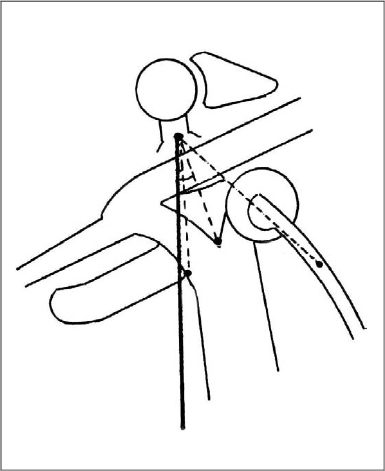
34 MCF Surgery Using Cochleariform Process as the Main Landmark MCF surgery using cochleariform process as the main landmark. Using the cochleariform process (CP) as a reliable landmark in middle cranial fossa surgery either alone, or in conjunction with other landmarks: The vertical crest lies at a 20° angle from the CP to the coronal plane, and at a distance of 5–6mm from the CP; the point where the medial margin of the basal turn of the cochlea crosses the labyrinthine segment of the facial nerve is at a 0° angle from the CP to the coronal plane, and at a distance of 6.5–7.5mm from the CP; additionally the superior semicircular canal is at a 45° angle from the CP to the coronal plane. Middle cranial fossa surgery. The main steps of the middle cranial fossa approach are similar in all described techniques, including the CP technique. The techniques differ mainly in the landmarks used, which result in differences during the final, yet most delicate stage of the procedure. In the CP technique, in contrast to the other approaches, the tegmen tympani is opened first. After the head of malleus, body of incus, and the cochleariform process have been exposed, the meatal plane is drilled in a mediolateral direction beginning 10–12mm medially to the CP, with the center of drilling located directly medial (slightly posteromedial) to the process, which is the anticipated position of the vertical crest. The drilling process continues with ease up to a point about 7–8mm from the CP, as neither cochlea, vestibule, nor labyrinthine facial nerve extend more medially. After reaching this point, more delicate work is required. Drilling carefully, the vertical crest is sought at a 20° angle from the CP to the coronal plane, and at a distance of 5–6mm from the CP, also keeping in mind the other CP-related clues. The CP may be used as the sole landmark or along with other landmarks. If it is used as the only landmark, continuous irrigation and magnification are essential to be able to observe the slightest color change, i.e., the blue discoloration that indicates the reflection of the superior semicircular canal, vestibule, or basal turn of cochlea; or the pink discoloration that indicates the reflection of the labyrinthine facial nerve, to prevent damage to these structures. If Garcia-Ibanez’s direct medial approach to the meatal porus is used, the proposed landmark provides safety, as the surgeon can determine where the critical structures lie and work safely medial to these structures. If House’s original approach is used, the proposed landmark enables the surgeon to bypass the delicate middle part of the labyrinthine segment, finding the vertical crest directly after exposing the distal part of the labyrinthine segment, and ultimately unroofing the middle part or leaving it intact, which reduces the risk of facial nerve damage. If Fisch’s approach is used, the proposed landmark not only gives more information about the location of the internal auditory canal and vertical crest, but also defines exactly where the blue line of the superior semicircular canal should be sought, which has no other clue indicating its location in the arcuate eminence. Definitions and Tips
Definition
Indications
Surgical Technique
MCF Surgery Using Cochleariform Process as the Main Landmark
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


