The orbit may be frequently involved by sinonasal or ventral skull base malignancy. This involvement bodes a poorer prognosis for survival. Multimodality therapy with surgery and radiation therapy is usually attempted to optimize local control and overall survival. Oncologic surgical resection with negative margins is critical to local control and survival. In the past, any involvement of the orbit was deemed to necessitate orbital sacrifice. However, contemporary studies show that in carefully selected cases, orbital preservation does not adversely impact survival. In addition, novel reconstructive techniques can help minimize complications and optimize functional and aesthetic outcomes.
Key points
- •
Multimodality therapy with surgery and radiation therapy is usually necessary to manage the orbit infiltrated with sinonasal or ventral skull base malignancy.
- •
Surgical resection with negative margins is the cornerstone of management.
- •
In carefully selected situations, orbital preservation does not adversely affect survival.
- •
Imaging and frozen section histopathology are critical in assessing candidacy for orbital preservation.
- •
Appropriate reconstruction of surgical defects is essential to minimize complications and optimize functional and aesthetic outcomes.
Video content accompanies this article at http://www.oto.theclinics.com .
Introduction: orbital involvement in sinonasal and ventral skull base malignancies
Malignancies of the sinonasal cavity and skull base involve the orbit in in 50% to 80% of cases. The incidence of orbital involvement depends on primary tumor site and histopathology, being reported in 62% to 82% of ethmoid tumors and 46% of nasal cavity tumors. Orbital invasion bodes poorer prognosis for overall and disease-free survival and is associated with poorer outcome from salvage surgery. Involvement of the orbit therefore upgrades local tumor stage to at least T3, with invasion of the orbital apex and beyond (T4b) having the gravest prognosis ( Table 1 ).
| Primary tumor (T) | |
| Maxillary sinus, nasal cavity and ethmoid sinus | |
| T3 | Tumor invades floor or medial wall of the orbit |
| T4a | Moderately advanced local disease: tumor invades the anterior orbital contents |
| T4b | Very advanced local disease: tumor invades orbital apex |
Introduction: orbital involvement in sinonasal and ventral skull base malignancies
Malignancies of the sinonasal cavity and skull base involve the orbit in in 50% to 80% of cases. The incidence of orbital involvement depends on primary tumor site and histopathology, being reported in 62% to 82% of ethmoid tumors and 46% of nasal cavity tumors. Orbital invasion bodes poorer prognosis for overall and disease-free survival and is associated with poorer outcome from salvage surgery. Involvement of the orbit therefore upgrades local tumor stage to at least T3, with invasion of the orbital apex and beyond (T4b) having the gravest prognosis ( Table 1 ).
| Primary tumor (T) | |
| Maxillary sinus, nasal cavity and ethmoid sinus | |
| T3 | Tumor invades floor or medial wall of the orbit |
| T4a | Moderately advanced local disease: tumor invades the anterior orbital contents |
| T4b | Very advanced local disease: tumor invades orbital apex |
Diagnosis
The proximity of the orbit to the sinonasal and ventral skull base facilitates tumor infiltration into the eye through many pathways ( Table 2 ). Although diplopia, epiphora, chemosis, visual changes, and proptosis may be present in approximately 50% of cases, the absence of these findings does not rule out tumor invasion. Symptoms can result from orbital compression, nasolacrimal duct obstruction, and true invasion. The periorbita is a robust barrier against invasion. However, once the tumor invades through the periorbita, there are no further barriers to diffuse orbital infiltration. Computerized tomography (CT) of the paranasal sinuses is useful in studying loss of orbital bone and enlargement of fissures and foramina. MRI is superior for delineating orbital soft tissue involvement, and distinguishing retained secretions (eg, in the lacrimal sac) from tumor. However, imaging may not be able to distinguish true periorbital and extraocular muscle invasion from other changes. Peritumoral edema can lead to muscle enhancement, which may be mistaken for muscle invasion. The final determination of orbital involvement is often made intraoperatively on frozen section pathology.
