Management of the Congenital and Acquired Anophthalmic Socket
Scott M. Goldstein
Kate Lane
Femida Kherani
The anophthalmic socket is not a common problem ophthalmologists have to encounter. Our time is mostly spent preserving vision, thus it can be difficult when a child is born with an anophthalmic socket or removal of an eye is indicated in older patients. The loss of an eye is a dreaded fear of many adults. Even in the setting of severe eye disease with chronic, unremitting pain, many patients choose to live with the pain rather than lose an eye to enucleation. Certainly enucleation, evisceration, and exenteration surgeries, which are utilized in the setting of irreparable trauma or severe disease, require an adjustment period. In both congenital and acquired anophthalmia, there is an emotional shock to the family or patient that takes time and reassurance as well as the skillful care of a multidisciplinary team to rehabilitate the patient. Ophthalmologists, oculoplastic surgeons, ocularists, and the patient’s primary care provider work in conjunction to see patients through the process of rehabilitation.
This chapter sets out to explore in depth how to approach the socket that is already missing an eye and requires further attention. Both congenital “clinical” anophthalmia and acquired anophthalmia will be discussed. Certainly, it is much more critical to assess and maintain the vision of a seeing eye, but none the less treatment of an unhealthy anophthalmic socket can improve the patient’s quality of life. The congenital anophthalmic socket is more often a severe microphthalmic socket and poses a whole set of issues that significantly differ from acquired anophthalmia. In the later patients, most problems arise from postsurgical complications or chronic changes associated with having a foreign body, the prosthesis, placed in the conjunctiva cul de sac. The issues are many but a methodical approach can usually help patients retain comfort, cosmesis, and self confidence.
Congenital Anophthalmia/Microphthalmia
Congenital anophthalmia and microphthalmia are rare developmental disorders of the globe and secondarily the surrounding ocular adnexa. True anophthalmia is a very rare condition that refers to the complete absence of ocular tissue in the orbit. Ocular adnexa may be, and often are, present in true anophthalmia. The diagnosis of true anophthalmia requires histologic or detailed neuroimaging studies. More often, “clinical anophthalmia” can be applied to cases where clinically the globe appears absent, but neuroimaging does indicate a presence of an ocular remnant.1 Consequently, the term microphthalmia is used more commonly to refer to a spectrum of disorders characterized by a smaller than normal eye based on axial length (Fig. 1). Microphthalmia is classically defined as a condition where the axial length is less than two standard deviations than the average age appropriate globe size.2 Microphthalmia can also be classified based on the axial length measurement as mild, moderate, or severe.3
 Figure 1. Clinical anophthalmia with no obvious eye and significantly reduce ocular adnexa |
Pathophysiology
Anophthalmia and microphthalmia (A/M) are likely due to disturbances in the morphogenetic pathway that controls eye development. It is presumed that the degree of clinical deformity is related to the possible insult at various stages of growth of the optic vesicle. The insult can be primarily genetic or from some external gestational factors like an infection. Embryologically, the globe forms in the first few weeks of gestation. A failure or disruption of this process results in a malformed eye (Fig. 2). Primary anophthalmia is a true failure of the optic vesicle to form from the cerebral vesicle. Secondary anophthalmia occurs from disruption of the neural tube and is usually not compatible with life.4
 Figure 2. Microphthalmic Eye with minimal cornea, 8mm diameter and No vision |
Microphthalmia is a heterogeneous disorder and can occur in an isolated fashion with no other systemic malformation or as part of a well-defined syndrome (Table 1). Simple microphthalmia refers to isolated microphthalmia without any systemic associations. The globe is small but otherwise normal. Complex microphthalmia refers to an eye that is small and has associated abnormalities such as anterior/posterior dysgenesis. When a newborn is found to have microphthalmia, a genetic consultation is prudent.
