior vestibular nerve shares the inferior compartment of the IAC with the cochlear nerve, and hence tumor adhesion to the cochlear nerve is more likely. In addition, the MFC approach allows the unroofing of the IAC and a direct view of tumors in the superior compartment, whereas the transverse crest of the IAC may obstruct the view to the lateral inferior compartment. Greater tumor adhesion to the cochlear nerve and blind surgical dissection in the inferior compartment carry a risk of injury to the cochlear nerve fibers and the vascular supply to the labyrinth. The preoperative identification of the nerve of origin is therefore an important prognostic consideration. The nerve of origin of small intracanalicular tumors may be identified with MRI ( Fig. 1 ); however, this may not be possible for larger tumors.
Vestibular tests for nerve of origin
Two vestibular tests have been used for the preoperative identification of the nerve of origin. The caloric test of electronystagmography assesses the function of the lateral semicircular canal, which is innervated by the superior vestibular nerve. Low caloric responses represent involvement of the superior vestibular nerve, whereas normal caloric function is considered to represent sparing of this nerve and inferior vestibular nerve involvement. Consequently, hearing preservation was reported in 64% of patients with a hypoactive response and in only 45% of those with normal caloric responses. Another vestibular test that indicates involvement of the inferior vestibular nerve and hence may have some prognostic usefulness is the vestibular-evoked myogenic potential (VEMP) test. VEMP testing reflects function of the saccular branch of the inferior vestibular nerve, and absent responses may represent tumor involvement of this nerve. However, the prognostic significance of the VEMP in acoustic neuroma surgery has not been evaluated in large series.
Tumor Factors
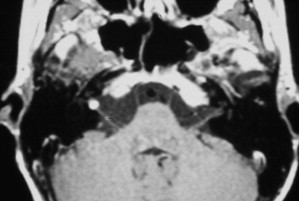
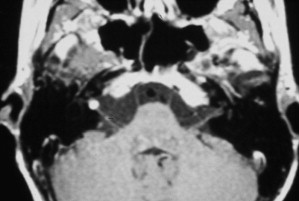
High-resolution, thin-cut MRI with and without gadolinium provides critical information for selection of the optimal surgical approach. The medial extension of the tumor into the cerebellopontine angle and the depth to which the tumor occupies the fundus of the IAC are important parameters for approach selection and prognosis of hearing preservation. The MFC approach is best suited for small intracanalicular tumors with less than 1 cm extension into the cerebellopontine angle that do not contact the brainstem ( Fig. 2 ). The standard MFC offers only limited exposure of the posterior cranial fossa for tumor dissection and intraoperative hemostasis. Tumors of the cerebellopontine angle and intracanalicular tumors with more than 1 cm of medial extension into the cerebellopontine angle are more suitable for a retrosigmoid craniotomy approach.
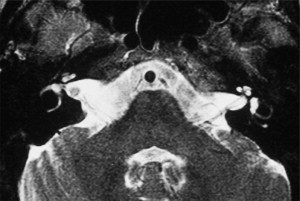
The degree of lateral extension of the tumor into the fundus of the IAC is best seen on T2-weighted sequences of MRI, which can show the bright signal of cerebrospinal fluid (CSF) lateral to the tumor at the fundus ( Fig. 3 ). One to 2 mm of room between the tumor and the fundus of the IAC has been associated with a greater chance of hearing preservation. A lower rate of hearing preservation in tumors that completely fill the IAC compared with cases in which the lateral end of the canal seems uninvolved has been reported.
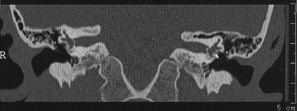
Given the anatomic variability of the petrous bone, information about the degree of pneumatization and amount of bone overlying the superior semicircular canal is helpful when planning an MFC. This fact is shown best with a high-resolution CT with images in the plane of (Poschel) or perpendicular to (Stenver) the superior semicircular canals ( Fig. 4 ).
Patient Factors
The MFC approach involves retraction of the temporal lobe for exposure of the superior petrous bone. Supratentorial craniotomy is associated with higher morbidity in elderly patients (older than 69 years of age). These patients have a dura mater that is thinner and more adherent to the skull than younger patients. Similarly, the rate of medical comorbidities (eg, blood dyscrasia, cerebrovascular disease) increases with age. A recent multicenter, prospective study of complications after craniotomy for meningiomas showed that even after carefully controlling preoperative comorbidities, elderly patients have a poorer outcome than younger patients. Prognostic factors of increased morbidity and mortality after craniotomy include :
- •
Age older than 69 years
- •
Tumor location in the skull base
- •
Peritumoral brain edema
- •
American Society of Anesthesiologists (ASA) class greater than II
- •
Karnofsky performance scale score less than 60
Summary of Patient Selection for Middle Fossa Surgery
The benefits, postoperative care, results, potential complications, and alternatives of the MFC should be thoroughly discussed with the patient. Small intracanalicular vestibular schwannomas can be managed with MFC, stereotactic radiation, or observation; treatment should be selected only after the patient has had the opportunity to consider the pros and cons of each modality. The other surgical methods are discussed in other articles in this issue, and the treatment must be individualized. Newly diagnosed patients may benefit from an initial period of observation, with periodic scanning. Because tumor growth and function deterioration is highly variable, the demonstration of tumor growth through imaging or clinical deterioration supports the need for intervention. The indications of the MFC in cases of unilateral vestibular schwannomas are shown in the following sections. Treatment selection in patients with tumors in the only hearing ear and in neurofibromatosis type 2 (bilateral acoustic tumors) is not as straightforward and is discussed separately in the section Surgery in the Only Hearing Ear and in Neurofibromatosis Type 2 . In general terms, the MFC is indicated for removal of unilateral vestibular schwannomas in patients with
- 1.
