22 Microscopic versus Endoscopic Transsphenoidal Pituitary Surgery
 Historical Perspective
Historical Perspective
Surgical approaches to the sella turcica have interested both the neurosurgeon and otolaryngologist since the early 1900s. Davide Giordano initially proposed a transglabellar-nasal approach to the sella turcica using anatomical studies.1,2 Based on the work of Giordano, Hermann Schloffer performed the first successful transsphenoidal resection of a pituitary tumor in 1907 via a three-stage lateral rhinotomy approach.3,4 In this approach, Schloffer performed a nasal skin incision that extended to the glabella and allowed for the nose to be reflected laterally. This approach was modified in 1909 by Theodor Kocher, who performed a submucosal resection of the nasal septum. Kocher’s technique included a complicated external nasal incision that resulted in improved cosmetic results as compared with those of his predecessors. Since the endonasal approach was initially described by Oskar Hirsch, the utility of the transsphenoidal approach to both sellar and parasellar lesions has grown in analogous fashion to our understanding of the tumor pathology as well as to advances in technology.4,5
Hirsch fashioned his endonasal surgical technique, avoiding the external nasal incision, after his mentor M. Hajek, who described a surgical approach to treat sphenoid sinusitis. In 1910, Hirsch performed his first endonasal approach on a patient with visual loss secondary to a pituitary lesion. The surgical resection of the lesion was performed over 5 weeks and in five different stages, each under local anesthesia, that included a middle turbinectomy, resection of the ethmoid air cells, an anterior sphenoidotomy, resection of the sellar floor, and finally resection of the pituitary lesion with subsequent improvement in vision.6,7 Hirsch subsequently modified his approach based on the submucosal technique of Kocher to decrease the operative time. In addition, he added the nasal speculum to both retract the mucosal flaps laterally and maintain exposure.4,5
Harvey Cushing’s first transsphenoidal operation used a modified version of Schloffer’s approach in a patient with acromegaly. The approach resembled a technique that was later described by Ottokar Chiari in 1912, in which an external incision was performed in the superomedial aspect of the orbit followed by a wide ethmoidectomy.8,9 Cushing later modified his technique based on the surgical approach described by Albert E. Halstead (Fig. 22.1). In 1912, Halstead described a sublabial gingival incision to allow for increased exposure of the sphenoid sinus.8,10 In 1921 Cushing stated, “It is certain that no method is applicable for all conditions of pituitary tumor and that for some no satisfactory procedure has been devised.”3,11 Despite success with the transsphenoidal approach, Cushing exclusively used the transfrontal approach by 1929 for pituitary lesions, noting that chiasmal compression was more effectively relieved under the direct vision provided by the latter procedure.3
Following Cushing’s example, the majority of neurosurgeons followed suit in abandoning the transsphenoidal approach. Hirsch, however, continued to defend the role of transsphenoidal surgery in treating pituitary lesions.5 Norman Dott learned the transsphenoidal approach from Cushing and continued to operate on pituitary lesions via the transsphenoidal route long after his mentor had abandoned the approach. In 1956, Gerard Guiot observed Dott performing the transsphenoidal resection of a pituitary lesion in two patients. Based on this experience as well as a review of Dott’s results with the approach, Guiot adopted the transsphenoidal approach in his own surgical practice and introduced an invaluable adjunct, intraoperative radiologic control.7
The resurgence of the transsphenoidal approach in North America was closely related to the work of Jules Hardy, who worked for 1 year under the tutelage of Guiot and during that time developed an appreciation for the transsphenoidal approach. To improve intraoperative visualization, Hardy introduced the surgical microscope to provide both illumination and magnification.7 Based on this improved visualization, he was able to identify a cleavage plane between the tumor and the normal gland. Using this plane, he introduced the concept of the selective microadenomectomy in which removal of such a lesion could be accomplished without affecting the function of the normal gland. With the combination of the microscope and intraoperative fluoroscopic guidance, Hardy was able to remove a variety of sellar and parasellar lesions with less morbidity and mortality than that seen with the transcranial approach.8
The first neurosurgeon to use the endoscope in a transsphenoidal approach was Guiot, who abandoned the instrument secondary to inadequate visualization.8 The use of the endoscope to assist in microscopic transsphenoidal surgical procedures was not again reported until 1977 by Apuzzo et al12 and soon thereafter by Bushe and Halves13 in 1978. Jankowski et al14 subsequently reported in 1992 the role of a pure endoscopic transsphenoidal approach to the sella turcica. The pioneers of the latter technique for resecting pituitary adenomas include Hae Dong Jho, a neurosurgeon, and Ricardo Carrau, an otolaryngologist, at the University of Pittsburgh Medical Center (UPMC). In addition, Amin Kassam, a neurosurgeon at UPMC, has looked to expand the role of the endoscope for the resection of skull base lesions outside of the sella turcica. Significant contributions to both the surgical technique as well as the surgical instruments for the pure endoscopic approach are attributed to neurosurgeons and otolaryngologists in North America and Europe.15

Fig. 22.1 The sublabial approach of Harvey Cushing. Original drawing by Max Brodel displaying a mouth gag, a sponge in the posterior nasopharynx to prevent aspiration, and a tongue depressor apparatus to administer ether anesthesia. (From Cushing H. Surgical experiences with pituitary disorders. JAMA 1921;76:1721–1726. Reprinted with permission.)
