Management of Bell’s Palsy and Herpes Zoster
Bruce J. Gantz
Brian P. Perry
New information concerning the etiology of the most common causes of facial paresis or paralysis is altering our management of these disorders. It is now known that neurotropic viruses are important etiologic factors in both Bell’s palsy and Ramsay Hunt syndrome. Herpes simplex virus type 1 has been identified in idiopathic facial paralysis or Bell’s palsy, and herpes zoster virus has been isolated in Ramsay Hunt syndrome. The identification of a viral etiology in these two disorders allows the clinician to more effectively tailor management strategies and improve outcome as new antiviral medications are developed. This chapter will review the pathophysiology, diagnosis, and newer management algorithms for Bell’s palsy and Ramsay Hunt syndrome.
PATHOPHYSIOLOGY
Bell’s Palsy
As first proposed by McCormick in 1972 (1), the herpes simplex virus has recently been shown to be the etiologic agent of Bell’s palsy (2, 3, 4). Using the polymerase chain reaction, herpes simplex virus type 1 (HSV-1) DNA has been identified in the saliva of patients with Bell’s palsy (3), as well as in the geniculate ganglion of a patient who died shortly after the onset of Bell’s palsy (2). The HSV-1 DNA has also been isolated in endoneurial fluid of patients undergoing facial nerve decompression for Bell’s palsy, whereas it was not isolated in control patients undergoing facial nerve decompression procedures for other indications (4). Sugita et al. (5) and Carreno et al. (6) have designed animal models for Bell’s palsy. Sugita et al. inoculated the ear (or tongue) of mice with HSV-1, demonstrating ipsilateral facial paralysis 6 days later. HSV-1 antigens were identified in both the facial nerve and nucleus following animal sacrifice. Using a rabbit model, Carreno found similar pathologic changes within the facial nerve and geniculate ganglion (edema, inflammatory cell infiltrates, vacuolar degeneration) without the associated facial paralysis.
It has been suggested that Bell’s palsy begins with viral involvement of the sensory fibers followed by the motor fibers of the facial nerve, consistent with the idea that the disease is a herpes viral geniculate ganglionitis (7). The neural injury is thought to be secondary to edema within the nerve induced by the viral infection. Three factors determine the extent of injury: the size of the fallopian canal, the anatomy of the meatal foramen, and the degree of edema. The meatal foramen is the narrowest portion of the fallopian canal (0.68 mm) (8), with varying degrees of inclination from the labyrinthine segment to the geniculate ganglion. Contributing to the constriction at the meatal foramen is a tight band of arachnoid tissue that is adherent to the nerve at this location. Based on these findings, Fisch and Felix (9) first proposed that the facial nerve was entrapped at the meatal foramen as a result of edema leading to ischemia and subsequent wallerian degeneration. Intraoperative conduction studies have confirmed this theory (10).
A range of injuries occurs within the facial nerve fibers, from simple conduction block (neuropraxia) to axoplasmic disruption (axonotmesis) and neural tubule disruption (neurotmesis). The different degrees of nerve injury are helpful in differentiating the severity of the neural injury. Neuropraxia results in blockage of propagation of neural impulses, but the injury is not severe enough to induce neural degeneration (wallerian degeneration) distal to the injury. If a nerve that is in a stage of neuropraxia is stimulated distal to the injury, propagation of an electrically applied stimulus distal to the lesion can occur. In axonotmesis and neurotmesis, wallerian degeneration occurs distal to the injury, preventing electrically applied conduction. Electrodiagnostic testing is able to differentiate between neuropraxia and axonotmesis/neurotmesis but cannot distinguish between axonotmesis and neurotmesis. Nerves that have an axonotmesis type injury alone may achieve a complete return of facial function because the neural tubule remains intact. Neurotmesis, on the other hand, is a more severe injury, including disruption of neural tubules resulting in misdirection of healing fibers,
leading to synkinesis and incomplete return of function. The rate of progression of wallerian degeneration, and therefore the rapidity of degeneration on electrical testing, provides useful information about the percentage of fibers undergoing neurotmesis (11). Nerves that degenerate slowly over 10 to 14 days are less likely to exhibit neurotmesis, whereas nerves that degenerate within 3 to 7 days most likely have undergone neurotmesis (11).
leading to synkinesis and incomplete return of function. The rate of progression of wallerian degeneration, and therefore the rapidity of degeneration on electrical testing, provides useful information about the percentage of fibers undergoing neurotmesis (11). Nerves that degenerate slowly over 10 to 14 days are less likely to exhibit neurotmesis, whereas nerves that degenerate within 3 to 7 days most likely have undergone neurotmesis (11).
Ramsay Hunt Syndrome
In 1907 Ramsay Hunt suggested that the combination of facial paralysis and vesicular eruption of the ear was due to a geniculate ganglionitis. Since that time it has been shown that herpes zoster oticus is a polycranial neuronitis, induced by the reactivation of the virus. The varicella zoster virus remains latent within the cerebrospinal ganglion cells after primary infection with chicken pox during childhood (12). Deterioration of specific cellular immunity to the varicella virus is thought to be the trigger for reactivation (13). Wackym (14) demonstrated the presence of the varicella zoster virus (VZV) within the geniculate, spiral, and Scarpa’s ganglia, as well as within the organ of Corti and macula of the saccule, in a patient with Ramsay Hunt syndrome and sudden hearing loss. Others, using the polymerase chain reaction, have shown the presence of the VZV in the oropharynx of patients with herpes zoster oticus and zoster sine herpete (15). Unlike Bell’s palsy, in which the neural injury is secondary to edema and subsequent ischemia, the VZV invades the neuronal soma, leading to cell death (16,17) and a much more guarded prognosis.