Table 1: Clinical Genetics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Autosomal dominant, autosomal recessive and x-linked genetic alterations have all been reported.5,6,7,8,9,10,11,12 A variety of gene defects have been reported over the years as our understanding continues to improve. Genes like SOX2, CHX10, POMT1, and Six6 have all been implicated in various syndromes and nonsyndromic causes of congenital anophthalmia/microphthalmia. For example, CHX10 and RAX play a role in retinal differentiation. Defects in these genes probably lead to poor retinal cellular formation and, thus, nonsyndromic, monogenic anophthalmia/microphthalmia. Molecular testing for mutations in genes associated with congenital anophthalmia is clinically available for SIX3, HESX1, BCOR, SHH, PAX6, RAX, CHD7 (CHARGE syndrome), IKBKG (incontinentia pigmenti), NDP (Norrie disease), SOX2 (SOX2-related eye disorders), POMT1 (Walker-Warburg syndrome), and SIX6. Molecular genetic testing for isolated (nonsyndromic) A/M is available on a research basis only. Based on the genetic workup, the family can gain important insight and information as it pertains to the baby and future children. Fortunately, many cases are isolated and sporadic.
Epidemiology
The microphthalmia spectrum of malformation is uncommon. Various studies have analyzed the prevalence of microphthalmia and anophthalmia in different areas of the world. Studies from France and Sweden found a prevalence of 0.2 and 0.27 per 10,000 births respectively.13 In England, data from 1988 to 1994 found an incidence of 1.0 per 10,000 births.14 In Scotland, the prevalence was reported to be 1.9/10,000.15 The Alberta Congenital Anomalies Surveillance System (ACASS) noted an average prevalence for anophthalmia /microphthalmia of 1.4 per 10,000 between 1991 and 2001.16 The prevalence in California of congenital anophthalmia has been found to be 0.18/10,000 births whereas bilateral microphthalmia occurred in 0.22/10,000.17 A more recent study looking at the full spectrum of congenital anophthalmia and microphthalmia in Hawaii found an incidence of 3.2/10,000 births, most of which were microphthalmia.18 Some of the variation in numbers from study to study can be explained by the inclusion/exclusion criteria rather than a true difference in the malformation around the world.
Management
In congenital cases of microphthalmia it is paramount to start by assessing visual potential. Mild cases can be followed and treated with spectacles, patching or other options to maximize visual potential. On the other hand, severe microphthalmia and clinical congenital anophthalmia typically have minimal visual function and are challenging conditions to manage. In addition to the absence of a seeing eye, there are also concerns regarding the possible disfigurement of the eyelid soft tissue, orbit and facial skeleton. Early intervention is recommended with a multidisciplinary team approach. This typically includes an ophthalmologist, oculoplastic surgeon, plastic surgeon, geneticist, pediatrician, and family support services. Parents need to be forewarned about the necessary commitment and lengthy course involved in treating these difficult cases. The International Congenital Anophthalmia Network (www.anophthalmia.org or 1-800-580-ICAN) is an excellent resource for families as is the world craniofacial foundation (www.worldcf.org).
When approaching a patient with microphthalmia, a complete examination and workup in necessary. It is imperative to establish the lack of vision before the long road of conformers, expansion, and prostheses are embarked upon. Often electrophysiologic testing is needed to determine the visual function of the eye. Very small rudimentary globes almost never have any vision. Orbital imaging should also be obtained to help evaluate the globe, orbital structures like extraocular muscles and the size of the bony orbit. With all this information in hand, an appropriate plan can be instituted.
Growth of the orbit and facial skeleton depends on the presence and size of an eye,19,20 thus management of congenital anophthalmia/microphthalmia should be initiated as soon as possible after birth. The first few years of life is a critical time period for potential growth of the orbit and absence of the globe can negatively affect the orbital and consequently facial skeletal development.19 Farkas demonstrated that 80% of skeletal maturation is completed in the first 5 years of life.21
Based on this data, the earlier an intervention is instituted, the easier it is to intervene and the better the outcome. There are three critical areas that are targeted in severe microphthalmic patients: (1) eyelid expansion, both horizontally and vertically, (2) Conjunctival cul-de-sac expansion, and (3) boney orbital expansion. All three are usually treated with any specific treatment.
