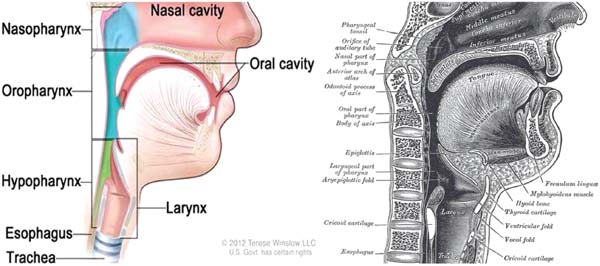
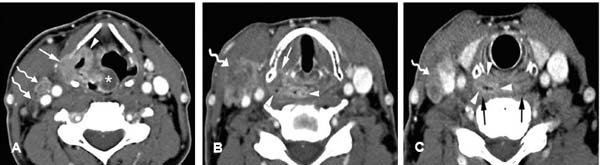
13 Core Messages • A multidisciplinary approach is necessary to devise an appropriate therapeutic algorithm. • Prognosis of cancer of the hypopharynx is associated with less favorable survival outcomes than that of other head and neck malignancies because of high incidence of submucosal involvement and cervical lymphatic spread at the time of presentation. • Computed tomography, magnetic resonance imaging, and positron emission tomography are the recommended imaging modalities in the diagnostic and preoperative work-up. In addition, they are indicated for the detection of locoregional recurrence and persistent disease and the assessment of treatment response. • Clinical staging generally guides treatment. Preservation of function, quality of life, and toxicities of treatment should all be considered when selecting an optimal treatment regimen. Surgery, radiation therapy, and chemotherapy all have an important role in management. • Biological agents such as cetuximab show promise as an adjunctive treatment of hypopharyngeal squamous cell carcinomas. Randomized prospective clinical trials demonstrating efficacy in comparison to standard chemoradiotherapy regimens are necessary to further define a potential role for cetuximab. Management of hypopharyngeal cancer poses a unique and difficult challenge to physicians. Because of the central location of the hypopharynx, its relation to several critical anatomic structures, and its integral role in swallowing, speech, and phonation, the management of hypopharyngeal cancer demands special attention. A collaborative effort between head and neck surgery, radiation, and medical oncology is often necessary to maximize both survival and quality of life. Furthermore, great care must be taken in the planning, management, and follow-up of these patients, as there are formidable reconstructive and functional challenges posed by surgical intervention and other treatment-related morbidities and impairments. Carcinomas of the hypopharynx are rare in comparison to other head and neck cancers (HNCs), comprising only 4.3% of all head and neck malignancies.1 Roughly, 2500 new cases of hypopharyngeal cancer are diagnosed in the United States each year.2 Moreover, the incidence of laryngeal cancer is four to five times higher than that of hypopharyngeal cancer. The overwhelming majority of hypopharyngeal malignancies are of epithelial origin. Approximately 95% are squamous cell carcinomas (SCCs), and thus they are the primary focus of this discussion. There is a clear gender difference, as men are more likely to develop hypopharyngeal cancer, particularly those of African American descent. In fact, a 3:1 male-to-female ratio has been demonstrated in the United States. However, there exists a subset of female patients with Plummer-Vinson syndrome who are more susceptible than men to develop hypopharyngeal cancers—specifically of the postcricoid area.3 Epidemiologic studies have also demonstrated a correlation between increased age and increased incidence of malignancy. The mean age of presentation is 65 years. As with other SCCs of the head and neck, hypopharyngeal cancers have a strong association with both chronic alcohol and tobacco use. Recently, seropositivity for human papillomavirus subtype 16 has been identified as an independent risk factor for head and neck SCCs.4 It should also be noted that very rarely (< 5%) hypopharyngeal cancers present as adenocarcinomas, lipomas, melanomas, or lymphoproliferative malignancies such as angiocentric T-cell lymphoma, non-Hodgkin lymphoma, and mucosa-associated lymphoid tissue. Other rare types of hypopharyngeal carcinomas include basaloid squamoid carcinomas, spindle cell carcinomas, small cell carcinomas, nasopharyngeal-type undifferentiated carcinomas, and carcinomas of the minor salivary glands.5 Cancer of the hypopharynx is often a devastating disease with a poor prognosis. Although these cancers are generally aggressive and poorly differentiated, the early stages of disease are often clinically silent. At the time of presentation, most patients already have extensive