Over the past 2 decades, there has been a significant increase in the resection of larger and more complex ventral skull base malignancies. The resection of these lesions has resulted in the creation of larger and more difficult to repair skull base defects. There are many available options for ventral skull base reconstruction. Despite the variety of reconstructive options, the key objective is to eliminate any communication between the intracranial space and the sinonasal cavity. This article discusses some of the more common techniques currently used for repair of these skull base defects.
Key points
- •
Recently, the vascularized pedicled nasoseptal flap has emerged as the workhorse for reconstruction of ventral skull base defects after endoscopic skull base surgery. However, for repair of skull base defects after resection of sinonasal and ventral skull base malignancies, extreme care should be taken to assure the flap is not involved with cancer cells.
- •
Although free grafts and single-layer repair techniques have been used to repair large skull base defects, multilayer closure with the inclusion of vascularized tissue may provide a stronger repair option.
- •
If postoperative radiotherapy is expected after resection of a ventral skull base malignancy, the use of vascularized tissue may help decrease the likelihood of dehiscence of the repair during radiotherapy.
- •
In cases where a combined endoscopic and open approach is performed for resection of a malignant ventral skull base lesion, a double-flap technique consisting of a vascularized pericranial flap and a vascularized pedicled nasoseptal flap can be used simultaneously to decrease the chance of failure.
Video content accompanies this article at http://www.oto.theclinics.com .
Introduction
Over the past 2 decades, the management of patients with sinonasal and ventral skull base malignancies has changed with more aggressive surgical resection being performed. One of the main factors facilitating aggressive surgical resection has been the improvement in ventral skull base repair techniques (open transcranial, combined open transcranial and endoscopic endonasal, or purely endoscopic endonasal) with decreasing rates of postoperative cerebrospinal fluid (CSF) rhinorrhea and associated intracranial complications. The decrease in postoperative CSF leak paralleled the emergence of the vascularized pedicled nasoseptal flap (PNSF) as the workhorse for reconstruction of ventral skull base defects after combined and endoscopic endonasal ventral skull base surgery. Some of these ventral skull base defects extend from the cribriform plate to the craniocervical junction in the sagittal plane and orbit to orbit and as far lateral as the infratemporal fossae and middle cranial fossae in the coronal plane, presenting a significant challenge for repair. A tight seal along the entire margin of a ventral skull base defect is necessary for successful repair. Inadequate repair can result in postoperative sequelae, such as CSF leak, meningitis, or intracranial abscess. Hence, it is of utmost importance to use the available repair methods as effectively as possible, with a significant emphasis placed on maximizing the surface area of the grafts used. This review discusses some of the more common techniques currently used for repair of these ventral skull base defects with an emphasis on the senior authors’ (J.A.E. and J.K.L.) preferred closure techniques. As one of the most commonly used options for ventral skull base defect repairs, nuances and pearls on the vascularized PNSF are emphasized in this article.
Introduction
Over the past 2 decades, the management of patients with sinonasal and ventral skull base malignancies has changed with more aggressive surgical resection being performed. One of the main factors facilitating aggressive surgical resection has been the improvement in ventral skull base repair techniques (open transcranial, combined open transcranial and endoscopic endonasal, or purely endoscopic endonasal) with decreasing rates of postoperative cerebrospinal fluid (CSF) rhinorrhea and associated intracranial complications. The decrease in postoperative CSF leak paralleled the emergence of the vascularized pedicled nasoseptal flap (PNSF) as the workhorse for reconstruction of ventral skull base defects after combined and endoscopic endonasal ventral skull base surgery. Some of these ventral skull base defects extend from the cribriform plate to the craniocervical junction in the sagittal plane and orbit to orbit and as far lateral as the infratemporal fossae and middle cranial fossae in the coronal plane, presenting a significant challenge for repair. A tight seal along the entire margin of a ventral skull base defect is necessary for successful repair. Inadequate repair can result in postoperative sequelae, such as CSF leak, meningitis, or intracranial abscess. Hence, it is of utmost importance to use the available repair methods as effectively as possible, with a significant emphasis placed on maximizing the surface area of the grafts used. This review discusses some of the more common techniques currently used for repair of these ventral skull base defects with an emphasis on the senior authors’ (J.A.E. and J.K.L.) preferred closure techniques. As one of the most commonly used options for ventral skull base defect repairs, nuances and pearls on the vascularized PNSF are emphasized in this article.