 Sinonasal Anatomy
Sinonasal Anatomy
The goal of any surgical procedure is to minimize morbidity while maximizing surgical success. An understanding of the sinonasal anatomy is critical in reaching this goal. Effective mucociliary movement is critical for maintaining mucous flow toward the sinus ostia and onto the nasopharynx. Blockage of this flow can result in stagnation of mucus within the sinus and subsequent sinusitis.16
The corridor to access the sphenoid sinus is between the middle turbinate and the nasal septum. Anterior to the middle turbinate, the drainage sites for the frontal, anterior ethmoid, and maxillary sinuses converge. The sphenoethmoidal recess is located between the rostrum of the sphenoid sinus and the inner aspect of the middle turbinate and serves as the confluence of drainage for the posterior ethmoid and sphenoid sinuses. Consequently, preservation of the anatomy anterior and lateral to the middle turbinate is critical to maintaining the normal drainage pathways of the paranasal sinuses. Therefore, both the approach used to access the sphenoid sinus and the manner of closure are important in minimizing morbidity.16
 Endonasal Pituitary Surgery
Endonasal Pituitary Surgery
The transsphenoidal approach has continued to be developed to allow for maximal tumor resection with minimal morbidity and mortality. The primary goals in resecting functioning pituitary microadenomas include eliminating tumor mass and minimizing risk of recurrence, normalization of hormone hypersecretion, and preservation of pituitary function. The resection of pituitary macroadenomas has similar goals, with the addition of removing mass effect on vital structures, such as the optic chiasm.17 The aforementioned goals can best be accomplished by using an operative approach that minimizes the morbidity secondary to the surgical approach while at the same time maximizing the visualization of the sellar and parasellar regions. The operative microscope has been a key component to the successful resection of a variety of these sellar and parasellar lesions by providing three-dimensional visualization of the surgical field.18 In an effort to improve visualization, the endoscope has become a valuable tool in transsphenoidal resection of pituitary lesions.
Patient Positioning
Patients are positioned such that the surgeon can comfortably access the sphenoid sinus and sella turcica and minimize intraoperative bleeding. Although a variety of positions are used, we advocate a lawn-chair—type position for both the endoscopic and microscopic approaches. Venous congestion is consequently minimized, allowing for increased venous drainage and decreased bleeding. The traditional position used by the otolaryngologist places the surgeon at the head of the table with the patient positioned supine. Although this improves surgeon comfort, this supine position does not allow for the reduced venous congestion offered by the lawn-chair—type position.19
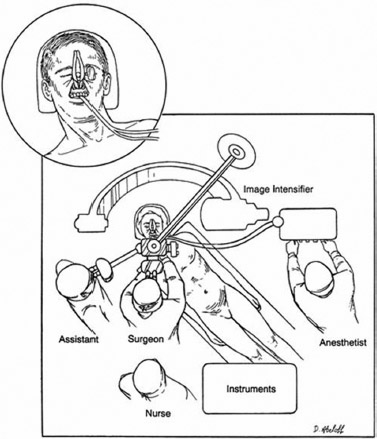
Fig. 22.2 Operating room setup and patient positioning for the microscopic transsphenoidal approach. The magnified drawing of the patient’s head displays the sublabial approach with the nasal speculum in place. (From Elias WJ, Laws ER Jr. Transsphenoidal approaches to lesions of the sella. In: Schmidek HH, Sweet WH, eds. Operative Surgical Techniques: Indications, Methods, and Results, Vol 1, 4th ed. Philadelphia: WB Saunders, 2000:373–384. Reprinted with permission.)
