33 Managing Postoperative CSF Leak
Endoscopic endonasal approaches (EEAs) to the pituitary and parasellar regions have been refined and expanded over the past decade.1–11 These approaches often create complex and high-flow cerebrospinal fluid (CSF) defects in the dura and skull base. Endoscopic reconstruction of such defects was one of the major challenges of endoscopic endonasal skull base surgery in early case series. Depending on reconstructive technique, tumor type, and surgical approach, rates of postoperative CSF leak vary from 5% to as high as 75%.12–15 Development of vascularized reconstruction techniques such as the nasal septal mucosal flap16,17 have lowered these rates to levels similar to those of open approaches.
Sequelae of postoperative CSF leak include meningitis, abscess, and pneumocephalus. Nonclinical sequelae include prolonged hospitalization and increased cost of care. Early repair may help to prevent these sequelae. However, it can be challenging to determine whether or not a patient is actively leaking in the postoperative period. Most postoperative CSF leaks do not become apparent until nasal packing is removed. Rarely, late CSF leaks will occur (weeks to months following surgery) as a consequence of patient activity, excessive debridement, or adjunctive therapy.
The reasons for a postoperative CSF leak are multiple and varied. The most common reasons for failure include high-flow defects, increased intracranial pressure, unsuitable reconstructive material, improper placement of a flap, inadequate recipient bed, and disruption of the repair. There are limited data regarding the optimal treatment strategy for patients with postoperative CSF leak.
 Risk Factors for Postoperative CSF Leak
Risk Factors for Postoperative CSF Leak
There are several factors that seem to contribute to higher postoperative CSF leak rates. These factors may be related to the disease (Cushing’s disease leading to obesity and poor healing) anatomical site (involvement of arachnoid cisterns or ventricles), reconstructive technique, adjuvant therapies, patient comorbidities (obesity, poor nutrition), or the patient’s strenuous activities.
Diseases such as Cushing’s disease create a disastrous milieu for surgery. Patients are overweight, heal poorly, and are at high risk for perioperative complications such as deep venous thrombosis or cardiac ischemia. As a result, skull base defects require meticulous repair in these settings. We prefer vascularized repair such as a nasoseptal mucosal flap16,17 even when treating small tumors because of these factors. Fat grafts are also less suitable in these patients because of poor quality of the fat.
Suprasellar, clival, or parasellar tumors often involve the basal arachnoid cisterns. Resultant wide dissection within these cisterns creates an open space for rapid transit of CSF. This may be one reason that these tumors have a higher risk of a postoperative CSF leak.14,15 Additionally, increased mixture of blood and CSF intraoperatively contribute to postoperative elevations of CSF pressure. Certainly, tumors such as craniopharyngiomas that extend into the third ventricle create a unique challenge for reconstruction (Fig. 33.1). Once again, a vascularized mucosal flap is preferred over avascular reconstructive techniques for separation of a direct communication between the ventricles and paranasal sinuses.
Although small dural defects can be reliably reconstructed using a variety of techniques and materials,18,19 large or high-flow defects are more demanding. We have observed the greatest success with a combination of an inlay collagen graft and an onlay septal mucosal flap. Alternative vascularized reconstructions may be used when a septal flap is not available. There are many technical factors to consider in performing the reconstruction. These include preparation of the recipient bed, elevation of the flap, placement of the flap, protective coverings (fibrin glue, synthetic glue), and support of the flap (nasal packing, balloon catheter).
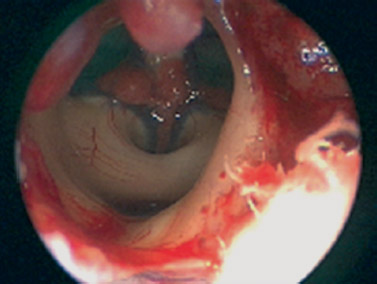
Fig. 33.1 Endoscopic view of the third ventricle following endoscopic endonasal resection of a craniopharyngioma. The resultant direct communication between the ventricular system and sinus cavity presents a unique challenge for reconstruction.
Adjuvant treatments such as chemotherapy or radiation can delay or halt postoperative healing. Occasionally, irradiation can lead to necrosis of a well-healed skull base repair. A vascularized repair should be strongly considered when the patient has received prior radiation therapy or the pathology requires postoperative irradiation. A sufficient period of time should pass following preoperative chemotherapy before performing skull base surgery to allow white cell counts to recover. Conversely, postoperative chemotherapy should not be started until healing is complete (minimum of 2 to 3 weeks).
Patient comorbidities should also be considered. Obesity is known to be a risk factor for occult hydrocephalus. It is hypothesized that increased central venous pressure secondary to high intra-abdominal pressure contributes to increased intracranial pressure. In addition, patients of any body habitus can suffer from malnutrition, leading to poor healing. If this is suspected, preoperative prealbumin levels should be checked and, if possible, optimized prior to elective skull base surgery.
 Detection of Postoperative CSF Leak
Detection of Postoperative CSF Leak
As with any complication, there is no substitute for direct examination of the patient for detection. Reliable patients are able to detect constant, unusual postnasal drainage and may complain of a gagging sensation or frequent cough. It can have an oddly salty or sweet flavor for the patient. This is different from the thick and sometimes vaguely foul-smelling or foul-tasting typical postoperative drainage. Most patients with this history can be tested with direct provocation. This involves having the patient lean forward, with the head lowered, to observe nasal drainage. Unilateral drainage that is clear and watery is usually CSF, but postoperative nasal washes, vasomotor rhinitis, and the CSF/sinus reservoir effect can all provide false positives. Nasal endoscopy may provide clear documentation of a CSF leak, but many leaks are missed due to the absence of drainage with the patient upright and the difficulty of visualizing the operative site. This can often be performed in the clinic or at the bedside.
A reliable adjuvant test is β2-transferrin (β2T) testing. β2T is a protein found almost exclusively in CSF.20
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


