Purpose
To investigate the relationship between metamorphopsia and macular morphologic changes after successful repair of rhegmatogenous retinal detachment (RD).
Design
Prospective, interventional, consecutive study.
Methods
The study included 129 eyes of 129 patients who had undergone successful retinal reattachment surgery. The severity of metamorphopsia was recorded using M-CHARTS and foveal microstructure was assessed with spectral-domain optical coherence tomography (OCT) at 6-12 months postoperatively.
Results
The mean metamorphopsia score was 0.30 ± 0.46, and 50 of 129 patients (39%) had metamorphopsia. Metamorphopsia was more severe in eyes with macula-off rhegmatogenous RD than those with macula-on ( P < .001). Eighteen of 50 eyes with metamorphopsia exhibited abnormal structures in the macular region (epiretinal membrane, disruption of the photoreceptor inner and outer segment junction, cystoid macular edema, macular hole, or subretinal fluid), whereas the other 32 eyes showed no morphologic changes with OCT. In these 32 eyes, the horizontal metamorphopsia score (0.86 ± 0.50) was significantly higher than the vertical metamorphopsia score (0.62 ± 0.39, P < .05). Nine of 69 eyes with preoperative macula-on rhegmatogenous RD developed postoperative metamorphopsia. Of the 9 eyes, 6 showed abnormal macular structures and the other 3 had normal-appearing OCT. The macula briefly detached during vitrectomy in these 3 cases.
Conclusions
In eyes that remained macula-on throughout surgery and had normal-appearing OCT, metamorphopsia did not develop. In some cases, the reason for metamorphopsia was anatomically obvious. In other cases that were preoperative and intraoperative macula-off, postoperative retinal vertical displacement could cause predominantly horizontal metamorphopsia.
The effectiveness of rhegmatogenous retinal detachment (RD) surgery has generally been assessed by the rates of retinal reattachment and the postoperative visual acuity. Even after successful retinal reattachment and improvement of visual acuity, however, the postoperative quality of vision may be unsatisfactory in some cases. Metamorphopsia is one of the most common postoperative symptoms in patients with RD, with 22%-33% of patients complaining of metamorphopsia by questionnaire. Wang and associates investigated 46 patients with macula-off rhegmatogenous RD undergoing scleral buckling surgery and found that 67% of them had metamorphopsia on the Amsler grid at 2 months postoperatively.
Recent advancement in optical coherence tomography (OCT) technologies has provided critical insights into the various retinal conditions. The development of spectral-domain OCT enhances the resolution with which the intraretinal architectural morphology, such as the ganglion cell layer (GCL), inner nuclear layer (INL), outer plexiform layer (OPL), outer nuclear layer (ONL), photoreceptor inner and outer segment junction (IS/OS), and external limiting membrane (ELM), can be clearly seen. Studies using OCT revealed that the visual acuity in RD patients deteriorated because of disruption of the IS/OS, disruption of the ELM, disruption of the cone outer segment tips, and thickening of the outer retina.
Few studies, however, have investigated the relation between metamorphopsia and OCT findings. Using the Amsler grid in patients with epiretinal membrane (ERM), Watanabe and associates reported that the INL was thicker in patients with broad metamorphopsia than in those without metamorphopsia. It has also been reported that the severity of metamorphopsia, quantified by M-CHARTS, was strongly associated with the thickness of the INL in patients with ERM. Rossetti and associates examined 7 patients who complained of long-standing metamorphopsia after successful repair of macula-off rhegmatogenous RD and found that all eyes had normal findings on spectral-domain OCT. There is, however, no report quantifying metamorphopsia in rhegmatogenous RD patients and evaluating the relationship between metamorphopsia and detailed OCT findings.
The purpose of the present study was to quantify the severity of metamorphopsia after successful repair of rhegmatogenous RD and to investigate the relationship between metamorphopsia and morphologic changes in the macular region assessed with spectral-domain OCT.
