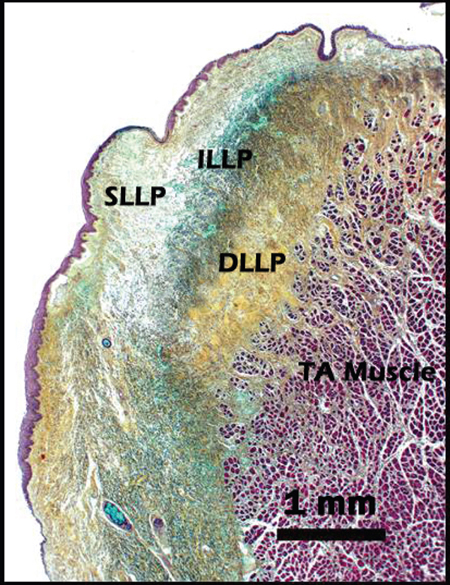
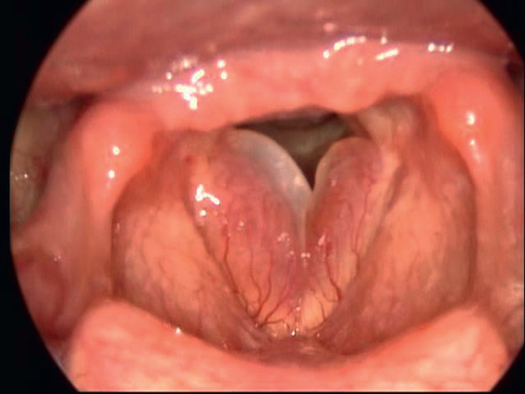
3 Microanatomy and Cellular Physiology The human vocal folds are unique structures. The microanatomy of these structures dictates the fluidity of the vibration and the quality of sound they produce. An understanding of vocal fold histology and cellular physiology is necessary to understand, diagnose, and treat pathology of the vocal folds. Hirano elegantly described the unique multilayered structure of the vocal folds in 1974 (Fig. 3.1).1 This layered structure has relevance not only in the maintenance of the mechanical properties of the vocal folds but also in the development of benign vocal lesions. These layers include the epithelium, the lamina propria, and the vocalis muscle. The lamina propria is further subdivided into superficial, intermediate, and deep layers. Each layer has distinct structural and mechanical properties that contribute to the characteristic vibration seen on laryngeal videostroboscopy or high-speed videography. An understanding of the structure and the varying mechanical properties of each layer is necessary to fully understand vocal fold vibration. Figure 3.1 Coronal section of the human vocal fold. Movat stain highlights layers of the lamina propria. DLLP, deep layer of the lamina propria; ILLP, intermediate layer of the lamina propria; SLLP, superficial layer of the lamina propria; TA, thyroarytenoid. The epithelium of the vocal folds is composed of stratified squamous cells that maintain the shape of the vocal folds. The remainder of the glottis, however, has ciliated pseudocolumnar epithelium. Unlike most squamous cells, such as normal skin, the vocal fold epithelium remains metabolically active throughout its life cycle. The surface cells slough off into the laryngeal lumen as new cells migrate superiorly and medially to replace them. The luminal cells exhibit a “microridge” pattern, thus increasing the surface area to better maintain the mucus blanket that covers the vocal fold surface. This bilayer mucus blanket is vital to ensure adequate moisture and lubrication of the vocal folds. The luminal layer of the blanket is mucinous. This layer, which is primarily composed of mucin molecules, is the thicker of the two layers and acts to prevent dehydration of the surface epithelium. The inner, serous layer is thinner due to its higher water content. This layer is in direct contact with the squamous cells of the vocal fold epithelium and the cilia of the pseudocolumnar cells of the glottis and facilitates the mucociliary transport of secretions up from the trachea and through the glottis for expectoration. Inhibition of mucociliary clearance can lead to impaired function of the upper respiratory tract. The epithelium is secured to the lamina propria by the basement membrane zone (BMZ). This zone is a collection of protein and nonprotein structures and is composed of two layers, the lamina lucida and the lamina densa. The lamina lucida is the low-density, clear zone medial to the basal epithelial cells, while the lamina densa is a zone of increased type IV collagen fibers adjacent to the lamina propria. These two layers provide structural support, connecting the epithelium to the underlying lamina propria through anchoring fibers.2 The BMZ is also essential for repair and maintenance of the epithelium. Chronic disruption of this layer may lead to the formation of a vocal fold nodule.3 Clinical Insight The BMZ is an area of clinical importance to differentiate between carcinoma in situ (CIS) and invasive carcinoma of the vocal folds. CIS of the vocal fold is defined as the presence of atypical cells within the epithelial layer of the vocal fold without evidence of invasion through the BMZ. Once cancerous cells infiltrate the BMZ, the process becomes invasive and the risk of regional and distant metastases increases. Therefore, great care must be taken to dissect below the BMZ when performing a biopsy of a suspicious vocal lesion to ensure that the correct diagnosis is made. The superficial layer of the lamina propria (SLLP), or Reinke space, is a potential space composed of loose, fibrous tissue in an extracellular matrix (ECM). It is extremely pliable and often compared to soft gelatin. Owing to its structure, the SLLP offers little resistance to vibration. The ECM is the key component of the SLLP that allows this motion. The ECM is a mixture of fibrous and interstitial proteins that serve as a scaffold for the SLLP. It provides strength and resilience in allowing