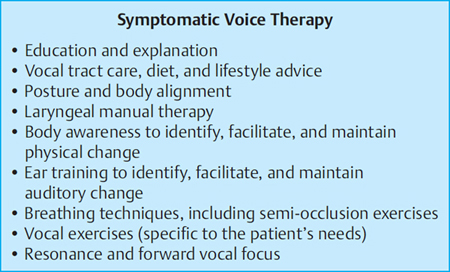
17 Management of Voice Disorders: Key Principles of Speech–Language Therapy The practice of speech–language therapy includes the application of procedures and principles for measurement, testing, identification, counseling, or instruction related to the development and disorders of communication, voice, and swallowing. Speech–language counseling therapists (SLTs) follow an undergraduate or postgraduate courses and graduate with a science-based qualification. The courses and clinicians are regulated by a professional body, for example, American Speech-Hearing-Language Association in the United States or the Royal College of Speech and Language Therapists and the Health Professions Council in the United Kingdom. Clinicians who specialize in the treatment of voice disorders do not undergo specific training to become voice specialists. There are a few postgraduate courses that offer training in voice pathology to ENT surgeons and SLTs, but most clinicians acquire their experience “on the job.” SLTs who specialize in the treatment of individuals with voice disorders work in collaboration with the laryngologist. They are concerned with understanding, assessing, and modifying vocal behaviors. SLTs do not provide medical diagnosis or treatment; neither do they provide vocal training that would enhance the aesthetic quality of voice. Rather, they are primarily concerned with the “pathological” aspect of a voice problem in one or more physical, perceptual, or behavioral components. In most countries, the general family doctor is the first “port of call” available to an individual with a voice problem. The family medical practitioner may prescribe a course of antibiotics, and if the problem persists, he may refer the patient to an ENT specialist. The current preferred practice is to assess voice disorders in voice clinics, based on a constructive partnership between ENT specialists and SLTs. Voice clinics provide more detailed and accurate information on the vocal tract and vocal function,1 which is very useful to the treating SLT. The ENT surgeon has the prime responsibility for examining the larynx and for making the appropriate diagnosis; however, increasingly, SLTs undertake special training that enables them to visualize the larynx in parallel or therapy clinic.2 This enables them to examine the impact of voice therapy on vocal function and to consider how they may alter their therapeutic approach on the basis of “live” evidence.3 The goal of the voice assessment is to establish a set of parameters that describe voice quality and voice use, and to relate these parameters to a well-designed treatment.4 Voice therapy aims to assist the dysphonic patient to return to a realistically achieved voice quality that will satisfy his or her emotional, occupational, and vocational needs. Achieving this objective depends on the patient’s anatomic, physiological, and psychological capabilities that may require the involvement of the multidisciplinary voice team and, of course, the patient’s ability to understand his or her vocal limitations. The initial voice therapy session usually consists of case history taking. The aim of this initial clinical interview is to explore the history of the patient’s presenting symptoms. This session often determines the success of the speech therapy intervention, which depends on the clinician’s skill to put the patient at ease and to manage their expectations, emotions, and understanding of their problem.5 During the case history taking, the clinician aims to explore the patient’s perspective on the nature of their voice problem and how it affects their life. We seek to learn about the onset of the current episode and how it developed over time, the consistency of voice quality and other associated symptoms, for example, vocal fatigue or laryngeal discomfort. Questions are asked about voice use/vocal load and about the manner/intensity of voice use in a professional/vocational, social, and recreational context. Armed with this information, the clinician may carry out the following assessments: Auditory perceptual assessment is a primary tool for voice clinicians. Similarly, the effectiveness of voice therapy is judged by patients and their families on the basis of their auditory perception.6 The GRBAS scheme developed by Hirano7 is the most commonly used rating scheme in voice disorders. The listener is required to rate the severity of five parameters using a four-point scale: 0 (normal); 1 (mild); 2 (moderate); and 3 (severe). The vocal attributes rated are as follows: G—grade, which represents the overall severity of the voice disorder; R—roughness, which represents the overall degree of irregularity of vocal fold vibrations, heard as harshness; b—Breathiness, which corresponds to the “air leakage” heard on phonation; A—asthenia, perceived as vocal weakness; and S—strain heard as hyperfunctional or effortful quality. GRBAS is considered a useful tool for clinicians working with voice disorders; it is simple to use, easy to learn, and yields high inter-rater reliability.8 Another scheme, used particularly in the United States, is the CAPE-V (consensus auditory-perceptual evaluation of voice), proposed by the American Speech-Language and Hearing Consensus Conference. The CAPE-V rates six vocal attributes: overall severity, roughness, breathiness, strain, pitch, and loudness. It uses a visual analogue scale on which the parameters are scored on a continuous scale, rather than the discrete four-point scale used in GRBAS. Evidence showed that this adaptation enables the scorer to note small differences within and among subjects.9 It also makes this scheme a useful tool in research. Both informal and formal auditory perceptual evaluations provide the SLT with valuable information about the quality and severity of the voice disorder, as well the way in which the patient uses the voice. The British Voice Association recommended the use of GRBAS for any clinician working with