31 Managing Postoperative Sinusitis
Postoperative care of the nasal and paranasal sinuses after endoscopic pituitary and skull base surgery is based on many of the well-established principles in endoscopic sinus surgery for inflammatory disease. The chief goals include maximizing wound healing, restoring mucociliary clearance, maintaining ostia patency, preventing scar formation, and avoiding rhinosinusitis.1 Although all of the above-mentioned goals are important, none is more critical than the preservation and rapid healing of the skull base. This is important to prevent serious complications such as cerebrospinal fluid (CSF) leaks, tension pneumocephalus, and meningitis.2,3
The otolaryngologist plays a crucial role in promoting wound healing of the skull base reconstruction during the postoperative period. Excessive crusting and rhinosinusitis secondary to impaired mucociliary clearance, synechia formation, and obstruction of sinus ostia may occur without adequate surveillance and intervention. Medical management includes saline irrigation, topical or oral antibiotics, nasal steroid sprays, decongestants, and mucolytics. In addition, postoperative nasal endoscopy with debridement is imperative for enhancing sinonasal healing and preventing sinonasal complications. Proper medical and surgical management of the sinonasal cavity provides the best opportunity for rapid and safe healing after endoscopic skull base surgery.
 Sinonasal Management
Sinonasal Management
Postoperative management of the sinonasal cavity is individualized based on the operative intervention and the patient’s wound-healing capabilities. The surgical approach, extent of surgery, presence of an intraoperative CSF leak, complexity of skull base reconstruction, and the patient’s comorbidities help to guide the postoperative management strategy. For example, extended transplanum, transtuberculum approaches to resect sellar-suprasellar pituitary macroadenomas require a greater amount of postoperative sinonasal care than resection of smaller intrasellar pituitary microadenomas. More extensive surgical dissection through the sinonasal cavity often requires a longer amount of time for wound healing and establishment of mucociliary clearance. Most approaches for pituitary adenomas require limited dissection, and therefore no more than 4 to 6 weeks is required for complete wound healing. Patient comorbidities such as diabetes, chronic renal failure, and chronic steroid use may prolong healing of the sinonasal cavity and skull base. Skull base reconstruction with biomaterials may prolong postoperative healing compared with the use of a vascularized pedicled flap (Fig. 31.1). A meticulous mucosa-preserving surgical approach usually results in decreased crusting, scarring, and obstruction of natural sinus ostia. Finally, rare intraoperative or postoperative complications such as bleeding, rhinosinusitis, and CSF leaks may also alter the postoperative management of the sinonasal cavity.
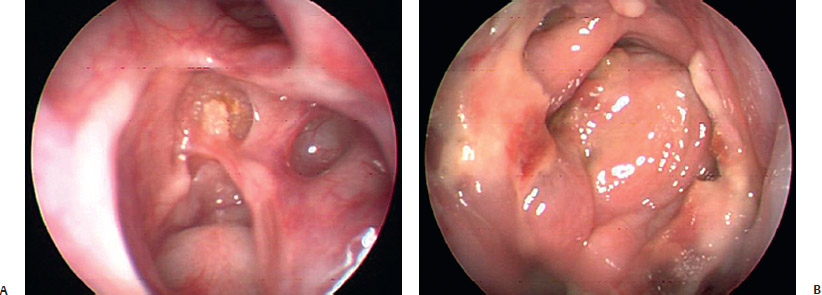
Fig. 31.1 (A) Incomplete mucosalization of the skull base at 6 weeks after skull base reconstruction with a biomaterial implant. (B) Healing of the skull base at 2 weeks after skull base reconstruction with a vascularized nasoseptal flap for an extended approach to a pituitary adenoma.
 Perioperative Management
Perioperative Management
The vast majority of patients after endoscopic pituitary and skull base surgery are admitted to the intensive care unit in the immediate postoperative period for observation. These patients often require frequent neurologic examinations, occasional lumbar drainage management, and monitoring for diabetes insipidus, CSF leaks, and pneumocephalus. Telfa nasal packs are placed anteriorly in the nasal cavities to wick blood in the immediate postoperative period. These packs are removed 24 to 48 hours after the surgical procedure, preferably prior to obtaining the postoperative magnetic resonance imaging (MRI). The head of the bed is kept elevated, usually no more than 30 degrees from the supine position. Ice packs are placed around the nose and face for comfort as needed. A face tent provides mist humidification to the sinonasal cavity and decreases patient discomfort. Nasal cannulae are strictly avoided during the postoperative period. Delivery of oxygen through a nasal cannula has the potential of causing a tension pneumocephalus, a serious and potentially devastating complication of endonasal, intracranial approaches (Fig. 31.2). Nasal sprays and irrigation should be avoided during the first postoperative week because they may cause bleeding or displace materials used for skull base reconstruction.
All patients are given perioperative antibiotics for 24 to 48 hours after surgery. A series of 90 patients undergoing endoscopic skull base surgery who received a single dose of perioperative antibiotics yielded no cases of intracranial infections or meningitis.4 These results are encouraging because skull base reconstruction entails transport of the grafts (fat, fascia lata, Medpor [Porex, Newnan, GA]) though the nasal cavity, considered to be a contaminated field. The potential ramifications of infection in these patients include meningitis, intracranial abscesses, and vascular compromise.