submucosal spread and a high incidence of cervical lymph node metastasis: roughly 70 to 80% of the patients initially present with stage III or IV disease.1,6 The overall 5-year survival rate is approximately 30% for patients with carcinoma of the hypopharynx.1 The anatomic boundaries of the hypopharynx can be conceptualized as the region between the oropharynx and the esophageal introitus (Fig. 13.1). More precisely, the hyoid bone constitutes the superior border of the hypopharynx, which extends inferiorly to the cricoid cartilage at the most inferior aspect. The cricopharyngeus delineates the transition point of the pharynx to the cervical esophagus. Of note, the hypopharyngeal region excludes the larynx. Indeed, the anterior wall of the hypopharynx is bounded by the posterior surface of the larynx while the retropharyngeal space denotes the posterior border of the hypopharynx. Because of the anatomic proximity of the larynx and the hypopharynx, the larynx is vulnerable to invasion by neoplastic processes of the hypopharynx.7 Furthermore, this anatomic distinction between the larynx and the hypopharynx offers clinical relevance. Although only millimeters apart, the low metastatic potential and high curability of laryngeal cancers dramatically contrast the early dissemination and poor prognosis of stage-matched hypopharyngeal cancers.8 Conceptually and clinically, the hypopharynx anatomy is subdivided into three distinct regions: pyriform sinuses, postcricoid area, and the posterior pharyngeal wall. Approximately, 65 to 85% of hypopharyngeal cancers arise from the pyriform sinus, 10 to 20% from the posterior pharyngeal wall, and 5 to 15% from the postcricoid area.9,10 The pyriform sinuses are bilateral recesses on each side of the larynx bounded superiorly by the pharyngoepiglottic folds and inferiorly by the cricoid cartilage. These anatomic boundaries form an inverted pyramidal-shaped space. Deep to the mucosa of the pyriform sinus lie both the recurrent laryngeal nerve and the internal laryngeal nerve, which is a branch of the superior laryngeal nerve. Laryngeal invasion has been noted with tumors of the pyriform sinus with medial extension.11 The posterior pharyngeal wall extends from the level of the hyoid bone superiorly to the uppermost aspect of the cricopharyngeus inferiorly. Tumors of this hypopharyngeal sublocale may extend into the prevertebral tissue, as this area is only posteriorly confined by a potential retropharyngeal space before abutting the vertebral and paravertebral anatomy.12 The postcricoid region forms the anterior wall of the hypopharynx and extends from the posterior surface of the arytenoid cartilages superiorly to the cricoid cartilage inferiorly. The postcricoid area connects the paired pyriform sinuses. Although a rare location for hypopharyngeal carcinoma, tumors of the postcricoid region have a tendency to involve the recurrent laryngeal nerve, paratracheal nodes, and thyroid because of a close anatomic relationship with the medially situated tracheoesophageal groove.12 The hypopharynx has an extensive lymphatic drainage network that exits superiorly via the thyrohyoid membrane and drains primarily into the jugulodigastric and mid-jugular (level III) lymph node chains. There is an additional drainage from the spinal accessory, retropharyngeal, paratracheal lymph nodes as well as the paraesophageal lymph nodes within the supraclavicular fossa. Different regions of the hypopharyngeal anatomy receive different lymphatic drainage, thus influencing the different yet characteristic patterns of dissemination of metastatic disease for each sublocale. At presentation, bilateral paratracheal lymphadenopathy is commonly found among patients with metastatic disease. In general, the pyriform sinus primarily drains to the upper (level II) and mid (level III) jugular chains, posterior cervical nodes, and retropharyngeal nodes. The posterior hypopharyngeal wall receives similar drainage to the mid-jugular and retropharyngeal nodes. Finally, the mid and lower jugular chains as well as the paratracheal lymph nodes receive lymph flow from the postcricoid area.13 Figure 13.1 Anatomy of the hypopharynx—sagittal