voice disorders.10 While it is difficult to find an “ideal” auditory perceptual clinical tool, it is important to stress that any voice clinician is expected to use a formal perceptual voice assessment scheme as it facilitates the recording of changes over time and it contributes to standardization of communication among colleagues. The current approach to the assessment of voice disorders involves instrumental assessment.4 Many hardware and software packages (e.g., KayPentax Computerized Speech Laboratory [KayPENTAX, New Jersey, United States] or Laryngograph Speech Studio [Laryngograph Ltd., Greater London, United Kingdom]) offer acoustic analysis and visual feedback of various aspects of speech and voice, which are used by SLTs in their voice therapy work. The acoustic analysis can yield aspects of voicing that may not be detected by the human ear, which would impact voice therapy.11 The visual display can help patients gain further insight into the nature of their voice and helps them adjust their vocal behavior on the basis of what they see on the screen. Instrumentation is also available for the analysis of the interaction between respiration and phonation. This is used by the SLT as part of the diagnostic evaluation, providing measures such as mean airflow rate, estimated subglottic air pressure, and laryngeal valving efficiency. On the whole, there is agreement among clinicians and researchers that there is currently no single acoustic measurement that correlates best to perceived impression, but a combination of acoustic values. So clinicians will have to rely on a combination of assessments until an easy, accurate, and meaningful way of measuring voice quality is evolved. The SLT may carry out other forms of noninstrumental assessments, for example, maximum phonation time, which provides information about the individual’s respiratory function and glottal efficiency on the basis of his or her ability to sustain.12 S/z ratio is used as another test among other tests to sustain a vowel sound.13 SLTs often ask patients to complete health-related questionnaire, exploring the impact of the voice disorder on their life. These questionnaires enable the clinician to identify particular issues related to voice use at work and in social interaction. They may be completed before and after intervention and can be used by the clinician as an outcome measure, demonstrating the effectiveness of intervention. The Voice Handicap Index (VHI)14 is one of the most widely used questionnaires, offering insight into the perceived impact of the voice disorder on the person’s life, and its severity. The shortened modified version of the VHI makes it easy and practical clinical and research tool, with strong reliability and validity. Once the diagnosis and treatment plan have been established, the role of the SLT is to provide the course of voice therapy. The goal of therapy is to restore the best voice possible that would satisfy the individual’s communication, vocational and social needs. The course of therapy would vary in accordance with the laryngeal diagnosis and with patient’s ability to comply with the treatment program. Voice therapy may be conducted in conjunction with other treatment modalities such as physical therapy, for example, in the case of muscle tension dysphonia. If the patient is due to undergo phonosurgery, the SLT should ideally see him or her preoperatively for case history taking and advice regarding the postoperative course of treatment. The first step in voice therapy is patient’s education.4 Helping patients familiarize themselves with normal voice production and understanding the outcome of their laryngeal examination would help them understand their problem and engage them in the treatment process. Vocal hygiene or voice care is one of the principles that is a routine part of every voice therapy program. It includes ideas about the do’s and don’ts of voice care such as limiting talking time and vocal loudness, avoiding speaking against background noise, reducing vocally abusive behaviors such as throat clearing, coughing, and maintaining an adequate level of hydration. Vocal hygiene focuses on healthy use of the vocal apparatus.4 It may include antireflux advice in terms of diet and lifestyle, and voice rest/conservation program, to assist healing. Direct voice therapy consists of exercises targeting specific faulty vocal behaviors that contribute to the dysphonia. Voice therapy moves gradually from one activity to the next while allowing the patient sufficient time for mastering and practicing the technique. As stated by Aronson and Bless,15 “no introduction to voice therapy approaches would be complete without a concomitant discussion of evidence-based medicine.” Although increasingly clinicians are requested to define estimated length of treatment and to provide information about its effectiveness, many treatment approaches used by voice clinicians do not have an evidence base.16 In nonorganic voice disorders involving excess musculoskeletal tension, treatment is based on the principle that reduction in muscle tension allows the larynx to return to its normal phonatory ability. This is achieved by mechanical relaxation of musculature and psychological release of any anxiety causing or associated with the tension. Progression from abnormal to normal voice occurs as a product of the patient’s conscious, voluntary response to the clinician’s instruction and encouragement. In organic disorders, the main principle of therapy is either muscle strengthening or adaptation to the mechanical problems through compensatory phonatory and respiratory maneuvers17 (Fig. 17.1). Figure 17.1 Symptomatic voice therapy.
Initial Referral
The Voice Clinic
Voice Evaluation
Case History
Perceptual Assessment
Laboratory Testing: Instrumental Assessment/Acoustic Analysis
Noninstrumental Voice Evaluation
Patients Rating Scales
Voice Therapy
Vocal Hygiene
Vocal Rehabilitation Techniques
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