Traditionally, serial progressively enlarging static acrylic conformers have been used to stimulate orbital and socket growth (Fig. 3). The ocularist is an integral part of the management team and visits to the ocularist can be as frequent as bimonthly in the first year of life to maximally stimulate orbital growth.22 These various conformers must be custom made and fit to the socket and lids being expanded. Initially a conformer on a stem or peg, which is shaped like a collar button, is utilized as it primarily helps with placement and secondarily will exert a horizontal force on the canthi. As the socket grows, these are replaced with more standard shells that continue the expansion process. Once the socket has been expanded to an adequate size with conformers, a dermis fat graft or orbital implant can be used for further socket reconstruction.23
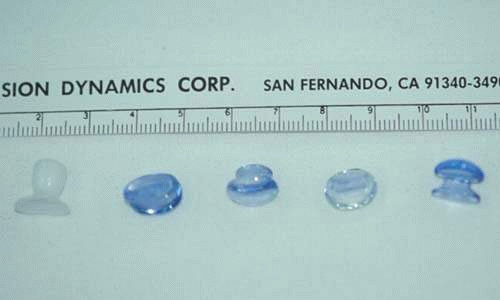 Figure 3. Various conformers used to expand a microphthalmic socket |
Incisional surgery as part of the rehabilitation of the congenital anophthalmic socket is almost never needed and should be approached with great caution. There is always some degree of socket present. Even the smallest socket still has some potential space for conformer placement. If retention is an issue, then a temporary tarsorraphy may be used to help with retention. Caution is required as sutures can erode the lid margins with time when placed under pressure. The tarsorraphy is best reinforced on the external lid surface with bolsters to minimize cheese wiring of the sutures and to help maintain the suture. If the socket still responds poorly to expansion, mucus membrane grafts can be utilized to increase the central socket surface area and help deepen the fornices. Lateral canthotomy is strongly discouraged. This procedure is often counterproductive and ultimately leads to scarring, diminished cosmesis, and more difficult prosthesis retention (Fig. 4). Placing an incision in an area under direct expansion will lead to wound distortion, scarring and often lateral canthal rounding. Further, lateral scarring with shortening of the critical lateral cul-de-sac can prevent prosthesis retention and mobility.
 Figure 4. Child referred secondary to scarring of lateral canthus along with entropion of upper and lower lids in microphthalmic socket after lateral canthotomy performed as infant |
Inflatable orbital expanders have previously been used for orbital volume expansion.24,25,26,27,28 These are similar to other soft tissue expanders and are tunneled in from a distant location. Such tissue expanders are typically placed in the deep orbit with a port in the supra-auricular area tunneled through the lateral orbital wall (Fig. 5a and b). After the socket heals from the initial surgery, the expander is slowly inflated over a few months until it reaches the desired size and effect. At this point, the tissue expander is explanted and a standard orbital implant or dermis fat graft is placed.
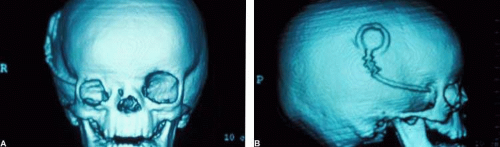 Figure 5. A. 3D CT scan demonstrates location of orbital balloon expander in position. Note small orbital structures on right, microphthalmic side. B. Lateral view. |
More recently, newer osmotic expanders have become popular and revolutionized socket expansion (Fig. 6).29,30,31,32,33,34 Hydrogel Tissue Expanders (Osmed, CA) consist of methylmethacrylate and N-vinylpyrrolidone copolymer, a material that previously has been used in contact lenses and scleral buckles. The hydrogel expander is placed in the socket (in a dehydrated state). It expands via osmosis of surrounding water to a maximum final volume. The product comes in a variety of sizes and is available as hemispheres (0.4 mL, 0.9 mL, 1.5 mL), spheres (2.0 mL, 3.0 mL, 4.0 mL) and pellets. It typically takes 24 hours for the expander to reach full size, which is typically twice the starting diameter and a 10-fold increase in volume.
 Figure 6. Hydrogel sphere in conjunctival cul-de-sac. |
The expander is often placed in the conjuctival cul-de-sac and secured with sutures. The hemispheres have suture tunnels and thus sutures can be run through the implant and out the fornices to the periosteum to secure them (Fig. 7a and b). A tarsorrhaphy also can be performed with sutures or cyanoacrylate glue to minimize the incidence of anterior extrusion of the expander. Glue reduces the risk of tissue injury sometimes encountered with sutures on the delicate lid tissue undergoing expansion. The implant can also be placed in the posterior orbit. The spheres may be placed in the cul-de-sac or surgically implanted in the orbit through a subperiosteal dissection via the lateral canthus or through a subconjunctival approach with a layered closure. Maximum expansion occurs within 24 hours and the expander should be kept in until the soft tissue expands accordingly. After serial expansion is complete, a dermis fat graft can ultimately be placed in the socket. Of note, in cases that are resistant to serial expansion or tissue expanders, craniofacial surgery may be necessary but is rarely needed or utilized.