Intracanalicular tumors extending less than 1 cm into the cerebellopontine angle, without brainstem contact
- 2.
Good hearing (better than or near 30 dB PTA and 70% WRS)
- 3.
Imaging (MRI) evidence of tumor growth and/or functional deterioration (eg, progressive hearing loss, disabling vertigo)
- 4.
No contraindications for a supratentorial craniotomy (ie, age >69 years, ASA class >II, and Karnofsky Performance Scale score <60)
Indications for surgery
With the current increase in the use of MRI, the identification of small (<1.5 cm) tumors in patients with normal or near-normal hearing also has been on the rise. Today’s skull base surgeons face the dilemma of selecting among three different therapy options for small and minimally symptomatic tumors: microsurgical removal, stereotactic radiation, and observation. During the initial evaluation of patients, surgeons must consider several audiometric, tumor, and patient factors to determine the risk of intracranial surgery, chances of function preservation, and long-term quality-of-life issues. MFC should be offered only for patients who have the best chance of serviceable hearing preservation, and when the risk/benefit analysis is favorable and accepted by the informed patient.
Audiometric Factors
Preservation of serviceable hearing
The goal of MFC is to achieve tumor removal and preserve auditory function that will be useful to the patient long-term. Useful, or “serviceable,” hearing can only be preserved if it is present preoperatively. The definition of serviceable hearing must be individualized, because it depends on several factors, such as audiometric values of the ipsilateral and contralateral ears, progression of hearing loss, patient preference, and available strategies of hearing loss habilitation. Preservation of binaural hearing is important for sound localization and speech understanding in noise; for a patient to benefit from binaural hearing, the interaural average four-frequency (0.5, 1.0, 2.0, and 3.0 kHz) hearing threshold should be less than 20 dB, and the interaural word discrimination score should be less than 20%. The determination of serviceable hearing in a patient with a tumor in the only hearing ear or in patients with bilateral tumors is obviously very different; some patients would choose to keep their hearing at any level even if it only provides sound awareness. The surgeon’s must ensure that the patient has appropriate expectations, habilitation options are available, and the overall quality of life is not placed at risk in exchange for the promise of some measurable auditory function.
From the audiometric standpoint, hearing is characterized by the combination of the four-frequency pure-tone threshold average (PTA) and the word recognition score test (WRS). What is considered serviceable hearing and a definition of success in hearing preservation in some centers is PTA and WRS values of at least 30 dB and 70%, respectively, and in other centers at least 50 dB and 50%, respectively. Hearing aid benefit is limited below the 50/50 level. Because some hearing may be lost immediately or gradually after surgery, and better preoperative hearing has been associated with better chances of early and long-term hearing preservation, it seems intuitive that hearing preservation surgery should be offered only to patients with hearing well above the 50/50 level. The 50/50 level of hearing represents the minimum serviceable hearing and, if preserved at or above this level, allows patients the use of amplification if needed.
Audiologic prognostic parameters beyond preoperative hearing function
Several prognostic signs for hearing preservation have been studied but, except for good preoperative hearing, most of these lack sufficient sensitivity and specificity to be reliable.
Auditory brainstem response test
The morphology and latency of the waveforms of the auditory brainstem response (ABR) test have been used for prognosis of hearing preservation. The absence of a response is associated with a low chance of hearing preservation, whereas a measurable response has no prognostic significance. Shelton and colleagues reported that hearing was preserved in 78% of patients with an interaural wave V latency difference of less than 0.4 ms, and in only 50% of those with no measurable ABR response. More recently, Brackmann and colleagues also showed a significant difference between the mean latency of the interaural wave V latency for patients with preserved hearing compared with those who lost their hearing. The prognostic significance of ABR has been confirmed by other studies, whereas a few have found no relationship.
Tumor location
It is generally accepted that the chances of hearing preservation are better in tumors arising from the superior vestibular nerve as opposed to those of the inferior vestibular nerve. The inferior vestibular nerve shares the inferior compartment of the IAC with the cochlear nerve, and hence tumor adhesion to the cochlear nerve is more likely. In addition, the MFC approach allows the unroofing of the IAC and a direct view of tumors in the superior compartment, whereas the transverse crest of the IAC may obstruct the view to the lateral inferior compartment. Greater tumor adhesion to the cochlear nerve and blind surgical dissection in the inferior compartment carry a risk of injury to the cochlear nerve fibers and the vascular supply to the labyrinth. The preoperative identification of the nerve of origin is therefore an important prognostic consideration. The nerve of origin of small intracanalicular tumors may be identified with MRI ( Fig. 1 ); however, this may not be possible for larger tumors.