Repair after open transcranial surgery
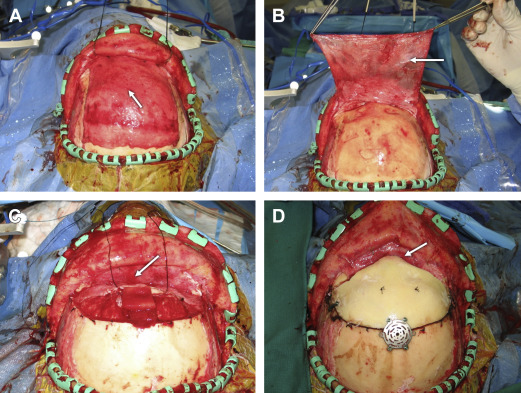
In patients undergoing bifrontal transbasal approaches and craniofacial resection, the vascularized pedicled pericranial flap (PCF) has been the gold standard for repair ( Fig. 1 ). A bicoronal scalp incision is performed from ear to ear and the scalp flap is elevated in a 2-layer fashion. The galeal flap is elevated with the skin as one layer while leaving the pericranium on the skull. Undermining the galea posterior to the skin incision is performed in order to obtain a larger surface area of pericranium. The PCF is subsequently elevated as a second layer and rotated anteriorly where it is pedicled. The transbasal cranial approach is then performed for resection of the sinonasal/ventral skull base malignancy. The frontal sinus mucosa is exenterated and the sinus cranialized. After this approach and resection of the sinonasal and ventral skull base malignancy and the cribriform plate, the dura is typically repaired by suturing a dural patch graft (usually from a dural substitute) to close the intracranial dural defect in a watertight fashion. The PCF is subsequently layered along the floor of the ventral skull base and tucked underneath the dura overlying the planum sphenoidale. Several sutures may be used to anchor the pericranium to the dura in this location. The distal end of the PCF is then folded on itself to provide coverage along the frontobasal dural closure. The closure of the transbasal approach is performed in the standard fashion.
Repair after combined open transcranial and endoscopic endonasal surgery
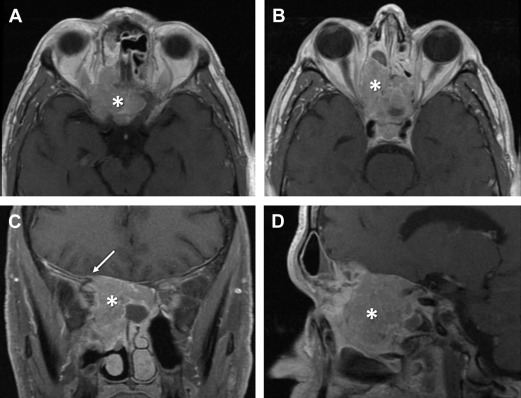
The vascularized PCF is the gold standard for repair after bifrontal transbasal approaches and craniofacial resection. Likewise, the vascularized PNSF has emerged as the workhorse for reconstruction of ventral skull base defects after endoscopic endonasal approaches. In the authors’ practice, they sometimes use a combined bifrontal transbasal approach and endoscopic endonasal approach to resect large anterior ventral skull base malignancies with significant sinonasal and intracranial extension or in some cases with significant neurovascular involvement. For these lesions, postoperative radiation therapy is anticipated, which can predispose patients to delayed flap necrosis and secondary CSF leakage. In these instances, the authors reconstruct the ventral skull base defect using a double-flap repair, which is composed of 2 vascularized pedicled tissue flaps: the PCF harvested from the transbasal approach from above augmented by a PNSF harvested from an endoscopic endonasal approach from below ( Figs. 2–4 ).
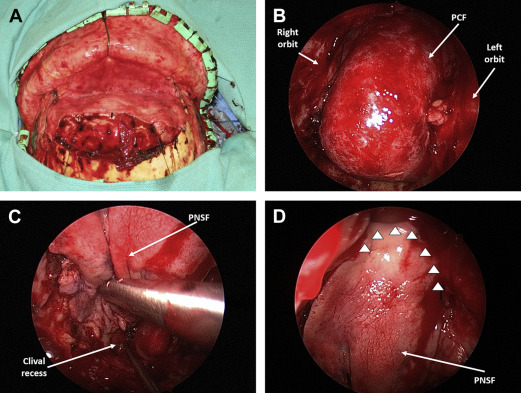
After the open resection of the intracranial portion of the malignancy, the initial dural and ventral skull base defect is repaired using a dural patch and a vascularized PCF as previously described. An endoscopic endonasal approach is then performed from below to remove tumor in the nasal cavity and paranasal sinuses. After complete resection of the intranasal portion of the lesion and achievement of intraoperative negative margins, a vascularized PNSF is harvested from the nasal septum as described by Hadad and colleagues and Kassam and colleagues. As part of the preparation for flap placement, an extended sphenoid sinusotomy (opening and combining the 2 sphenoid sinuses into a single cavity) is typically performed and the sinus mucosa completely removed to prevent the development of intracranial mucocele formation and to allow for proper adherence of the PNSF to the ventral skull base. It is much preferred to use the contralateral PNSF for repair of ventral skull base defects after resection of a sinonasal and ventral skull base malignancy in order to prevent placing a flap involved with cancer in the repair. Frozen section of the PNSF edges should be taken to rule out cancer involvement. In the authors’ institution, they use the ipsilateral PNSF only if no other repair option is available, and when the likelihood of the ipsilateral flap involvement with cancer cell is unlikely. When this has to be performed, they usually harvest the flap as far away from the tumor as feasible and typically involve the mucosa of the hard palate in the flap. The PNSF is rotated to cover the ventral skull base defect endonasally. This endonasal repair is then bolstered with gentamicin-soaked absorbable gelatin sponge pledgets followed by an expandable Merocel (Medtronic Xomed, Jacksonville, Florida, USA) nasal packing. Postoperatively, patients are kept on antibiotics for approximately 10 days until endoscopic removal of the nasal tampon in the outpatient setting.