DIAGNOSIS
Bell’s Palsy
The acute onset of facial weakness or paralysis, occasionally associated with otalgia, hyperacusis, and dysgeusia without any additional findings, is classic for Bell’s palsy. There is no side or gender predilection, and the annual incidence is 17 to 19 per 100,000 population (18). The occurrence of Bell’s palsy during pregnancy is 3.3 times that for agematched nonpregnant women (18). Peitersen (19) identified a 70% rate of complete paralysis and 30% rate of incomplete paralysis; usually the facial paresis progresses rapidly to facial paralysis in less than 48 hours.
The history and physical examination should be dedicated to making the diagnosis of Bell’s palsy one of exclusion. A history of facial twitching or a slowly evolving paresis should be considered presumptive evidence of a tumor. Although both recurrent and bilateral facial paralyses can be due to Bell’s palsy (HSV-1), their existence places the burden of proof upon the clinician, and imaging should be performed. Most patients begin to demonstrate the first signs of recovery within 3 weeks of onset, and nearly all patients have some return of function by 6 months (19). If some recovery of facial function has not occurred by 6 months, imaging is necessary to exclude a neoplasm. With the exception of the facial paralysis, the head and neck examination should be normal; occasionally one will identify loss of papillae on the ipsilateral tongue due to chorda tympani involvement. Audiologic evaluation often demonstrates a loss of the ipsilateral stapedial reflex with normal pure tones and speech discrimination.
Perhaps the most important aspect of the evaluation of a suspected case of Bell’s palsy is electrodiagnostic testing. The combined use of electroneurography (ENoG) and voluntary contraction electromyography (EMG) can determine the extent of neural injury and provide prognostic information necessary for management decisions. ENoG, as originally described by Esslen (20), can differentiate between a conduction block (neuropraxia) and wallerian degeneration (axonotmesis/neurotmesis). Due to the delay in wallerian degeneration reaching the stylomastoid foramen (the site of electrodiagnostic stimulation), ENoG is not performed until 3 days after the onset of complete facial paralysis. It has been shown that degeneration of 90% or more of the nerve fibers within 14 days of the onset of the paralysis is associated with an incomplete recovery in more than 50% of cases (21). If this level of degeneration is not achieved within 3 weeks after onset of paralysis, the patient has an excellent prognosis for complete return of function. The rapidity of degeneration also has prognostic value; the more quickly one reaches complete electrical degeneration, the more severe the injury (11). The frequency of electrodiagnostic testing is therefore based on the percent degeneration given the duration of paralysis (Fig. 37.1).
Those patients who exhibit complete degeneration on ENoG should also undergo a voluntary evoked EMG to identify a false-positive ENoG result or deblocking phenomenon. Voluntary evoked EMG involves asking the patient to make a forceful facial contraction with EMG electrodes in place. Deblocking is the phenomenon in which asynchronous neural firing due to regeneration of axoplasmic flow fails to generate a surface, compound muscle action potential (CMAP). Any motor activity on voluntary evoked EMG testing indicates “deblocking” of the conduction block and subsequently a favorable prognosis. Poor prognosticators include electrical silence and fibrillation potentials.
Ramsay Hunt Syndrome
Herpes zoster oticus usually presents with severe otalgia, a vesicular eruption, and facial paralysis. The vesicles typically occur on the tympanic membrane, external auditory canal, conchal bowl, and the postauricular region; however, they may also present on the palate and pharyngeal mucosa. Unlike Bell’s palsy, multiple cranial neuropathies are commonplace with the varicella zoster virus. The eighth cranial nerve is most commonly involved with associated sensorineural hearing loss and vertigo. Involvement of the cornea may also occur, necessitating prompt ophthalmologic consultation.
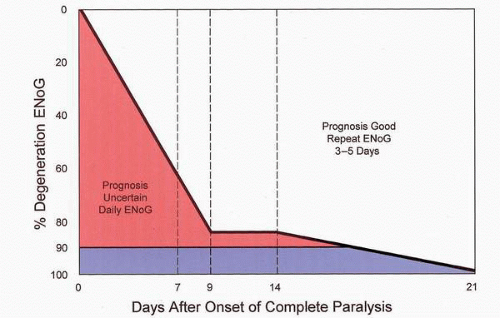 FIG. 37.1 ENoG retest protocol. The pink area represents an uncertain prognosis, and daily ENoG testing is recommended. The blue area indicates 90% degeneration, suggesting severe degeneration. |
Ancillary testing, with the exclusion of an audiogram, is unnecessary. Electronystagmography (ENG) performed in the acute setting will be dominated by the underlying spontaneous nystagmus, which occurs with eighth nerve involvement. Persistent dysequilibrium months later may necessitate an ENG to document caloric weakness prior to initiation of vestibular rehabilitation. Electrical testing has demonstrated variable results in herpes zoster oticus, which may be due to the multiple regions of neural injury in this disorder, in contrast to the single site of injury in Bell’s palsy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