Methods
We analyzed 129 patients after successful surgery for unilateral rhegmatogenous RD undertaken at University of Tsukuba Hospital from October 1, 2010 to April 26, 2012. Their ages averaged 52.3 ± 11.0 years (mean ± SD), and there were 84 male and 45 female patients. We conducted this prospective, interventional, consecutive study in accordance with the Declaration of Helsinki, and received approval from the institutional review committees of University of Tsukuba Hospital. Prior to inclusion in the study, all patients provided informed consent after the nature of the study was explained to them. Exclusion criteria included patients with a previous history of vitreoretinal surgery and ophthalmic disorders except myopia of less than -6 diopters and severe cataract of more than grade 3 nuclear sclerosis or cortical opacity. Eyes with complicated vitreoretinal disease, such as proliferative vitreoretinopathy and RD resulting from giant retinal tears, macular hole, or ocular trauma, were excluded. Patients with logarithm of minimal angle of resolution best-corrected visual acuity (logMAR BCVA) of >0.7 were also excluded because of possible incorrect measurement of the severity of metamorphopsia.
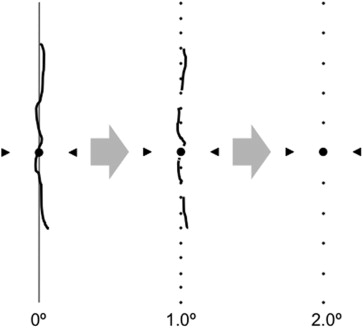
Visual acuity, metamorphopsia, and OCT images were obtained at 6-12 months postoperatively. BCVA measured with the Landolt chart was expressed as logMAR. The severity of metamorphopsia was quantified with M-CHARTS (Inami Co, Tokyo, Japan). M-CHARTS consists of 19 dotted lines with dot intervals ranging from 0.2-2.0 degrees of visual angle. If the straight line is substituted with a dotted line and the dot interval is changed from fine to coarse, the distortion of the line decreases with the increasing dot interval, until the dotted line appears straight. At first, vertical straight lines (0 degrees) were shown to the patient. If the patient recognized a straight line as straight, the metamorphopsia score was 0. If the patient recognized a straight line as irregular or curved, then subsequent pages of M-CHARTS, in which the dot intervals of the dotted line change from fine to coarse, were shown one after another. When the patient recognized a dotted line as being straight, the visual angle that separated the dots was considered to represent his or her metamorphopsia score for vertical lines ( Figure 1 ). Then the M-CHARTS was rotated 90 degrees and the same test was performed with horizontal lines. The examinations were repeated 3 times, and their mean values were used for data analyses. Each examination was performed at 30 cm with the refraction of the eye exactly corrected for this distance. The presence of metamorphopsia was defined as the mean metamorphopsia score (metamorphopsia score) ≥0.2, because the metamorphopsia scores were 0 in all normal subjects.
Retinal images were obtained with spectral-domain OCT (Cirrus high-definition OCT; Carl Zeiss, Dublin, California, USA). We performed the 5-line raster scans in a horizontal and vertical manner for each eye using Cirrus analysis software version 3.0. Scans with signal strength of more than 7/10 were considered to be appropriate, and a representative image was selected. Diagnosis of a disrupted IS/OS was made based on loss and irregularity of the hyperreflexive line corresponding to the IS/OS junction. We also assessed the degree of the ELM disruption in a similar fashion. Two graders (Y.S., T.H.) assessed the status of the IS/OS and the ELM lines. Both graders were masked to the clinical findings of the patients, including their visual acuity and metamorphopsia score results.
Clinical data were collected, including age, sex, surgical procedures, the number of retinal tears, circumferential dimension of retinal tears, area of retinal detachment, and macular status (on/off) ( Table 1 ). We evaluated whether RD existed at the macula region using spectral-domain OCT in all eyes preoperatively.