The combination of the vascularized PCF and PNSF offers several advantages. Each flap complements the other at its weakest point. In a PCF repair alone, the weakest point and likely failure site is the region of the planum sphenoidale at the posterior suture line. The PNSF provides robust coverage of that area to strengthen the PCF’s point of weakness. Conversely, the PNSF’s weakest point is anteriorly near the region of the frontal sinus because of its maximal reach. This fact is particularly true if portions of the PNSF are involved by tumor and need to be excised, which compromises the surface area and reach of the flap. In such a situation, the PNSF’s point of weakness can be bolstered by the PCF because coverage of the cranialized frontal sinuses is quite robust.
Repair after purely endoscopic endonasal surgery
In patients undergoing purely endoscopic endonasal resection of sinonasal/ventral skull base malignancies, repair of the ventral skull base defect can be performed using a variety of donor graft materials (middle turbinate, temporalis fascia, fascia lata, palatal mucosal, septal mucosa), flaps (PNSF, inferior turbinate flap, middle turbinate flap, and so forth), synthetic materials (acellular dermal allograft), and surgical techniques ( [CR] ). Some techniques involve a single-layer closure, whereas others involve the use of a multilayer closure. Some investigators advocate for rigid reconstructive techniques, whereas others think such an option to be unwise. Although still controversial, what has emerged as the most commonly used technique in major endoscopic skull base centers (including the senior authors’ clinical practice) is the use of a multilayer closure with vascularized tissue when available without rigid reconstruction. However, other commonly used techniques are important to discuss.
Single-Layer Acellular Dermal Allograft Reconstruction
Casiano and colleagues have described the endoscopic repair of large ventral skull base defects using a single layer of thick acellular dermal allograft or 2- to 3-ply lyophilized dura. For large defects extending the full length of the anterior ventral skull base (approximately 2 × 3 cm), the lyophilized dura or acellular dermal allograft is tucked at least 1 cm circumferentially between the remaining dura and the orbital roof ( Fig. 5 ). Further discussion of this repair technique is provided in Ghassan Alokby and Roy R. Casiano’s article, “ Endoscopic Resection of Sinonasal and Ventral Skull Base Malignancies ,” in this issue.
Vascularized Pedicled Nasoseptal Flap Reconstruction
Vascularized pedicled nasoseptal flap reconstruction based on ventral skull base regions
The vascularized PNSF has become an essential component for repair of large ventral skull base defects after endoscopic endonasal skull base surgery. The PNSF has become a mainstay technique because of its high success rate based on its ability to be specifically tailored on a case-by-case basis. The dimensions of the PNSF are largely determined by the ventral skull base defect site/size. The ventral skull base can be divided into 5 broad regions: (1) the cribriform region; (2) the planum sphenoidale/tuberculum sellae region; (3) the sella; (4) the clival/odontoid region; and (5) the lateral corridors. Each region requires unique PNSF dimensions to achieve a successful repair. Endoscopic ventral skull base surgery can involve one or more of these regions, creating a large spectrum of potential defects. Fortunately, the versatility of the PNSF allows this repair option to be an almost universal repair material for large and complex ventral skull base defects. Below are specific PNSF designs that are individually fashioned for ideal coverage of each of the 5 distinct regions of the ventral skull base. These designs can be customized/combined based on the regions involved.
Cribriform region
Defects in the cribriform area ( Fig. 6 A ) necessitate a maximization of the PNSF length. To this end, the anterior limit of the PNSF needs to be extended to the limen nasi ( Fig. 6 B). The inferior longitudinal incision is created just deep to the nasal vestibule at the limen nasi. PNSFs with these boundaries may provide sufficient coverage of a standard surgical defect of the cribriform region. When the defect is widened from medial orbital wall to medial orbital wall, full coverage requires a much broader flap; this is accomplished by placing the inferior longitudinal incision underneath the inferior turbinate ( Fig. 6 C) and the superior incision near or up to the level of the nasoseptal angle ( Fig. 6 D).
Planum sphenoidale/tuberculum sellae region
After creation of a planum sphenoidale/tuberculum sellae defect, a long PNSF is required, given that the flap has to lie on the inferior and posterior walls of the sphenoid sinus (clival recess) before arching back onto the planum sphenoidale/tuberculum sellae region ( Fig. 7 ).
Sella region
Coverage of a standard sellar defect requires a relatively shorter flap than the previous two regions. Positioning the anterior vertical incision at approximately the junction of the anterior and middle one-third of the nasal septum provides sufficient flap length to reach the limit of the sellar defect ( Fig. 8 ). Flap width is not an issue, and placing the inferior longitudinal incision at the junction of the nasal floor and nasal septum provides a sufficiently broad flap. There is also no need to place the superior incision as high as the nasoseptal angle.