 Figure 7. A. Hydrogel hemisphere sewn into position. B. Two months later with early tissue expansion. |
In a series of 28 patients with unilateral or bilateral clinical anophthalmia treated at The Children’s Hospital of Philadelphia between 2002 and 2006, the hydrogel orbital expander improved fissure length in 21.5% of patients with placement of the first expander.3 Serial expanders were necessary in the majority of these patients until a maximal dermis fat graft could ultimately be placed in the socket. Schittkowski et al. reported on the use of hydrogel pellets for socket expansion in six patients between the ages of 5 and 42 months with unilateral microphthalmos who were treated by injection of 4 to 14 pellet expanders into the retrobulbar orbital tissue. Volume augmentation was 1 to 3.5 mL. The pellets were injected using a customized trocar and placed behind the microphthalmic eye and directed into the intraconal space. Within 24 hours the pellets expand and the microphthalmic eye and surrounding tissue were pushed anteriorly. Orbital volume augmentation was achieved with this method and a prosthesis was then fit to complete the process.
With skill, dexterity and prompt treatment, the congenital anophthalmic socket can be rehabilitated with an excellent outcome (Fig. 8). As the children grow into their teenage and adult years, they eventually become like the adult acquired anophthalmic patient with the same potential for similar complications.
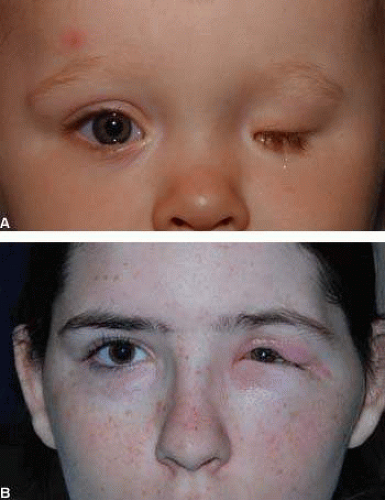 Figure 8. A. Microphthalmic patient without expansion of left socket. B. Three years after hydrogel expander. |
Management of the Acquired Anophthalmic Socket
Although the indications for anophthalmic surgery may vary widely, the post-operative course of patients who undergo successful enucleation, evisceration or exenteration converges in the management of the anophthalmic socket. While the ultimate goal of primary surgery is very patient specific – be it to maintain patient comfort in the case of a blind and painful eye, or to prevent sympathetic ophthalmia after trauma, or to prevent the spread of an intraocular or peri-ocular tumor, the successful surgery also allows the patient to be rehabilitated in a more social sense. The emotional toll of losing an eye may be compounded by more specific concerns relating to the spread of an intraocular or intraorbital infection or tumor. Many patients worry about how the loss of visual field and/or depth perception will affect their life or their ability to work, and concerns about cosmesis – how they will look, how they will be perceived by others – are of great importance to the monocular patient.
The ophthalmologist plays an important role in helping each patient to adjust to the change, but the crucial responsibility is in maintaining the health of the anophthalmic socket. It is imperative to note that eye care providers should always take time to examine the anophthalmic socket as part of a comprehensive exam. Taking the time to ask about problems and to look for them will help maintain the long term health of the anophthalmic socket. The remainder of this chapter will focus on the maintenance of a healthy socket in the adult patient as well as to address some of the common problems that may be encountered in the postoperatively
The Healthy Anophthalmic Socket
Successful anophthalmic surgery results in a socket which is both functionally and aesthetically acceptable for the patient (Fig. 9). Although highly subjective, for the patient who has undergone enucleation or evisceration this end-point entails: (1) an orbital implant that is of sufficient volume to prevent the appearance of enophthalmos; (2) a socket lined with conjunctiva or mucous membrane with fornices deep enough to hold a prosthesis; (3) a prosthesis that sits comfortably in the socket and is customized to enhance symmetry; (4) good transmission of motility from the implant to the prosthesis; and (5) healthy periorbital structures, such as eyelids and lashes, which not only help to support the prosthesis but can also help to camouflage any abnormalities.