Patients are advised to avoid nose blowing, sneezing with their mouth open, sipping through straws, and heavy lifting or other strenuous activity, to adhere to a bowel regimen of stool softeners, and to avoid any maneuvers that may increase their intracranial pressure. Patients are also instructed to avoid hot showers to prevent vasodilation of intranasal vessels and subsequent bleeding. Patients are usually discharged with a prescription for an antibiotic and pain control along with a follow-up appointment with the otolaryngologist in 1 week.
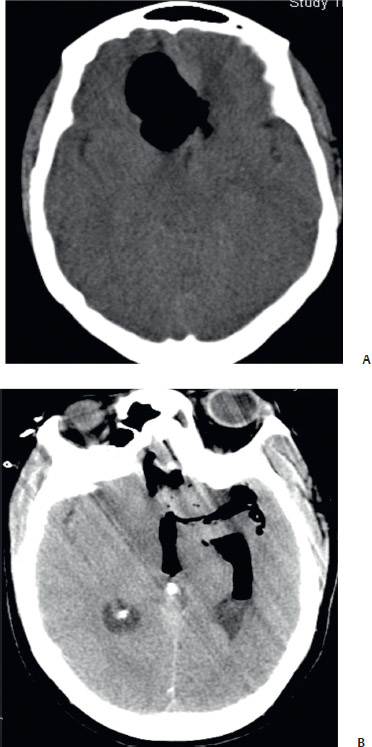
Fig. 31.2 Delivery of oxygen with nasal cannula after endoscopic skull base surgery resulted in (A) tension pneumocephalus at the base of the frontal lobe, which may enter into (B) the subarachnoid space and intraventricularly.
 Postoperative Management
Postoperative Management
Postoperative sinonasal care begins with the otolaryngologist, approximately 1 week after discharge from the hospital. Gentle postoperative endoscopic debridement of the sinonasal cavity is performed. This includes removing crusting, old blood, mucoid secretions, and breakdown products from hemostatic agents and tissue. The sphenoid sinus cavity is carefully inspected for a CSF leak, and secretions are gently suctioned, without instrumenting the skull base. Any crusting along the reconstruction site is left in place until subsequent visits when the scabs are no longer adherent to the skull base. Scabs are never aggressively debrided from the skull base in the early postoperative visits as this may precipitate bleeding or a CSF leak.
Vestibular sores or abrasions to the nasal ala and vestibule are extremely rare. However, if present, they should be treated with local wound care and topical antibiotic ointmeant. Patients are also placed on a gentamicin nasal spray (80 mg in 1000 mL of saline) three times a day for 4 weeks to decrease mucosal edema and bacterial colony count, as well as to improve nasal mucociliary function and nasal hygiene.5 Systemic absorption of intraoperative gentamicinnasal irrigation has been studied and appears to be below systemic therapeutic levels.6 Patients are typically seen in the office 3 and 6 weeks after discharge from the hospital. Follow-up visits consist of postoperative sinonasal debridements, lysis of synechia, and examination of the skull base. A cranial nerve exam is performed in addition to evaluate for meningeal signs or symptoms as well as the presence of CSF rhinorrhea. Extended skull base approaches require more frequent and lengthier postoperative follow-up visits to remove crusting and ensure good mucosal healing.
 Management of Sinonasal Complications Bleeding
Management of Sinonasal Complications Bleeding
Postoperative bleeding rarely requires intervention if meticulous hemostasis is maintained intraoperatively. In our series of pituitary and anterior skull base cases, there was a 2% incidence of postoperative epistaxis. Minor postoperative bleeding is expected and usually does not require any treatment other than mist humidification and frequent changing of the nasal drip pad. In rare cases, a moderate amount of bleeding may be controlled with placement of a hemostatic matrix or intranasal packing. Endoscopic visualization of the origin is recommended for expedient hemostatic control and to avoid jeopardizing the skull base reconstruction. In some circumstances, if the patient is cooperative, local anesthesia and electrocautery can be applied under endoscopic guidance to control the bleeding. If the bleeding is brisk, located deeper in the nasal cavity, and difficult to identify despite endoscopic visualization, controlling the hemorrhage in the operating room is preferable. This is particularly important in the immediate postoperative period, given the risk of displacing the skull base reconstruction materials if a nasal pack is placed without adequate visualization. More-over, although rare, depending on the extent of intracranial dissection especially within the cavernous sinus, unidentified bleeding deep in the nasal cavity may represent an intracranial source.
In endoscopic pituitary surgery, particular attention must be directed to the posterior nasal and posterior septal branches off the sphenopalatine artery. For extended transethmoidal, transcribriform, or transorbital procedures, attention should be directed to branches of the anterior and posterior ethmoidal arteries. Suspected bleeding from the ethmoidal arteries necessitates immediate evaluation of the eye to rule out a retrobulbar hematoma. In the extremely rare event of a sentinel bleed suggestive of bleeding from the carotid artery, immediate intranasal packing and insertion of a Foley balloon should be initiated to tamponade the bleed. A hemodynamically stable patient should be taken emergently for angiography. An unstable patient should be emergently taken to the operating room for carotid ligation.
Crusting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


