Management of Malignancies of the Ear
Michael J. McKenna
Hinrich Staecker
Malignant tumors of the temporal bone are among the most challenging and difficult clinical problems encountered by otolaryngologists. Although a variety of malignant tumors may develop within or metastasize to the temporal bone, most tumors in this area are squamous cell carcinomas (1, 2, 3). Because these tumors often arise in the setting of chronic infection of the ear canal or tympanomastoid cavity, diagnosis is often delayed until the development of progressive symptoms, which unfortunately correspond with advanced disease and poor prognosis (4, 5, 6, 7, 8, 9, 10). The new onset of pain in the face of chronic infection should immediately raise suspicion of an underlying malignancy. Other risk factors for the development of carcinoma of the temporal bone include a history of prior radiation therapy (11,12).
The most common and readily treatable malignancies of the ear are those involving the auricle and include basal cell carcinoma, squamous cell carcinoma, and malignant melanoma. The risks of developing a cutaneous malignancy of the auricle are the same as for other cutaneous sites and are related to ultraviolet radiation and an underlying hereditary predisposition. The principles of management are also the same, requiring local excision with frozen section control of all margins. If managed properly, the cure rate for squamous cell carcinoma and basal cell carcinoma of the auricle exceeds 95%. The cure rate for malignant melanoma is significantly less, because this tumor tends to metastasize at an early stage. One of the greatest challenges in management of these lesions is often related to the auricular repair following excision (5, 6, 7,13) (Chapter 46).
Malignant lesions in the pediatric population are usually of mesenchymal origin and include rhabdomyosarcoma, neuroblastoma, and histiocytosis (disorders of Langerhans cells). The treatment varies significantly from the epithelial lesions encountered in adults. The primary treatment modalities usually include chemotherapy and radiation therapy, with surgery reserved for biopsy and occasionally for salvage if chemotherapy and radiation therapy fail to control the disease.
Primary malignant lesions of the middle ear and temporal bone in the adult population are almost always of epithelial origin and most commonly are derived from squamous epithelium. However, other epithelial malignancies do occur and include adenocarcinoma and adenoid cystic carcinoma (14, 15, 16, 17). Although the management is fundamentally the same, it is important to keep in mind that lesions of adenoid cystic carcinoma may appear deceptively small based on clinical exam and imaging studies. It is not uncommon for these lesions to extend microscopically far beyond their site of origin and beyond the scope of the planned surgical resection.
EVALUATION AND STAGING OF MALIGNANT LESIONS OF THE EXTERNAL AUDITORY CANAL AND TEMPORAL BONE
Numerous staging systems have been proposed for the staging of malignant tumors of the temporal bone (3,5,7, 8, 9, 10, 14,16,18, 19, 20). Most of these staging systems are based on the location and the degree of extension, which correlates with long-term survival. As more of the temporal bone is involved, the surgical complexities increase and the chance for cure decreases. Figure 40.1 represents a mid-modiolar view of the temporal bone outlining surgical limits for progressively more extensive lesions. In general, lesions can be divided into four categories: (i) Lesions located solely within the external canal can be successfully managed with surgical resection without postoperative radiation, with cure rates of approximately 90%. (ii) Lesions that involve the middle ear cavity and are found to be confined to the middle ear and external auditory canal at surgery are best managed by surgical resection followed by postoperative radiation therapy. Cure rates for these tumors are approximately 50% to 60%. (iii) Lesions of the external auditory canal and tympanomastoid cavity that demonstrate significant bone erosion are best managed by wide surgical resection with postoperative radiation therapy, with cure rates in the range of 20% to 30%. (iv) Lesions that extend beyond the confines of the external canal and middle ear with involvement of the parotid, temporomandibular joint, jugular vein, carotid artery, facial nerve, and labyrinth have a poor prognosis even with surgical
resection, radiation therapy, and chemotherapy. Cure rates for these lesions are in the range of approximately 5%. Lesions that extend intracranially to involve the structures of the posterior fossa or middle fossa are essentially incurable, and treatment should be considered palliative. Surgery and radiation are helpful in controlling symptoms of pain and prolonging survival in these cases (4, 5, 6, 7, 8, 9, 10,13,14,19, 20, 21, 22). Most patients who succumb to malignancies of the temporal bone die from local extension. Regional metastasis is less common than for squamous cell carcinoma in other head and neck locations. Distant metastasis is relatively uncommon.
resection, radiation therapy, and chemotherapy. Cure rates for these lesions are in the range of approximately 5%. Lesions that extend intracranially to involve the structures of the posterior fossa or middle fossa are essentially incurable, and treatment should be considered palliative. Surgery and radiation are helpful in controlling symptoms of pain and prolonging survival in these cases (4, 5, 6, 7, 8, 9, 10,13,14,19, 20, 21, 22). Most patients who succumb to malignancies of the temporal bone die from local extension. Regional metastasis is less common than for squamous cell carcinoma in other head and neck locations. Distant metastasis is relatively uncommon.