 Figure 9. Successful and cosmetically acceptable anophthalmic left socket with porous implant and prosthesis OS. |
The issues implicated in the choice of orbital implant after enucleation or evisceration are beyond the scope of this chapter and have been discussed elsewhere. It will be said, however, that individualization of the implant size is important in optimizing orbital volume replacement and in achieving the best possible aesthetic result.35 An adequately sized implant can also forestall several characteristic postoperative problems, such as an abnormally deep superior sulcus, upper eyelid ptosis, or enophthalmos. These problems can be minimized with a larger-than-desirable prosthesis; however, the weight of larger prostheses often results in progressive lower eyelid laxity and malposition and may limit socket excursion.36 Too large an implant, however, may predispose patients to implant extrusion in the early postoperative period as Tenon’s capsule must be closed with greater tension.37
The Prosthesis
After surgery is completed, it is recommended that a prosthesis be fit 6 to 8 weeks postoperatively. This allows the mucosal incision to heal and for edema to resolve. The ocularist will make a custom mold of the socket along with a match of the iris color and pupil size. Thankfully there are many outstanding ocularists that take pride in their work and understand the nuances of orbital rehabilitation. Their hard work is what makes it possible to achieve a cosmetically superior result. It is difficult as a surgeon to perform a picture perfect enucleation or socket rehabilitation only to see the patient wearing a poorly made prosthesis (Fig. 10a and b).
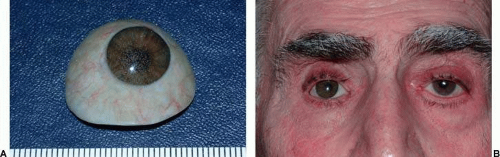 Figure 10. A. Poorly made prosthesis with multiple air bubbles embedded in the prosthesis in front of the “iris.” B. On external view, the eye lacks a normal appearance and draws in attention. |
There is a certain maintenance that is required to perpetuate the health and cosmesis of the eye socket. This is why it is imperative to teach patients how to care for their socket and prosthesis. In general, patients can leave the prosthesis in 24 hr/day and leave it alone as much as possible. That stated, patients should know how to insert and remove the shell. It can be removed to be cleaned in patients with mucus or salt build up on the prosthesis. Otherwise, it can be left in place for the ophthalmologist and ocularist to examine and clean. A prosthesis should be cleaned and polished annually and remade approximately every 7 years. Also, children should have their prosthesis remade more often as they can outgrow the prosthesis during the first 5 to 10 years of life.
Some patients do not like to remove the prosthesis as they are uncomfortable with touching the socket or prosthesis. This unfortunately is a disservice to them. Sometimes the prosthesis will rotate out of position creating an unusual appearance for the patient who otherwise was functioning well. Patients who know how to care for and remove or insert the prosthesis can better help in the general care of the shell. Chronic, continuous wearing of the prosthesis can occasionally cause irritation of the conjunctival socket, especially in the dry eye patient. This can occasionally lead to socket contraction and poor prosthesis retention. Patients in this situation should be monitored more closely and be taught how to care for the socket.
Prosthesis Motility and Implant Coupling after Enucleation or Evisceration
One of the major hurdles to social rehabilitation for the patient after enucleation or evisceration is poor prosthesis movement (Fig. 11). A discussion of implant motility must consider two separate but overlapping paths: first, the evolution of the orbital implant has contributed greatly to improvements in postoperative motility; and second, advances in surgical technique, both in response to these implant changes, and also as a result of a growing understanding of physiology, has allowed surgeons to augment motility like never before.
 Figure 11. Reduced motility in left gaze of a left socket prosthesis. |
Although a complete review of anophthalmic implant history is beyond the scope of this text, some aspects are worth highlighting. The earliest implants were spheres placed within the Tenon’s capsule. The disinserted extraocular muscles were allowed to contract within the socket, contributing minimally to postoperative implant motility. Surgeons then began to advocate suturing the muscles in front of alloplastic spherical implants. This technique only slightly improved motility, however, and there was a tendency for these implants to migrate between the imbricated muscles, especially superotemporally.38 Attempts at changes in implant design, such as grooved implants to reduce migration, and quasi-integrated implants (Allen, Iowa, Universal) that had irregularly shaped surfaces (Fig. 12) to create an indirect coupling mechanism between the implant and prosthesis imparted greater movement to the prosthesis, however were ultimately abandoned due to high complication rates and chronic exposure problems.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