the vocal fold to vibrate freely, while allowing the SLLP to maintain its structure. The fibrous proteins, namely collagen type I and elastin, provide the tensile strength needed to maintain the SLLP, while the interstitial proteins, such as hyaluronic acid, decorin, and versican, provide the viscoelastic characteristics of the vocal fold for vibration.2 These interstitial proteins also give the vocal fold the ability to absorb the shock of repeated impact from phonation. Understanding the microanatomy and the mechanical properties of this layer is extremely important as the majority of benign vocal fold lesions occur in this layer. Vocal fold polyps, nodules, cysts, and polypoid corditis, or Reinke edema, all form in the SLLP.4 Hyaluronic acid, or hyaluronan, is perhaps the most important of the ECM proteins. It is a glycosaminoglycan polymer of disaccharides composed of repeating units of glucuronic acid and acetylglucosamine.5 Owing to its high charge at physiologic pH, hyaluronic acid readily binds water to form a gel-like substance that affects the viscoelasticity of the lamina propria, determining tissue viscosity, osmosis, and flow resistance.6 This most likely determines the biomechanics of vocal fold vibration. Clinical Insight Polypoid corditis, or Reinke edema, most often occurs in the setting of heavy cigarette smoking and, less often, in severe hypothyroidism. Patients typically complain of lowered vocal pitch. Physical examination with indirect laryngoscopy reveals varying degrees of edema of the vocal folds due to the abnormal accumulation of fluid in the SLLP (Fig. 3.2). The marked edema likely occurs as a response to the chronic irritation of the cigarette smoke or as a manifestation of myxedema in the setting of hypothyroidism. This edema typically involves the entire membranous vocal fold from the vocal process to the anterior commissure, causing it to become floppy. Increased mucosal wave is observed on laryngovideostroboscopy. The fundamental frequency during phonation is decreased due to the increased mass of the affected vocal fold, according to the equation ω = √(k/m), where ω is frequency, k is constant, and m is mass. The initial treatment for polypoid corditis is to remove the chronic irritant, in the case of smoking, or to correct the hormone deficiency, as in hypothyroidism. If a patient continues to have significant dysphonia despite these measures, surgical treatment may be considered. Typically, microflap excision is performed to remove the excess SLLP and redundant mucosal cover. More recently, angiolytic lasers have been used to treat polypoid corditis in-office. Occasionally, extensive bilateral disease may cause airway compromise. Surgical treatment should occur in this setting despite the patient’s smoking status. The intermediate layer of lamina propria (ILLP) and the deep layer of lamina propria (DLLP) together comprise the vocal ligament, or the transition layer between the overlying epithelium and the SLLP and the underlying vocalis muscle. The ILLP comprises roughly one-half of the lamina propria and contains a high concentration of reticular type III collagen fibers. It is less densely organized than the DLLP, which is composed of type I and type III collagen fibers that penetrate the superficial bundles of the vocalis muscle.7 The vocal ligament is the free, superior margin of the conus elasticus, which is an elastic membrane that connects the cricoid cartilage to the thyroid and arytenoid cartilages. The ILLP is thickened at the anterior and posterior ends of the membranous vocal fold. These areas are known as the anterior and posterior macula flava. The anterior macula flava serves as a transition zone between the stiffthyroid cartilage and the pliable membranous vocal fold, while the posterior macula flava serves as a transition between the membranous vocal fold and the stiff vocal process of the arytenoid cartilage.8 This structure allows for the support of increased tensile stress that occurs in vocal tasks that require high-pitched sounds. The vocal ligament is a key landmark for the depth of dissection of a benign laryngeal lesion in laryngeal microflap surgery. Once the epithelium has been incised and the SLLP bluntly elevated, the vocal ligament appears laterally as a shiny, yellow-white strip of elastic tissue. Figure 3.2 Polypoid corditis.
Vocal Fold Histology
Epithelium
Superficial Layer of the Lamina Propria
Intermediate and Deep Layers of the Lamina Propria
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