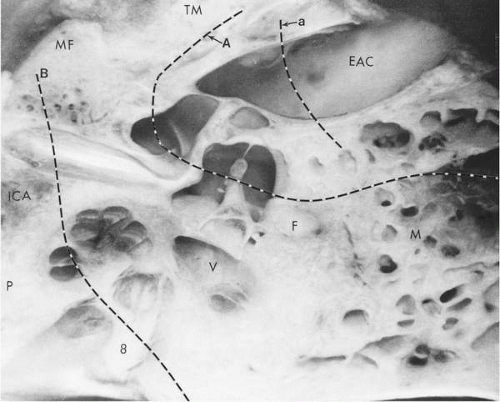 FIG. 40.1 Mid-modiolar horizontal view of a celloidin-embedded temporal bone. The location of medial margins for partial temporal bone resection (A), subtotal temporal bone resection (B), and a subtype of partial temporal bone resection (a) for cartilaginous canal lesions are shown by the broken lines. MF, middle fossa; TM, temporomandibular joint; EAC, external auditory canal; ICA, internal carotid artery; P, petrous apex; V, vestibule; F, facial nerve; M, mastoid antrum; 8, eighth nerve. |
The initial evaluation of patients with suspected malignancies of the temporal bone should include a complete head and neck exam, a cranial nerve exam, and a high-resolution computed tomographic (CT) scan of the temporal bone, brain, and neck with axial and coronal projections. In cases where there is clinical or radiographic evidence of involvement of the middle fossa plate, posterior fossa plate, or the infratemporal fossa, a magnetic resonance imaging (MRI) scan should be obtained. With MRI it may be possible to demonstrate involvement of the dura or intracranial extension, which cannot be appreciated on CT alone. Although distant metastases are relatively uncommon, the patient should undergo a metastatic workup with a chest CT and liver function studies. Audiometry is also routinely obtained.
To establish the correct diagnosis, a representative biopsy must be obtained. If malignancy is suspected and a negative biopsy is obtained, a second biopsy should be taken and should include a deep wedge of tissue at the margin of the lesion and normal-appearing tissue. If necessary, this can be done under general anesthesia, but care should be taken that the biopsy does not compromise or interfere with the planned surgical resection.
A confounding problem in the evaluation of lesions of the external auditory canal is the occasional development of pseudoepitheliomatous hyperplasia, which may occur in the setting of both acute chronic inflammation of the external auditory canal (23). The biopsy of the lesions may be indistinguishable from squamous cell carcinoma even when examined by an experienced pathologist. If the clinical presentation and exam are not consistent with malignancy and
there is no evidence of bone erosion on CT scan, it is our practice to excise these areas of abnormality with wide local excision and to follow these patients closely. Lesions of pseudoepitheliomatous hyperplasia should heal promptly and completely. Delayed healing or lingering epithelial abnormalities are rebiopsied. If the second biopsy again demonstrates what appears to be squamous cell carcinoma, the lesions are managed accordingly. Even if the canal heals completely without evidence of irregularity, it is imperative that the patients continue to be followed by routine otoscopy and follow-up CT scan for several years.
there is no evidence of bone erosion on CT scan, it is our practice to excise these areas of abnormality with wide local excision and to follow these patients closely. Lesions of pseudoepitheliomatous hyperplasia should heal promptly and completely. Delayed healing or lingering epithelial abnormalities are rebiopsied. If the second biopsy again demonstrates what appears to be squamous cell carcinoma, the lesions are managed accordingly. Even if the canal heals completely without evidence of irregularity, it is imperative that the patients continue to be followed by routine otoscopy and follow-up CT scan for several years.
An unfortunate and not uncommon occurrence is the encountering of a malignant tumor at the time of tympanomastoidectomy that had been planned for the management of chronic otitis media. Usually, neither the surgeon nor the patient is adequately prepared. In many instances, imaging studies have not been obtained preoperatively and the extent of disease is not known. This situation is best managed by obtaining a definitive frozen section diagnosis and a simple one-layer closure of the wound. This patient should then undergo a thorough evaluation to determine the extent of the disease process followed by a definitive surgical procedure as early as possible.
SURGICAL INDICATIONS AND PLANNING
Surgical planning is dependent upon the establishment of a reliable tissue diagnosis, the determination of the extent of the disease process based on clinical exam and radiographic imaging, and the age and general health of the patient.
Adjunctive Therapy
Radiation therapy should be planned as postoperative treatment for all cases of squamous cell carcinoma except those lesions limited to the external canal. Radiation therapy is always given as a planned treatment modality rather than reserved for clinical evidence of recurrence. Primary radiation therapy or combinations of chemotherapy and radiation have not been shown to be as effective as surgery with postoperative radiation (7,21,24).
The role of chemotherapy in the management of temporal bone malignancies has not been clearly established. There does not appear to be a role for primary treatment with chemotherapy or for induction chemotherapy prior to planned surgical resection, because this may delay definitive treatment of a potentially curable lesion. Chemotherapy has been helpful in prolonging survival in patients who have incurable or inoperable tumors and in those patients with positive margins following surgical resection. The role of chemotherapy as an adjunctive treatment modality in patients who undergo resection followed by planned radiation therapy has also not been established. This is in large part related to the fact that these tumors are relatively uncommon, and studies to establish the efficacy of chemotherapy require a relatively large number of patients.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