The patient’s head is positioned in a Mayfield horseshoe headrest and flexed laterally. For ease in producing an accurate lateral radiograph with intraoperative fluoroscopy, the bed is positioned such that the patient’s head is parallel to the walls of the room and the nasal dorsum is parallel to the floor. In addition, the bed is placed in reverse Trendelenburg position such that the thorax is situated at approximately a 30-degree angle above the horizontal. The bed is also tilted slightly to the surgeon, both to prevent the surgeon from leaning over the patient and to improve the patient’s lateral neck rotation (Fig. 22.2). As the patient’s head is not fixed to the operative table, this position can be subtly manipulated intraoperatively. This is more pertinent in microscopic surgery in which the surgeon can rotate the head to look laterally instead of moving the microscope.19
Nasal Preparation
The nasal preparation begins preanesthesia with intranasal oxymetazoline sprays. Once the patient is in the operating room, immediately after intubation and prior to positioning, additional oxymetazoline should be applied intranasally. After the patient is positioned, the nares and maxilla are first washed with chlorhexidine antiseptic solution. The middle turbinate and septum may be injected with 1:200,000 epinephrine. In the sublabial approach, the mucosa overlying the maxilla is also injected. Cotton patties, soaked in either oxymetazoline or epinephrine, are placed between the middle turbinate and the septum for the purpose of hemostasis. Following draping, the patties are removed. For the endoscopic approach, the nasal preparation is perhaps more important as even small amounts of bleeding can make the exposure difficult.
Surgical Approaches
The manner in which the surgeon accesses the sphenoid sinus can be broadly divided into endonasal and sublabial approaches. Traditionally, both endonasal and sublabial approaches were performed using submucosal tunnels. Some surgeons have advocated an endonasal direct sphenoidotomy.20 This approach and its variants have the benefit of fewer anterior septal complications and a more rapid access to the sphenoid sinus. However, the width of the expo sure (and therefore the field of view and maneuverability of instruments) progressively decreases from the sublabial to the endonasal transseptal to the endonasal direct sphenoidotomy.19,21
Following exposure of the sphenoid sinus and completion of the anterior sphenoidotomy, the surgeon must decide the required sellar and parasellar exposure to adequately resect the tumor. The traditional microscopic exposure involves only removal of the anterior wall of the sella turcica. A chisel and mallet or drill may be used to gain initial access to the sellar dura followed by use of the Kerrison punch. Often the sellar bone has been thinned by the tumor and can be easily out-fractured. The goal of bony removal is to expose the dura just medial to the medial surface of the cavernous segment of the carotid artery bilaterally. As the carotid protuberances most often cannot be completely visualized with the microscopic approach, this bony removal requires the combination of direct visualization and surgical feel with the Kerrison punch (Fig. 22.3). Inferiorly the bone forming the sellar floor should be removed and superiorly the bony opening should reach the inferior border of the superior intercavernous sinus. For larger tumors extending toward the anterior cranial fossa, an extended transsphenoidal approach can be of value. In this approach, the bony opening is extended beyond the anterior wall of the sella turcica to include the planum sphenoidale.21–23
Our pure endoscopic technique has evolved over time from attempting to recapitulate a mononostril microscopic approach to a more practical binostril approach. There has also been a shift from using an endoscope holder to using a threehand technique. One of the primary advantages of using the latter approach is the pseudo–three-dimensional surgical view that can be generated by movement of the endoscope during the operation.24
For initial exposure, the surgeon uses a two-hand technique (Fig. 22.4) with the 0-degree short endoscope for dissection to the sphenoid ostia. The right nostril is typically used for this purpose, unless a septal deviation significantly decreases the working room, requiring use of the left nostril. The middle turbinate is then identified and carefully lateralized with the use of a suction spatula. The surgeon must be careful to minimize damage to the normal mucous drainage pathway as described above.24

Fig. 22.3 Microscopic operative view following an anterior sphenoidotomy. The sellar dura (SD) is exposed to the cavernous sinus bilaterally; however, the microscope’s line of sight limits direct lateral visualization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