| Route of Extension | Orbital Involvement |
|---|---|
| Direct invasion through bone |
|
| Direct extension through preformed pathways |
|
| Perineural extension |
|
| Subperiosteal or intraperiosteal extension |
|
| Nasolacrimal duct |
|
| Blood borne |
|
Staging of orbital involvement and surgical implications
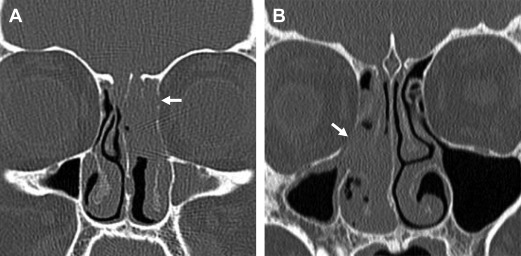
Different systems have been proposed for staging orbital involvement by sinonasal tumors ( Tables 3–5 ). These staging systems attempt to stratify patients along a spectrum of invasiveness. Table 5 proposes a contemporary grading system that can be used for treatment planning. The most minimal form of orbital involvement is rarefaction or focal erosion of the lamina papyracea without transgression of the periorbita ( Fig. 1 ). As tumors progressively invade the orbit, periorbita can become focally or extensively involved with tumor, eventually infiltrating orbital fat ( Fig. 2 ). Ultimately, extraocular muscles can become involved either by focal tumor contact or frank invasion/encasement ( Fig. 3 ). In terms of vision preservation and the need for reconstruction, tumor extension into the nasolacrimal duct/sac and eyelids is particularly relevant ( Fig. 4 ). Adjacency to or invasion of a nerve must be noted preoperatively to counsel patients regarding potential postoperative neurologic deficits and to map out neurotropic cancer spread with MRI ( Fig. 5 ). Invasion of the orbital apex, cavernous sinus, and other intracranial structures will significantly impact resectability and patient outcome ( Fig. 6 ).
| Grade | Criteria |
|---|---|
| I | Erosion or destruction of medial orbital wall |
| II | Extraconal invasion of periorbital fat |
| II | Invasion of medial rectus muscle, optic nerve, ocular bulb, or skin overlying the eyelid |
| Grade | Criteria |
|---|---|
| A | Tumor adjacent the orbit, without infiltration of the orbital wall, which appears thinner |
| B | Tumor eroding the orbital wall without ocular bulb displacement |
| C | Tumor eroding and infiltrating the orbital wall, displacing the orbital wall, without periorbital involvement |
| D | Tumor invading the orbit with periorbital invasion |
| Grade | Criteria | Surgical Approach |
|---|---|---|
| 1 | Tumor adjacent to orbital wall, which may be thinned, bowed, or eroded without periorbital involvement | Orbital preservation is undertaken ( [CR] ) |
| 2 | Tumor eroding orbital wall, with resectable periorbital involvement | Orbital preservation is attempted; periorbita is resected and preservation is likely feasible ( [CR] ) |
| 3 | Tumor with extraocular muscle, intraconal fat, globe, or orbital apex invasion | Orbital clearance is performed |
| 4 | Tumor invading the nasolacrimal system, eyelids duct and/or sac | Orbital preservation may be feasible; reconstruction performed for functional eye |
| 5 | Tumor with cavernous sinus, optic canal or massive intracranial invasion | Unresectable tumor |

Prognosis
An international collaborative analysis of 334 patients with ethmoid malignancies undergoing craniofacial resection found orbital involvement reduced 5-year disease-specific survival from 78.0% to 44.4%. Although survival may not be adversely affected if orbital invasion is limited to the orbital periosteum, orbital apex involvement significantly decreases survival. Tumor histology may affect survival. Nishino and colleagues reported a statistically superior 5-year overall survival rate of 74% for squamous cell carcinoma versus 40% for other sinonasal malignancy invading the orbit.
Management of orbital invasion
A combination of surgery and radiation therapy is used for advanced sinonasal and ventral skull base malignancies with invasion of the orbit. Induction and postoperative chemotherapy also may have a role. Surgery to address orbital disease may require orbital exenteration (complete removal of orbital contents, including the eyelids) or orbital clearance (complete removal of orbital contents with preservation of the lid and palpebral conjunctiva). For the purposes of this article, we use the term “orbital sacrifice” to refer to either.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