view. Adapted from: PDQ® Hypopharyngeal Cancer Treatment, Bethesda, MD, National Cancer Institute (left) and 20th U.S. edition of Gray’s Anatomy of the Human Body (right). http://cancer.gov/cancertopics/pdq/treatment/hypopharyngeal/HealthProfessional. The act of deglutition is a key function of the hypopharynx and is coordinated by both sensory and motor input of the glossopharyngeal and vagus nerves that contribute to the pharyngeal plexus. The motor innervation of the hypopharynx is predominantly vagal. The superior and middle pharyngeal constrictors receive motor input via the superior pharyngeal nerve and the pharyngeal branches of the vagus, while the inferior pharyngeal constrictor receives innervation from the external and recurrent branches of the vagus nerve. With regard to sensory innervation, the internal laryngeal branch of the superior laryngeal nerve traverses the lateral wall of the pyriform sinus and the thyrohyoid membrane, where it merges with the vagus nerve.5,12 Of note, the phenomenon of referred otalgia that comprises part of the classic symptom triad (see the section on Patient Evaluation) for patients with hypopharyngeal cancer results from cross-innervation at a common point of synapse. The sensory portions of the internal laryngeal branch of the superior laryngeal nerve synapse on the jugular ganglion along with sensory nerves of the external auditory canal (Arnold nerve, a division of the vagus), leading to symptoms of referred otalgia. The superior thyroid arteries form the main arterial supply of the hypopharynx with collateral supply via the lingual and ascending pharyngeal arteries. The venous drainage follows that of the arterial supply.5,12 Patients with cancer of the hypopharynx classically present with a triad of symptoms: chronic throat pain, referred otalgia, and progressive dysphagia. Dysphagia often starts with solids and progresses to inability to tolerate liquids, which eventually results in malnourishment. Symptomatology of hoarseness and airway obstruction are generally indicative of laryngeal nerve involvement or paralysis. Specifically, small tumors of the postcricoid area have been known to present with a foreign body sensation in the throat. Weight loss, hemoptysis, and laryngeal stridor generally present later in the disease course. As previously mentioned, hypopharyngeal cancer is often clinically silent until more advanced stages of disease. A retrospective study by Hoffman et al reported that more than one-third of the patients with stage I or II disease were asymptomatic at presentation. In addition, gastroesophageal reflux was the second most common presenting symptoms among patients with stage I or II disease.14 Among symptomatic patients with stage III or IV disease, the most common presenting symptom was an asymptomatic neck mass. Palpable lymphadenopathy was present in up to 70% of the patients with pyriform sinus lesions upon initial presentation. Of note, a large majority (62.7%) of patients with advanced disease also presented asymptomatically. It should be noted that the prevalence of distant metastases among patients with hypopharyngeal cancers is among the highest for all HNCs. It has been reported that up to 60% of hypopharyngeal SCCs have spread to regional nodes at the time of diagnosis and as many as 17% may be associated with distant metastases when clinically diagnosed.15,16 An extensive work-up is requisite for a patient presenting with suspected hypopharyngeal cancer. The initial evaluation should involve a thorough history and physical examination, with emphasis on the head and neck examination. The neurologic examination and assessment of palpable cervical and supraclavicular lymphadenopathy should also be key components of the physical examination. The next step is visualization of the lesion. Currently, flexible laryngoscopy is the modality of choice for visualization of the mucosal anatomy and airway. The assessment of the integrity of the vocal cords for signs of fixation or impaired mobility is important because vocal cord involvement is part of the clinical staging work-up; furthermore, recognizing signs impending airway compromise can be