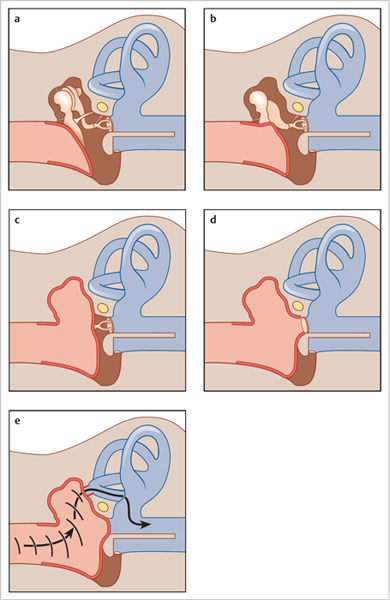
5 Middle Ear Surgery • Consider the hearing in the other ear, comorbidity, and patient’s wishes; great caution in operating on the better-hearing ear • When considering the risks of ear surgery, weigh up against the risks of leaving the condition untreated; e.g., lifetime risk of developing an otogenic intracranial abscess ~1:200 but poor evidence that surgery lessens this risk • Modified radical mastoidectomy (MRM) or canal wall down mastoidectomy: • Combined approach tympanoplasty or canal wall up mastoidectomy: • Atticoantrostomy or front-to-back surgery: • Revision mastoidectomy: • Complications: • Operation to eradicate disease in the ME with or without TM reconstruction • Myringoplasty: operation to repair TM without removal of disease from the ME • Modified Wullstein classification (Fig. 5.1):
5.1 General Considerations for Ear Surgery
5.2 Cholesteatoma Surgery
 Preserves remnants of tympanic membrane (TM) and ossicular chain, keeping eustachian tube orifice covered (as distinct from radical procedure)
Preserves remnants of tympanic membrane (TM) and ossicular chain, keeping eustachian tube orifice covered (as distinct from radical procedure)
 Leaves open mastoid cavity
Leaves open mastoid cavity
 Cavity problems minimized by creating well-saucerized small cavity, covering middle ear (ME) mucosa with TM remnant, keeping facial ridge low, and creating adequate meatoplasty for ventilation and access
Cavity problems minimized by creating well-saucerized small cavity, covering middle ear (ME) mucosa with TM remnant, keeping facial ridge low, and creating adequate meatoplasty for ventilation and access
 Often necessitates long-term aural toilet and water exclusion; may be more difficult to create well-fitting hearing aid (HA) mold or reconstruct hearing by ossiculoplasty
Often necessitates long-term aural toilet and water exclusion; may be more difficult to create well-fitting hearing aid (HA) mold or reconstruct hearing by ossiculoplasty
 Preservation of ear canal wall with posterior tympanotomy to allow for access to facial recess
Preservation of ear canal wall with posterior tympanotomy to allow for access to facial recess
 Requires second-look surgery to exclude residual disease (found in up to 20% of cases), so need to be medically fit for at least two general anaesthetics and have reliable follow-up
Requires second-look surgery to exclude residual disease (found in up to 20% of cases), so need to be medically fit for at least two general anaesthetics and have reliable follow-up
 Use of potassium titanyl phosphate laser can help reduce residual disease rate and allow for ossicular chain preservation to preserve hearing
Use of potassium titanyl phosphate laser can help reduce residual disease rate and allow for ossicular chain preservation to preserve hearing
 Diffusion-weighted magnetic resonance imaging techniques may allow for detection of residual disease and so prevent unnecessary second-look procedures
Diffusion-weighted magnetic resonance imaging techniques may allow for detection of residual disease and so prevent unnecessary second-look procedures
 In the long term, no need for continued aural toilet or water exclusion; may allow for better ossiculoplasty results and easier HA fitting
In the long term, no need for continued aural toilet or water exclusion; may allow for better ossiculoplasty results and easier HA fitting
 For more limited attic disease can allow for disease removal with a small cavity
For more limited attic disease can allow for disease removal with a small cavity
 Can be extended to an MRM
Can be extended to an MRM
 A problem cavity may be improved by lowering facial ridge, obliterating cavity, closing TM perforation, or creating larger meatus
A problem cavity may be improved by lowering facial ridge, obliterating cavity, closing TM perforation, or creating larger meatus
 If no hearing, consider subtotal petrosectomy and blind sac closure
If no hearing, consider subtotal petrosectomy and blind sac closure
 Much the same as for untreated disease: deafness, dizziness, facial palsy
Much the same as for untreated disease: deafness, dizziness, facial palsy
 Taste disturbance, sigmoid sinus bleed, semicircular canal fistula
Taste disturbance, sigmoid sinus bleed, semicircular canal fistula
5.3 Tympanoplasty
 In children, generally consider after ~8 years of age, once grown out of childhood ear conditions
In children, generally consider after ~8 years of age, once grown out of childhood ear conditions
 Type 1: reconstruction TM with intact and mobile ossicular chain (myringoplasty)
Type 1: reconstruction TM with intact and mobile ossicular chain (myringoplasty)
 Type 2: absent malleus handle; TM reconstructed over malleus remnant and long process incus
Type 2: absent malleus handle; TM reconstructed over malleus remnant and long process incus
 Type 3: no incus/malleus; TM reconstructed to lie on stapes head (myringostapediopexy)
Type 3: no incus/malleus; TM reconstructed to lie on stapes head (myringostapediopexy)
 Type 4: stapes footplate present; exteriorized, exposed in mastoid cavity; TM reconstructed over round window to create baffle
Type 4: stapes footplate present; exteriorized, exposed in mastoid cavity; TM reconstructed over round window to create baffle
 Type 5: fixed footplate; fenestrate lateral Scc
Type 5: fixed footplate; fenestrate lateral Scc
 Type 6: sono-inversion; TM reconstructed over oval window (baffle) with round window uncovered
Type 6: sono-inversion; TM reconstructed over oval window (baffle) with round window uncovered
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