| Number of eyes | 129 |
| Age (y) | 55.3 ± 11.0 |
| Sex (male/female) | 84/45 |
| Surgical procedures (scleral buckling/vitrectomy) | 31/98 |
| Number of retinal tears | 2.0 ± 1.5 |
| Circumferential dimension of retinal tears (degrees) | 17.9 ± 16.6 |
| Area of retinal detachment (degrees) | 126 ± 73 |
| Macular status (on/off) | 69/60 |
| Preoperative visual acuity (logMAR) | 0.56 ± 0.80 |
| Postoperative visual acuity (logMAR) | 0.05 ± 0.18 |
| Postoperative metamorphopsia score (M-score) | |
| Horizontal M-score | 0.30 ± 0.50 |
| Vertical M-score | 0.31 ± 0.49 |
| Mean M-score | 0.30 ± 0.46 |
All surgeries were performed at our clinic by 2 experienced vitreoretinal surgeons (F.O., Y.O.). In eyes with cataract of grade 2 nuclear sclerosis or cortical opacity, the crystalline lens was removed by phacoemulsification and an acrylic foldable intraocular lens was implanted in the capsular bag, followed by vitrectomy. The surgical technique comprised a 23- or 25-gauge pars plana vitrectomy that released vitreous traction around the breaks, internal drainage of the subretinal fluid, a total gas-fluid exchange with 20% sulfur hexafluoride (SF 6 ), and laser photocoagulation. When scleral buckling was performed, cryopexy and an exoplant (segmental silicone sponges in combination with an encircling silicone band) were used to support the retinal breaks. Subretinal fluid drainage and SF 6 gas injection were performed when required. In both treatment groups, patients injected with gas were instructed to maintain a face-down position during the first postoperative week.
The mean and standard deviations were calculated for metamorphopsia score and other parameters. The Student t test was performed to compare age, the number of retinal tears, circumferential dimension of retinal tears, and area of retinal detachment between patients with and without metamorphopsia. Differences in sex, surgical procedures, and macula status between patients with and without metamorphopsia were analyzed by the Fisher exact probability test. A logistic regression analysis was performed to determine parameters significantly relevant to the presence of metamorphopsia. Wilcoxon signed rank test was used to compare horizontal and vertical metamorphopsia scores. All tests of associations were considered statistically significant if P < .05. We carried out the analyses using StatView (version 5.0; SAS Inc, Cary, North Carolina, USA).
Results
The mean metamorphopsia score of all patients was 0.30 ± 0.46, while horizontal and vertical metamorphopsia scores were 0.30 ± 0.50 and 0.31 ± 0.49, respectively. There was no significant difference between horizontal and vertical metamorphopsia scores ( P = .81). The mean metamorphopsia score ranged from 0.0-2.0 ( Figure 2 ). Fifty of 129 patients (39%) had metamorphopsia (metamorphopsia score ≥0.2). Forty-one of 60 eyes with macula-off rhegmatogenous RD (68%) and 9 of 69 eyes with macula-on rhegmatogenous RD (13%) had metamorphopsia. Patients with macula-off rhegmatogenous RD showed a significantly higher incident of metamorphopsia than those with macula-on rhegmatogenous RD ( P < .0001). Patients with metamorphopsia had a larger area of retinal detachment ( P < .0001) than those without metamorphopsia. Age ( P = .16), sex ( P = .71), surgical procedures ( P = .39), the number of retinal tears ( P = .33), and circumferential dimension of retinal tears ( P = .50) showed no association with either the presence or absence of metamorphopsia. In logistic regression analysis, postoperative metamorphopsia score was significantly associated with macula-off rhegmatogenous RD ( P < .0001), whereas other parameters were not relevant ( Table 2 ).
| β | SE | P Value | |
|---|---|---|---|
| Age (y) | 0.00 | 0.03 | .79 |
| Surgical procedures (scleral buckling/vitrectomy) | 0.00 | 0.66 | .98 |
| Number of retinal tears | 0.08 | 0.17 | .85 |
| Circumferential dimension of retinal tears (degrees) | 0.00 | 0.02 | .67 |
| Area of retinal detachment (degrees) | 0.00 | 0.01 | .89 |
| Macular status (on/off) | 0.35 | 0.62 | <.0001 a |
Figure 3 shows OCT findings in eyes with metamorphopsia. Of the 50 eyes, 6 eyes had ERM, 5 eyes had disruption of IS/OS, 3 eyes had cystoid macular edema (CME), and 2 eyes had macular hole (MH) and 2 eyes with persistent subretinal fluid (SRF), while the other 32 eyes exhibited no abnormal morphologic change. In these 32 eyes, the horizontal metamorphopsia score (0.86 ± 0.50) was significantly higher than the vertical metamorphopsia score (0.62 ± 0.39, P < .05) ( Figure 4 ).