Vestibular tests for nerve of origin
Two vestibular tests have been used for the preoperative identification of the nerve of origin. The caloric test of electronystagmography assesses the function of the lateral semicircular canal, which is innervated by the superior vestibular nerve. Low caloric responses represent involvement of the superior vestibular nerve, whereas normal caloric function is considered to represent sparing of this nerve and inferior vestibular nerve involvement. Consequently, hearing preservation was reported in 64% of patients with a hypoactive response and in only 45% of those with normal caloric responses. Another vestibular test that indicates involvement of the inferior vestibular nerve and hence may have some prognostic usefulness is the vestibular-evoked myogenic potential (VEMP) test. VEMP testing reflects function of the saccular branch of the inferior vestibular nerve, and absent responses may represent tumor involvement of this nerve. However, the prognostic significance of the VEMP in acoustic neuroma surgery has not been evaluated in large series.
Tumor Factors
High-resolution, thin-cut MRI with and without gadolinium provides critical information for selection of the optimal surgical approach. The medial extension of the tumor into the cerebellopontine angle and the depth to which the tumor occupies the fundus of the IAC are important parameters for approach selection and prognosis of hearing preservation. The MFC approach is best suited for small intracanalicular tumors with less than 1 cm extension into the cerebellopontine angle that do not contact the brainstem ( Fig. 2 ). The standard MFC offers only limited exposure of the posterior cranial fossa for tumor dissection and intraoperative hemostasis. Tumors of the cerebellopontine angle and intracanalicular tumors with more than 1 cm of medial extension into the cerebellopontine angle are more suitable for a retrosigmoid craniotomy approach.
The degree of lateral extension of the tumor into the fundus of the IAC is best seen on T2-weighted sequences of MRI, which can show the bright signal of cerebrospinal fluid (CSF) lateral to the tumor at the fundus ( Fig. 3 ). One to 2 mm of room between the tumor and the fundus of the IAC has been associated with a greater chance of hearing preservation. A lower rate of hearing preservation in tumors that completely fill the IAC compared with cases in which the lateral end of the canal seems uninvolved has been reported.
Given the anatomic variability of the petrous bone, information about the degree of pneumatization and amount of bone overlying the superior semicircular canal is helpful when planning an MFC. This fact is shown best with a high-resolution CT with images in the plane of (Poschel) or perpendicular to (Stenver) the superior semicircular canals ( Fig. 4 ).
Patient Factors
The MFC approach involves retraction of the temporal lobe for exposure of the superior petrous bone. Supratentorial craniotomy is associated with higher morbidity in elderly patients (older than 69 years of age). These patients have a dura mater that is thinner and more adherent to the skull than younger patients. Similarly, the rate of medical comorbidities (eg, blood dyscrasia, cerebrovascular disease) increases with age. A recent multicenter, prospective study of complications after craniotomy for meningiomas showed that even after carefully controlling preoperative comorbidities, elderly patients have a poorer outcome than younger patients. Prognostic factors of increased morbidity and mortality after craniotomy include :
- •
Age older than 69 years
- •
Tumor location in the skull base
- •
Peritumoral brain edema
- •
American Society of Anesthesiologists (ASA) class greater than II
- •
Karnofsky performance scale score less than 60
Summary of Patient Selection for Middle Fossa Surgery
The benefits, postoperative care, results, potential complications, and alternatives of the MFC should be thoroughly discussed with the patient. Small intracanalicular vestibular schwannomas can be managed with MFC, stereotactic radiation, or observation; treatment should be selected only after the patient has had the opportunity to consider the pros and cons of each modality. The other surgical methods are discussed in other articles in this issue, and the treatment must be individualized. Newly diagnosed patients may benefit from an initial period of observation, with periodic scanning. Because tumor growth and function deterioration is highly variable, the demonstration of tumor growth through imaging or clinical deterioration supports the need for intervention. The indications of the MFC in cases of unilateral vestibular schwannomas are shown in the following sections. Treatment selection in patients with tumors in the only hearing ear and in neurofibromatosis type 2 (bilateral acoustic tumors) is not as straightforward and is discussed separately in the section Surgery in the Only Hearing Ear and in Neurofibromatosis Type 2 . In general terms, the MFC is indicated for removal of unilateral vestibular schwannomas in patients with
- 1.
Intracanalicular tumors extending less than 1 cm into the cerebellopontine angle, without brainstem contact
- 2.
Good hearing (better than or near 30 dB PTA and 70% WRS)
- 3.
Imaging (MRI) evidence of tumor growth and/or functional deterioration (eg, progressive hearing loss, disabling vertigo)
- 4.
No contraindications for a supratentorial craniotomy (ie, age >69 years, ASA class >II, and Karnofsky Performance Scale score <60)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