lifesaving. Indirect laryngoscopy or indirect mirror examination are viable alternatives. Triple endoscopy (nasopharyngolaryngoscopy, esophagoscopy, and bronchoscopy) with biopsy under anesthesia should be performed for definitive tissue diagnosis. With cancers of unknown primary site, directed biopsies of the nasopharynx, the hypopharynx, and the base of the tongue, as well as ipsilateral or bilateral tonsillectomy, should be performed.17 However, fine-needle aspiration should be the first diagnostic step if neck lymphadenopathy is present. In general, core biopsy is contraindicated, as it may be detrimental to later therapeutic surgical intervention. The use of the barium swallow study as a diagnostic test has decreased in popularity, but it may still be used if the lesion prevents endoscopic examination. In addition, it is used postoperatively to examine residual deglutition function as well as to assess for gross anatomic defects such as strictures and fistulae. Subsequent to the establishment of a biopsy-proved diagnosis, the pretreatment work-up ensues to define local and regional extent of the disease. Cancer of the hypopharynx is staged clinically. Standard imaging involves chest X-ray, computed tomography (CT) with contrast, and/or magnetic resonance imaging (MRI) with contrast of the primary tumor, oral cavity, and neck. CT and MRI both offer unique advantages and the study of choice is based on clinician preferences. CT is superior in the assessment of cartilage and bone invasion, while MRI is a better study to assess soft-tissue involvement (Fig. 13.2). In addition, those patients with suspected or proven advanced stage III or IV disease should be considered for positron emission tomography-computed tomography (PET-CT) imaging. PET scanning is also a useful imaging modality for the evaluation of unknown primaries as well as treatment response and when MRI or CT yields equivocal results. The metastatic work-up is completed with relevant laboratory studies (complete blood count, liver function tests [LFTs], blood urea nitrogen-to-creatinine ratio, prothrombin time/partial thromboplastin time, basic metabolic profile, thyroid stimulating hormone [TSH]) and additional imaging based on clinical suspicion. Finally, the patient should undergo pretreatment anesthesia studies and surgical clearance. In addition, nutrition, speech and swallowing evaluation, and pulmonary function testing should be sought as indicated, as well as a formal dental evaluation, which is mandatory before the initiation of radiotherapy. Planning for posttreatment morbidities must be anticipated. The majority of patients undergoing chemoradiotherapy should have prophylactic placement of a feeding tube or consideration for a percutaneous gastrostomy tube. The patient population presenting with cancers of the hypopharynx generally have significant morbidities related to chronic alcohol and tobacco use. Extensive work-up of comorbidities such as cardiovascular disease, chronic obstructive pulmonary disease, liver dysfunction, and malnutrition should be done preoperatively to determine whether a patient is a surgical candidate. Therefore, great care should be taken during preoperative assessment and optimization to reduce perioperative and postoperative complications and morbidities. Figure 13.2 Axial contrast-enhanced computed tomography image of a T4aN2b pyriform sinus lesion. (A) Supraglottic level. The soft tissue mass invades the paraglottic space and extends through the thyrohyoid membrane into the extralaryngeal tissues. Asterisk denotes thickened right aryepiglottic fold. (B) Glottic level. Between the thyroid and the arytenoid cartilage, tumor extends into the true vocal cord (arrow). Bulky disease in the apex of the pyriform sinus showing midline extension (arrowheads). (C) Subglottic level. Retrocricoidal tumor extension (arrowheads). Curved arrows denote adenopathy. Adapted from: Hermans R. Staging of laryngeal and hyperharyngeal cancer: value of imaging studies. Cancer Imaging 2008;8:S94–S107.
Management of Hypopharynx Cancer
Anatomy
Patient Evaluation
Management of Hypopharynx Cancer
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


